
Abstract
Objective: To review the frequency as well as the pros and cons of telephone and video-enabled telemedicine during the first 9 months of the Coronavirus disease 2019 (COVID-19) pandemic as experienced by safety net providers across New York State (NYS).
Methods: Analysis of visits to 36 community health centers (CHCs) in NYS by modality (telephone vs video) from February to November 2020. Semi-structured interviews with 25 primary care, behavioral health, and pediatric providers from 8 CHCs.
Findings: In the week following the NYS stay-at-home order, video and telephone visits rose from 3.4 and 0% of total visits to 14.9 and 22.3%. At its peak, more than 60% of visits were conducted via telemedicine (April 2020) before tapering off to about 30% of visits (August 2020). Providers expressed a strong preference for video visits, particularly for situations when visual assessments were needed. Yet, more visits were conducted over telephone than video at all points throughout the pandemic. Video-specific advantages included enhanced ability to engage patients and use of visual cues to get a comprehensive look into the patient's life, including social supports, hygiene, and medication adherence. Telephone presented unique benefits, including greater privacy, feasibility, and ease of use that make it critical to engage with key populations and as a backup for when video was not an option.
Conclusions: Despite challenges, providers reported positive experiences delivering care remotely using both telephone and video during the COVID-19 pandemic and believe both modalities are critical for enabling access to care in the safety net.
Introduction
The Coronavirus disease 2019 (COVID-19) pandemic has catalyzed profound transformations across the health care delivery system, including an abrupt shift toward telemedicine. While telemedicine has been around for decades, low reimbursements and regulatory restrictions stymied its growth. Early in the pandemic, policymakers and insurers introduced several measures to broaden access to telemedicine, including relaxing privacy regulations, increasing reimbursements, coverage for audio-only visits, expanding coverage for services, and lifting geographic restrictions limiting where telemedicine services could be delivered.1⇓–3 These changes helped accelerate the shift toward telemedicine—nearly half of all Medicare primary care visits were provided via telemedicine in April 2020, representing a 350% increase in visits from pre-pandemic levels and signifying a tectonic shift unlikely to be reversed.4
Digital technologies such as telemedicine have the potential to drive major improvements in health care delivery by reducing inefficiencies, improving access, reducing costs, and increasing quality of care.5 Telemedicine, a subset of telehealth, refers to the use of electronic information and communication technologies to provide health care when distance is a barrier.6 Although telemedicine includes the use of asynchronous tools, such as electronic messaging and patient monitoring, of particular benefit during a pandemic requiring social distancing are synchronous telemedicine modalities such as videoconferencing and telephone that take the place of face-to-face visits. Such remote visits may facilitate much-needed access to care while minimizing the risk of exposure for patients, providers, and the surrounding community—a feature that may be especially beneficial for historically underserved, low-income communities that have been disproportionately affected by COVID-19.
Yet, when it comes to equity in access, telemedicine presents a double-edged sword. On the 1 hand, telemedicine visits can make care more convenient and accessible by removing physical barriers such as distance or transportation costs.7 On the other hand, some telemedicine modalities, such as videoconferencing, entail using digital tools and technologies that may not be equally accessible to all patients.8 COVID-19 has further exposed dramatic inequities in technology access and utilization, compounding socioeconomic and racial disparities in health equity. Studies conducted early in the pandemic suggest that sociodemographic characteristics are associated with patient participation in video-enabled telemedicine.9–10 For example, in a study of 15 integrated health systems in Boston, researchers found lower use of video versus telephone visits among older, Black, Hispanic, and Spanish-speaking patients, suggesting that audio-only telemedicine plays a crucial role in securing access for vulnerable populations in a post-pandemic world.11 Similarly, a cohort study of 1162 patients at a large, urban tertiary care center found that socioeconomic characteristics, such as median household income and insurance status, were associated with a patient's participation in telemedicine.12
Although research comparing telemedicine modalities are rare, prior studies found that videoconferencing may be superior to audio-only care because the ability to see patients can provide useful clinical context or help build rapport and reassurance, improving patient-provider communication.13⇓–15 As a result, video-enabled telemedicine has been established as the de facto standard alternative to face-to-face care during the pandemic, with an expanded reimbursement policy for telemedicine significantly favoring video-enabled visits over audio-only communication.10,16⇓⇓⇓–20 The digital divide, coupled with differences in reimbursements, may pose added obstacles for providers in the safety net, especially as it relates to the use of different telemedicine modalities to maintain critical access to care for underserved populations.
The principal aims of this study are to describe the transition to and ongoing use of telemedicine to meet the needs of safety-net patients during the COVID-19 pandemic and examine provider perspectives about the comparative benefits and challenges of video-enabled and audio-only telemedicine visits to deliver care in the safety net. To address these aims, we conducted interviews with 25 primary care, behavioral health, and pediatric providers from 8 Community Health Centers (CHCs) associated with the Community Health Care Association of New York State (CHCANYS). Interview questions centered on the providers' experience delivering telemedicine during the pandemic, with an emphasis on comparing the benefits and pitfalls of video versus telephonic care. In addition, we tracked the use of different care modalities (telephone, video, in-person) across 36 CHCs in New York State (NYS), an early epicenter in the United States, in the months before and during the height of the COVID-19 pandemic.
CHCs play a critical role in serving populations and communities disproportionately impacted by COVID-19. CHCs deliver comprehensive primary care to more than 25 million people across the United States, providing access to many who otherwise may not be able to afford care.21 Understanding providers' perspectives of the use of telephone and video visits in CHCs during an emergency is important because these providers represent a key point of access in underserved communities. Safety-net providers are not simply a stakeholder in the process of telemedicine adoption; they exercise a dominant influence on how telemedicine is actualized and experienced by patients. Findings from this study can inform policies surrounding the use of telemedicine and the design of telemedicine platforms that are more responsive to the needs of safety-net providers and the patients they serve.
Methods
Study Setting
CHCANYS is a membership organization that represents the more than 70 CHCs of New York State.22 CHCANYS represents a diverse group of CHCs, ranging from large metropolitan community health systems in New York City to rural health centers in Upstate New York and Western New York. Each CHC is unique in its size and geographic reach. Some CHCs have multiple sites within a larger system that serves different areas of New York State, while others consist of 1 site.
Quantitative Data
CHCANYS collected data from standard electronic health record reports from January to November 2020 on visits completed by modality (video vs telephone) from 36 CHCANYS health centers. Estimates of total visits have been posted elsewhere.23 We present percentages of total visits by visit modality in 2-week intervals from February to October 2020.
Qualitative Data
In collaboration with CHCANYS, we selected 7 sites to represent the population of CHCs across New York State. The criteria included health centers that varied by region of the state, size (small, medium, and large), setting (urban and rural), and included key subpopulations such as intellectual and developmental disabilities (I/DD); migrant/seasonal farmworkers; homeless; and lesbian, gay, bisexual, transgender, and queer+ (LGBTQ+). Two of the 7 prospective health centers declined to participate, and 3 additional health centers were added to the list of prospective health centers. The remaining 8 CHCs were recruited for this study in collaboration with CHCANYS. The characteristics of the 8 participating CHCs are shown in Table 1. The recruited CHCs serve urban, suburban, and rural areas. Many of the CHCs serve subpopulations, including migrant/seasonal farmworkers, persons experiencing homelessness, immigrants, and individuals living with HIV. A significant percentage of patients at the CHCs are insured through Medicaid. The racial/ethnic diversity of patients at the sites varies widely, with some sites serving mostly Black and Hispanic patients and others serving mainly White patients. Of the 8 CHCs, 5 had some degree of experience with telemedicine before COVID-19.
Characteristics of Participating Sites in Study of Community Health Center Providers' Experience of a Transition to Telemedicine During COVID-19—October to November 2020
The contact persons at the participating CHCs identified providers from 3 clinical services: adult primary care (family medicine and internal medicine); pediatrics; and behavioral health who they thought would be interested in participating in the study. In total, 27 providers were identified as potential participants. Two providers declined to participate. A total of 25 providers were interviewed using semi-structured interview guides that were developed in collaboration with CHCANYS. The guides were pilot tested on 2 interviews and modified slightly following the pilot tests. Each interview was conducted by 2 interviewers from the research team using video or audio calls and was professionally transcribed. Interviews were conducted from October to November 2020, and approval for this study was obtained from the New York University Grossman School of Medicine Institutional Review Board. Table 2 shows the number of provider interviews completed by CHC site and clinical service.
Number of Provider Interviews Conducted by Site and Clinical Service in Study of Community Health Center Providers' Experience of a Transition to Telemedicine During COVID-19—October to November 2020
The research team employed rapid qualitative methods in which we took a protocol-driven, deductive approach to analyze these data.24 We developed an interview summary template as a systematic way of extracting and condensing the data. Each interview question was assigned a predetermined domain name. The research team used the templates to outline the main points related to each domain and capture corresponding illustrative quotes. The interview team tested the summary template using 2 interview transcripts. Three people reviewed each transcript and completed the summary template. A side-by-side comparison was made of information extracted from the transcripts, including the amount of data extracted and attribution to specific domains. Minor modifications were made to the summary template to ensure ease of use and enhance comparability among data extractors. Once the template was finalized, the research team split up the remaining transcripts and completed the summary templates. After this process, the research team created a matrix of findings to synthesize the data across the 25 individual summaries. The summary template is available as supplemental material.
Findings
Telemedicine Modalities Used over Time
Before COVID-19, telemedicine visits accounted for a small percentage of total visits to CHCANYS health centers. On February 22, video and telephone visits accounted for 3.4% and 0% of visits, respectively. In the first week following the March 22 NYS stay-at-home order and emergency changes to the NYS Medicaid program, these figures jumped to 14.9% and 22.3%, respectively. (Figure 1).
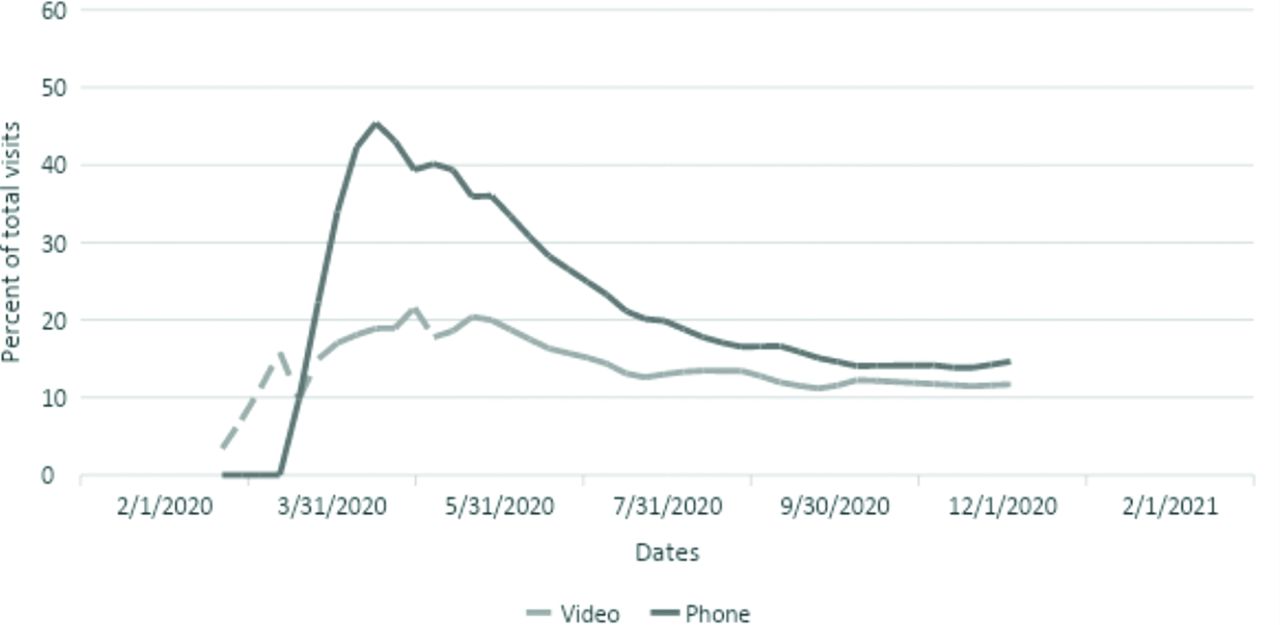
Percentage of telemedicine visits by modality (telephone vs video). Legend: Percentage of visits made by video or telephone to 36 community health centers that belong to the Community Health Care Association of New York State (CHCANYS) from February to October 2020. Total visits (denominator) include all outpatient visits, including in-person, telephone, and video visits. Before the onset of COVID-19, on February 22, video and telephone visits accounted for 3.4% and 0% of visits, respectively. In the first week following the March 22 NYS stay-at-home order and emergency changes to the NYS Medicaid program, these figures jumped to 14.9% and 22.3%, respectively.
Both video and telephone visits increased significantly at the height of the first wave of COVID-19 across NYS. At its peak, more than 60% of visits were conducted via telemedicine (April 11 to May 2), most of which was provided via telephone. At every point following the stay-at-home orders, telephone visits accounted for a larger proportion of telemedicine visits than video visits, but the difference narrowed considerably over time. Telemedicine visits tapered off toward the beginning of August, accounting for less than 30% of visits.
Provider Perspectives on Telemedicine Use during COVID-19
Interview responses were grouped into 5 categories: 1) benefits of telemedicine; 2) pitfalls of telemedicine; 3) comparison of modalities; 4) role of reimbursements; and 5) suggested improvements.
Benefits of Telemedicine
All 3 provider groups (primary care, pediatrics, behavioral health) perceived the care provided during telemedicine visits as being of similar quality to in-person visits and telemedicine as being successful in reducing patient no-shows. There was also agreement that telemedicine provided flexibility for patients and reduced barriers to care such as transportation, childcare, and work-related time constraints, resulting in an overall improvement in patient access. As explained by 1 pediatric provider:
“It's almost like all the barriers that are in place with this socially complex population were taken away because I can see you in your home, and we can spend as much time as you want to. You don't have to be rushing from work. You don't have to skip the appointment because you have to pick up your kids from school. We can just do this visit, and it's not rushed.”
Slight differences emerged among provider groups regarding the different aspects of health care delivery for which telemedicine was beneficial. Primary care providers noted the positive effects of telemedicine on chronic disease management, allowing providers to better monitor patients with comorbidities and improving the quality of care for such conditions using quick telephone check-ins. For behavioral health providers, the benefit of telemedicine included the ability to bring in off-site participants, such as social workers, to engage in group interactions which otherwise would not have been possible. Telemedicine was also seen as useful in reducing stigma surrounding accessing behavioral health services by alleviating concerns that patients would be observed entering the clinic.
Each provider group identified patient populations and treatments for which telemedicine was particularly useful. These included older adult populations, patients with comorbidities, frail or infirm patients, homebound patients with physical disabilities, patients with anxiety, pre-exposure prophylaxis (PrEP) patients that require relatively frequent visits, and patients undergoing opioid addiction treatment. Patients reliant on public transportation, patients with children, and patients with busy work schedules or jobs with less autonomy to leave during the workday were also cited as priority population groups for telemedicine.
Pitfalls of Telemedicine
There was consensus among provider groups that despite the benefits of telemedicine, there were limitations surrounding the type of services that can be offered. Primary care and pediatric providers generally did not find telemedicine useful for visits requiring physical examinations, such as rashes or earaches. Furthermore, for primary care providers, a lack of equipment in patients' homes, such as scales or blood pressure cuffs, lowered providers' ability to assess patient health accurately. Without such home-based monitoring devices to support remote care, primary care providers noted limitations in managing chronic illness remotely.
Pediatric providers noted that certain types of care, such as play therapy, ongoing well-child annual visits, and vaccinations, were not possible over telemedicine. These limitations were amplified for certain patient populations. For example, behavioral health providers and pediatric providers treating adolescents discussed confidentiality and privacy issues for patients at home who may be surrounded by family members. In addition, for some behavioral health patients who struggle with social isolation and anxiety, telemedicine is not useful as it represents a further loss in human contact. Further, for new patients requiring an initial intake visit, it was more difficult for providers to establish rapport. This finding was particularly relevant for behavioral health providers seeking to develop a therapeutic connection with new patients via telemedicine.
In addition, providers noted added challenges surrounding the integration of telemedicine visits within the existing clinical workflow. For example, providers found it difficult to connect with interpreters, accomplish team-based care with warm handoffs, or refer patients to nonmedical services external to the clinic while using telemedicine. This issue is particularly salient for the high-risk population that the CHC sites serve since patients commonly have unmet social determinants of health needs that require referral to additional services. One pediatric behavioral health provider noted:
“A big concern for me is that a lot of time, again, the parents will bring in the kids here. We used to have a caseworker, a case manager here on the floor. Then when they would see me and I find out that there were certain social challenges, I will connect them right away. Right now, I keep asking those questions about their social situation, financial situation, but now I don't have that [with telemedicine].”
Heavy reliance on telemedicine also raised concerns around increased caseloads and physician burnout, particularly among behavioral health providers who noted increased demands for mental health services. Some providers perceived managing and monitoring a high caseload in high stress or crises to be easier with telemedicine due to the quick, easy access provided by telephone visits. However, some behavioral health providers reported feeling exhausted from the decrease in no-show appointments that previously allowed for catch-up on administrative tasks. One behavioral health provider explained:
“The psych providers have all kind of been talking about feeling burned out and feeling exhausted. So, some of the things we've done with that is try to adjust now that we're having a lower no-show rate, making sure that we're not scheduling as many patients maybe as we were in the past. So, we're trying to adapt in that way. Trying to make sure that we have regular meetings to check in and adjusting people's schedules as needed.”
Comparison of Modalities: Telephone versus Video-Enabled Telemedicine
Videoconference technologies were identified as being particularly useful by all provider types in allowing providers to monitor a patient's home environment and engage with family members and caregivers who may not have otherwise attended an in-person visit. Behavioral health providers specifically reported that certain therapeutic methods were possible through video-enabled telemedicine but not telephone visits, such as Eye Movement Desensitization and Reprocessing (EMDR).
Video also made it possible for providers to view patients' actual medications and ascertain whether they were being taken appropriately. Visual cues, such as for hygiene and self-care, also helped with clinical assessment. One primary care provider noted:
“I think there is something just to be gained when I am able to see someone. Body language and facial expressions, those subtle parts of nonverbal communication, are available, whereas, over the telephone, they aren't. We rely on them quite a bit. Overall, I can kind of see just how someone is doing. Are they smiling? Are they happy? People can show me things on their skin or anything that might be readily visible. You gain a lot of information by seeing the environment that someone is in as well. For many of us, sometimes it was the first peek into their home environment or their apartments, which can give us a lot of important visual cues as well.”
However, some primary care providers explained that telephone calls with physicians may provide patients with a sense of intimacy that video consultations lack. Telephone calls were also perceived as allowing patients more privacy in the home than video consultations and providing greater flexibility around where and when patients can have a visit. Although behavioral health providers registered conversation gaps with telephone consultations due to an inability to read body language or facial expressions, they also felt that psychotherapy quality was at times better over the telephone, as not being seen allowed patients to speak more openly, with more transparency and without the added pressure on their appearance or background. As 1 behavioral health provider noted:
“Many times, patients when they go face to face, they want to show the best of them, and they put up a show, the defense of ‘I'm fine’ or minimizing what happened. But when they are home, and there's nobody staring at them or judging them, they can actually feel themselves, and that's why my interventions, I feel, have been very helpful in moving people through the treatment process.”
Providers also noted technological issues with videoconferencing modalities, as well as a digital divide among patient populations. Specifically, poor Wi-Fi connectivity, a lack of devices with video capabilities, and limited data plans were cited as constraints to successful video consultations, with all 3 provider groups specifying that these issues were exacerbated in low income, rural, and vulnerable populations who may necessitate socially distanced visits the most. In such cases, there was agreement among provider groups that telephone serves as a necessary option to facilitate patient access to care. However, all 3 provider groups identified videoconferencing, when a viable option, as preferred to telephone.
Providers also noted that preference for modality also differed by patient. While the majority of providers reported that patients generally preferred video-enabled telemedicine, when possible, some providers expressed that certain groups of patients, including gender-nonconforming individuals and autistic individuals, preferred telephone visits over video visits because seeing themselves on video caused emotional discomfort. For patients lacking the technology or access for video consultations or patients with lower levels of technical literacy, providers noted that audio-only visits represented the only viable option for a remote clinical consultation. In such cases, audio-only visits were perceived as a necessary alternative to audiovisual or in-person consultations.
Role of Reimbursements
All provider groups emphasized the need for telemedicine visits, both audio-only and videoconference consultations, to remain reimbursable for providers to be able to provide ongoing support and care to patients without compromising the financial stability of health care organizations. As explained by 1 pediatric provider:
“From my perspective, it would be like cutting patients off at the knees if they ever stopped reimbursing for telephone visits because—though it's not ideal—there is still so much value in talking to the patient, accessing the patient, getting the patient the refills that they need so they don't end up having a hypertensive emergency or God forbid an asthma attack in a child.”
The provider groups mentioned 3 types of reimbursement: continued reimbursement parity for video and in-person visits, reimbursement parity for audio-only and audiovisual consultations, and reimbursement for home-health equipment, which was perceived as salient for patients with chronic conditions that required continuous monitoring.
Most providers were familiar with pandemic-related changes to reimbursement policies and noted that access to care would be diminished in the future should reimbursement policies for video visits revert to pre-pandemic rates. In particular, providers raised concerns over the sunsetting of reimbursement for audio-only consultations, citing potential issues related to equitable access for key populations, including older adult and low-income patient populations. As 1 pediatrics provider noted:
“I think in terms of equity, it totally is against elderly and I also think that, for those patients with the economic issues, the people who didn't access care because of economics now have found a way to access care that fit into their ability to deal with the economics of taking care of their health before it was too late.”
There was also strong agreement that reimbursements played a role in determining the type of visits a clinic can offer. As stated by 1 primary care provider:
“If you differentially reimburse, then you're going to have the differential ability to provide services. If you place a value that's higher on one kind of a visit than another, and somebody can't access that level of visit, you're automatically saying, ‘you don't get better quality care, you're going to get this lesser-quality of care.”
Suggested Improvements
There was consensus among provider groups regarding how telemedicine could be improved going forward in 3 key areas. First, providers noted desired changes to telemedicine platforms. For example, providers said platforms could be made more user-friendly for patients with low levels of computer literacy, built to support team-based care, have links to interpreter lines, and integrate an ability to stratify patients by risk level to determine the visit type needed. Providers also noted that having a platform that could integrate with electronic medical record systems (EMRs) would allow providers to conduct telemedicine visits more smoothly.
Second, providers cited a need for financial assistance for organizations to obtain the technologies necessary to implement telemedicine successfully. This need included funds for updated telemedicine platforms for providers, as well as for home-monitoring equipment, such as scales and blood pressure cuffs for patients. Additional financial assistance to provide training for staff on troubleshooting with patients and develop evidence-based skillsets the provision of telephonic and video care was also mentioned.
Third, providers noted that city- and community-level initiatives, such as Wi-Fi enhancers and universal broadband access, were necessary to improve the quality of telemedicine visits, and in particular, video consultations. As noted by 1 behavioral health provider:
“People don't have the access to the high spend platforms equipment. They don't… It's no different from if you live in a poor neighborhood; the school is not as great as if you're on the Upper West Side. If you live in a poor neighborhood, the connectivity, the fresh food, all of the issues that come with being poor, and the inequities are the same reflected back with telemedicine.”
Discussion
In this study of safety-net providers across New York State, we found that the use of telemedicine increased significantly throughout the COVID-19 pandemic. In under 2 weeks, most visits transitioned to telemedicine, with telephonic care being the primary mode of care delivery. Our findings are consistent with early experiences from other providers reported in recent literature. For example, most in-person visits were replaced by telephone visits at a large Veteran Affairs primary care health system in the first few weeks of COVID-19 related lockdowns.25 Similarly, telephone care was the “telemedicine mainstay” at 4 primary care practices across the United States as of April 2020.26 Our study examined visit patterns over 9 months into the pandemic and found that telemedicine visits increased significantly, mainly driven by an initial spike in telephone visits. Though the proportion of telemedicine visits decreased over time, they remained well above pre-pandemic levels. At every point in time, a greater proportion of visits were conducted via telephone compared with video, suggesting that audio-only visits may play a crucial role in maintaining access to care in the longer term.
Qualitative results corroborate these trends. All 3 provider groups believed both video and telephone visits were and will continue to be critical for enabling access to care. Consistent with other studies, providers expressed a strong preference for video visits, particularly for situations when visual assessments were needed.14 However, feasibility remained a clear concern. Providers noted that barriers to video-enabled telemedicine, such as poor Wi-Fi connectivity, lack of access to devices with video capabilities, and limited data plans, were exacerbated in the low-income communities they served.
These findings add to the growing literature on the impact of the digital divide in the age of COVID-19.27⇓–29 The digital divide refers to the gap between people who have full access to digital technologies and those who do not. Prior studies suggest that sociodemographic characteristics of patients are strongly associated with the willingness and ability to use video-enabled telemedicine both before and early in the COVID-19-related lockdown.8⇓⇓–11 This divide is amplified among safety-net populations such as those served by community health centers. Children in low-income households and children who are Black or Hispanic are significantly less likely to have access to a computer than wealthier or white peers.30 Older, low-income, and less educated patients were also less likely to use video-enabled telehealth.31–32 Consistent with existing literature, providers in our study observed low levels of technology literacy and less uptake in video-enabled appointments among older patients, suggesting that equity remains a salient concern when considering telehealth modalities.
However, while all 3 provider groups noted challenges related to the digital divide, telemedicine seemed to pose distinct challenges for the 3 populations served. Pediatric providers noted that parents would sometimes conduct a visit without their child, so ensuring children were located next to parents during visits were uniquely challenging. Sitting still visits without distractions also proved difficult for younger patients. Meanwhile, primary care providers noted the lack of access to physical equipment, such as blood pressure cuffs, scales, and pulse oximeters, as a challenge in using telemedicine. Behavioral health patients highlighted issues related to privacy and confidentiality when using telemedicine more so than the other patient groups, a finding confirmed in the existing literature.33–34
It is noteworthy that providers from all 3 categories found several benefits specific to telephonic care. Many of these benefits, such as the acceptability of telephone visits among patients or the increased access to care afforded by telephone visits, were identified in previous studies.35⇓⇓⇓⇓⇓⇓–42 Our respondents also noted unexpected benefits, such as increased privacy and an enhanced sense of intimacy with telephone visits, as well as the ability to better manage care for patients in high-stress or crises due to the quick, easy access provided by telephone visits. Therefore, while all 3 types of providers generally preferred video, they relied heavily on the telephone as a lifeline. All provider groups emphasized they wanted both audio-only and videoconference consultations to remain reimbursable.
There are several limitations to our study. First, this study of primary care, behavioral health, and pediatrics providers are limited to the experiences of providers working within CHCs in New York. CHCs are federally supported health centers that offer an affordable care option for primary care. To be designated as a CHC and receive federal funding, providers must offer care to patients regardless of the ability to pay and provide comprehensive health services, including behavioral health services.21 As a result, the experiences of providers in our study may not reflect those of other primary care providers in broader settings, such as teaching institutions, hospitals, or private community practices.
Furthermore, though some federal regulations determine the use of telemedicine, many telemedicine policies, including reimbursements, differ from state to state. The experiences of providers' practices in New York State may not reflect those of providers in other states. Second, this study presents the opinion of providers and does not elaborate on the experiences of patients. Future studies should examine patient experiences of telemedicine and explore areas of divergence or congruence across patient and provider responses. Third, participation in this study was voluntary, and participation may have been biased toward those who felt most strongly about the topic of telemedicine. Finally, our study combines the experiences of different types of services and providers into 1 group. The appropriateness of a telehealth visit may depend on the type of service provided. Though we touch on some differences that emerged across the 3 provider groups, our study fell short of thoroughly comparing the experiences of the different providers.
The COVID-19 pandemic and the need to limit unnecessary in-person interactions prompted the federal government, some states, and some health insurance carriers to relax telemedicine restrictions, including allowing patients to access services from home and allowing telephone visits to qualify as telemedicine.2,3 Specifically in New York, the state's Medicaid program expanded coverage for telemedicine services, including “assessment, diagnosis, consultation, treatment, education, care management and/or self-management of a Medicaid member.” Furthermore, for purposes of the State of Emergency, the definition of telemedicine was “expanded to include telephone conversations.”43 The rapid growth in both telephone and video visits following these policy changes suggests the changes successfully promoted access to care during the height of the COVID-19 pandemic.
Telemedicine has been described as a “silver lining” in the pandemic, allowing patients to access care easily and flexibly.44⇓⇓–47 Though several studies have been published on this topic following the pandemic, our study is the first to examine visits patterns over a longer period (9 months) and report provider perspectives about their experience delivering care using these different modalities. We found that telemedicine use declined over time as clinics began to offer more in-person care. Yet, both telephone and video visits remained above pre-pandemic levels even after COVID-related restrictions eased. These findings suggest that while on-site clinical visits are crucial for patient care, both video and telephone visits will continue to shape how health care is delivered in a post-pandemic world.
At least 1 prior study comparing traditional on-site visits to telemedicine visits found that patient satisfaction hinged on the perception of how the physician communicated. For example, the sound of the clinician's voice and the types of questions that were asked during the visit were rated as more important than the doctor's physical presence.48 These results suggest that regardless of modality, what may matter more is that the patient feels listened to. In our study, providers perceived care delivered through telemedicine to be of similar quality to in-person visits. When it came to communicating with patients, providers noted that telephone consultations might open conversation gaps due to an inability to read body language or facial expressions. Yet, for some visits, such as psychotherapy, not being seen may allow patients to speak more openly and with greater transparency. Future studies should explore how to support communication between patients and providers using different modalities. Other studies should also assess patient and provider preferences for the optimal type of modality and match these preferences to the most appropriate form of care delivery.
Acknowledgments
We thank Marie Mongeon, Cole Unger, Diane Ferran, and Jeff Barnes of the Community Health Care Association of New York State (CHCANYS) for the data used in this study.
Notes
This article was externally peer reviewed.
Funding: The preparation of this manuscript was supported by funding from RCHN Community Health Foundation.
Conflict of interests: None.
To see this article online, please go to: http://jabfm.org/content/34/6/1103.full.
- Received for publication April 30, 2021.
- Revision received July 16, 2021.
- Accepted for publication July 21, 2021.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of billing policy changes on telehealth use in Ontario: a population-based repeated cross-sectional study
- Reasons for encounter in video contacts at a Danish out-of-hours primary care service: a questionnaire study
- Telemedicine Adoption During COVID-19 Pandemic: Perspectives from Primary Care Clinicians in Safety-Net Settings
- The Most Frequently Read Articles of 2021
- Research on the Issues Family Physicians Face Today: Controlled Substances, COVID-19, Hypertension, and "Slow Medicine," Among Many More Topics