
Article Figures & Data
Figures
- Figure 1.
Chart Flow Diagram. Abbreviation: PBRN, practice-based research network.
- Figure 2.
The Thematic Structure of PBRN Establishment. Abbreviation: PBRN, practice-based research network.


Tables
Inclusion Criteria 1. Peer-reviewed journal articles published between 1/1/1965 and 12/31/2020 in English language that refer to one or more primary care PBRNs and include information about their establishment. 2. Articles that refer to research projects conducted by PBRNs that also provide information about their establishment. 3. Reports, editorials, letters, commentaries, conference papers, and web pages that may provide complementary information on an already identified PBRN. 4. Information on PBRN establishment was included after defining primary care-linked PBRNs based on the scope of primary care in each particular region or country. Exclusion Criteria 1. Articles that focus on specific research studies, data collection, or database/technology development in PBRN settings, without providing information about the PBRN's establishment. 2. Articles in which the identity of the PBRN can't be determined (e.g., due to blinding). PBRN, practice-based research network.
- Table 2.
Included Practice-Based Research Networks, Peer-Reviewed Articles, and Review Sources
PBRN Country Year of Foundation Peer-Reviewed Articles and Review Resources 1. Nijmegen Family Practice Academic Network The Netherlands 1967 Van den Bosch 1993223 Van Weel et al 20009 Gunn 200210 Schers et al 2008136 Van Weel 20087 2. Weekly Returns Service (WRS) United Kingdom 1967 Fleming and Crombie 1985158 Fleming et al 19916 Fleming 199949 3. Dutch Sentinel General Practice Network (SGPN) The Netherlands 1970 Schweikardt et al 201647 4. Dartmouth-Northern New England Primary Care Cooperative Research Network/COOP Project USA 1977 Nelson et al 1981130 Nelson et al 198154 Nelson 1983224 Mold and Peterson 2005112 5. Ambulatory Sentinel Practice Network (ASPN) USA-Canada 1978 Green et al 198435 Iverson et al 198836 Rosser and Green 198937 Green et al 1993180 Main et al 1993225 Green et al 1994104 Nutting et al 1999181 Lindbloom et al 2004164 Pearls of Research125(p20,22,24) 6. Belgian Network of Sentinel General Practices Belgium 1978 Lobet et al 1987161 Boffin et al 2010155 Boffin et al 2013226 7. Minnesota Academy of Family Physicians Research Network (MAFPRN) USA 1978 Solberg et al 1983171 Solberg et al 198656 8. Centro Studi e Ricerca in Medicina Generale (CSeRMeG PBRN) Italy 1983 Visentin 200576 9. Pediatric Practice Research Group (PPRG) USA 1984 Christoffel et al 1988170 LeBailly et al 2003167 Ariza et al 2004227 LaBresh et al 2014228 10. International Primary Care Network (IPCN) National range PBRNs of primary care physicians from Belgium, Canada, England, the Netherlands, Switzerland, and USA 1985 Culpepper and Froom 198841 Froom and Culpepper 1991229 11. San Francisco Bay Area Collaborative Research Network (SFBayCRN, previously UCSF PBRN) USA 1985 Osborn and Petitti 1988138 Croughan-Minihane et al 1999127 Pearls of Research 1998125(p104) 12. Transition project (Thanshis) The Netherlands 1985 Okkes et al 2002230 13. General Practice Information Network New Zealand 1986 Kljakovic et al 1992231 Leitch 2016232 14. Pediatric Research in Office Settings (PROS) USA 1986 Wasserman et al 1992160 Wasserman et al 1998131 Slora et al 2006178 Slora and Wasserman 201096 Wasserman et al 201155 15. Wisconsin Research Network (WReN) USA 1987 Pearls of Research 1998125(p65–71) Beasley et al 1991124 Van Weel et al 20009 16. University of Missouri PBRN USA 1987 Williamson et al 1988131 17. Harrisburg Area Research Network (HARNET) USA 1988 Slawson et al 1993189 Shaughnessy et al 1999233 18. (CumbReN) United Kingdom 1988 Robertson et al 200568 19. Upper Peninsula Research Network (UPRNet) USA 1988 Pearls of Research 1998125(p72–5) 20. Registration Network Family Practices (RNH) The Netherlands 1988 Metsemakers et al 1992109 Knottnerus et al 1992234 Van den Akker et al 1998182 de Lusignan and van Weel 2006235 21. Royal New Zealand College of General Practitioners (RNZCGP CRN) New Zealand 1989 Tilyard et al 1995236 Dovey and Tilyard 199684 Rodnick 1999237 Hall and Martin 2003238 Leitch 2016232 22. Clinical Directors Network (CDN) USA 1989 Sardell 1996111 23. General Practice Data Retrieval Project (GPDRP) United Kingdom 1989 Boydell et al 1995106 24. Utrecht University General Practices Network The Netherlands 1989 Hak et al 1998239 Hak et al 1998240 Venmans et al 2009186 25. African Sentinel Practitioner Research Network (SASPREN) South Africa 1990 Volmink and Furman 199148 Volmink 1996146 Volmink et al 1996174 De Villiers 1998179 26. University of Adelaide PBRN Australia 1990 Marley 1992145 27. Rotterdam General Practitioners Project (ROHAPRO) The Netherlands 1990 Middelkoop et al 1994241 Middelkoop et al 199557 28. Australian Sentinel Practice Research Network (ASPREN) Australia 1991 Gunn 200210 Clothier et al 200546 29. Northern Primary Care Research Network (NoRen) United Kingdom 1991 Carter 199852(p77,79–83,86) 30. South Texas Ambulatory Research Network (STARNet) USA 1992 Noël et al 2011242 Hayes and Burke 2012243 STARNet244 31. Medical Research Council General Practice Research Framework (MRC GPRF GPRF) United Kingdom 1993 Carter 199852(p122–6) Comino 200270 32. Oklahoma Physicians Resource/Research Network (OKPRN) USA 1994 Mold and Barton 1996113 Mold and Peterson 2005112 Nagykaldi et al 2005168 Mold and Gregory 2003184 Pearls of Research 1998125(p85) Nagykaldi et al 2006245 33. Wessex Research Network (WReN) United Kingdom 1994 Smith and Dunleavey 199678 Van Weel et al 20009 Gunn 200210 34. Intego Belgium 1994 Truyers et al 2014147 Van Casteren et al 2015246 35. Practice Partner Research Network (PPRNet) USA 1995 Ornstein and Jenkins 199791 Mold and Peterson 2005112 Nemeth et al 2007247 Wessell et al 2008248 36. Virginia Ambulatory Care Outcomes Research Network (ACORN) USA 1996 Etz et al 2015249 ACORN250 37. STaRNeT United Kingdom 1996 Carter 199852(p84–5, 89–101) Thiru et al 2003251 Comino 200270(p12,23,29) 38. Residency Research Network of Texas (RRNeT) USA 1997 Albright et al 2001252 Hill et al 2012253 Hayes and Burke 2012243 Burge and Hill 2014121 RRNeT254 39. High Plains Research Network (HPRN) USA 1997 Mold and Peterson 2005112 Westfall et al 2006255 40. Trent Focus Collaborative Research Network United Kingdom 1995 Frew et al 2001256 Cooke et al 200271 Comino 200270 Hammersley et al 2002257 Trent Focus, Annual Report 1996-9769 Trent Focus, Annual Report 1998-99141 Trent Focus, Annual Report 1999 to 2000141 Trent Focus, Annual Report 2000 to 2001123 Trent Focus, Annual Report 2001 to 2002258 41. East London and Essex Network of Researchers (ELENoR) United Kingdom 1997 Davies et al 200258 Davies et al 200259 Graffy et al 200272 Graffy 2003259 Abbott and Gunnell 200551 42. North Staffordshire General Practice Research Network United Kingdom 1997 Porcheret et al 200474 Hayward et al 2013260 43. West London Primary Care Research Network Community Interest Company (WeLReN) United Kingdom 1997 Thomas and While 200186 Comino 200270 44. TayRen United Kingdom 1998 Pitkethly and Sullivan 200373 45. Scottish Primary Care Research Network SPCRN (previously SPPIRe) United Kingdom 1998 Zwar et al 2006261 Sullivan et al 200775 Sullivan et al 201460 46. American Academy of Family Physicians National Research Network (AAFP NRN) USA 1999 Lindbloom et al 2004164 Graham et al 2007120 AAFP National Research Network162 Galliher et al 2009177 47. Belgian Primary Care Data Network Belgium 1999 DeClerq et al 2002144 48. Advanced Practice Registered Nurse Network (APRNet) USA 1999 Deshefy-Longhi et al 2002169 McCloskey et al 200397 Olsen et al 2005262 Deshefy-Longhi et al 2008263 49. ASPIRE (A Sign Health Polyclinics Initiative for Research Excellence) (Singapore) Singapore 2000 Chuan and Gan 2001264 50. Dumfries and Galloway Primary Care Research Network United Kingdom 2000 Hannay 200661 51. General Practice Research Network (GPRN) Australia 2000 Sayer et al 2003129 Trinh et al 2017265 52. Research Involving Outpatient Settings Network (RIOS Net) USA 2000 Sinclair-Lian et al 2008266 Williams et al 2009267 53. Kentucky Ambulatory Network (KAN) USA 2000 Pearce et al 200498 Love et al 2006134 54. Southern Primary-Care Urban Research Network (SPUR-Net) USA 2000 Kuo et al 200899 55. University Family Practice Network (UFPN) Australia 2000 Laurence et al 2001136 Gunn 200210 56. North Carolina Family Medicine Research Network (NC-FM-RN) (Now NCnet) USA 2001 Sloane et al 2005268 Sloane et al 2006140 Gourlay et al 2010183 57. Primary Healthcare Research Network-General Practice (PHReNet) Australia 2001 Comino 200270 Comino et al 200262 Mehmet et al 2004269 Magin et al 2011143 58. Continuity Research Network (CORNET) USA 2002 Serwint 2001114 Serwint et al 2006175 Wasserman et al 201155 59. Oregon Rural Practice-Based Research Network (ORPRN) USA 2002 Nagykaldi et al 2006245 Fagnan et al 2007156 ORPRN115 60. Midwest Nursing Centers Consortium Research Network (MNCCRN) USA 2002 Anderko et al 2005270 Anderko et al 2005139 Anderko et al 200653 61. South Australian Primary Health Care Research Network (SARNet) Australia 2002 Waters et al 200463 Ried et al 2006100 Aims and objectives for the SARNet Research Network 2006271 Ried et al 200765 Farmer et al 2005272 62. Mecklenburg Area Partnership for Primary Care Research (MAPPR) USA 2003 Dulin 2005107 Dulin et al 2010273 Dulin et al 2011157 Dulin et al 2012274 MAPPR275 63. Electronic Primary Care Research Network (ePCRN) USA and United Kingdom 2004 Peterson et al 200623 Fontaine et al 200738 Delaney et al 201239 Peterson et al 201240 64. Massachusetts School Nurse Research Network (MASNRN) USA 2004 Vessey 2007166 Pulcini et al 2008276 65. CONTinuous Morbidity Registration Epidemiologic NeTwork (CONTENT) Germany 2005 Laux et al 2005150 Chmiel et al 2011187 66. ResoPrim Project Belgium 2005 De Clercq et al 2009277 67. UK Clinical Research Network (UKCRN) and National Institute for Health Research (NIHR) CRN United Kingdom 2006 Department of Health 2006278 Department of Health 200627 Sullivan et al 200775 Cooke et al 200850 Pickstone et al 200885 National Institute for Health Research 2012279 National Institute for Health Research 2014135 National Institute for Health Research 2014280 Local Clinical Research Networks 2016281 68. GRACE-01 International 2006 Butler et al 200942 Nuttal et al 201143 69. DARTNet USA 2007 Pace et al 200921 Maro et al 2009282 Pace et al 2009188 Libby et al 2010116 Pace et al 2014153 70. Greater Rochester-PBRN (GR-PBRN) USA 2007 Gibson et al 2010102 71. OCHIN Practice-Based Research Network (OCHIN PBRN) USA 2007 DeVoe et al 201190 DeVoe et al 201292 DeVoe and Sears 2013110 Arkind et al 2015283 72. Victorian Primary Care Practice-Based Research and Education Network (VicReN) Australia 2007 Soós et al 201066 Australian Primary Care Research Network APCReN221 73. Canadian Primary Care Sentinel Surveillance Network (CPCSSN) Canada 2008 Birtwhistle et al 2009126 Birtwhistle 2011159 Peckham and Hutchison 2012284 Coleman et al 2015285 74. European Academy of Pediatrics Research in Ambulatory Settings network (EAPRASnet) International 2008 Del Torso et al 201044 75. TARGet Kids Toronto Area Research Group Canada 2008 Morinis et al 2012149 Abdullah et al 2015286 Carsley et al 2015148 76. FIRE Project (Family Medicine ICPC-Research Using Electronic Medical Records) Switzerland 2009 Chmiel et al 2011187 Rizza et al 2012287 Zellweger et al 2014288 77. Centricity Health Care User Research Network (CHURN) USA N/A (2009?) Lieberman 200682 Gill et al 2010289 Gill et al 2012185 78. West of Ireland Research and Education Network (WestREN) Ireland 2009 Kavanagh et al 2010122 79. Electronic Practice Based Research Network (e-PBRN) Australia 2010 Liaw et al 2011103 Taggart et al 2012152 e-PBRN290 80. Scalable Architecture for Federated Translational Inquiries Network (SAFTINet) USA 2010 Schilling et al 2013165 Kwan et al 2013291 Sills 201588 Kwan et al 201693 81. Community Health Applied Research Network (CHARN) USA 2010 Likumahuwa et al 2013108 82. VA WH-PBRN (USA) USA 2010 Frayne et al 201382 Pomernacki et al 2019292 83. WWAMI Region Practice and Research Network (WPRN) USA 2011 Baldwin et al 201218 Stephens et al 201295 Cole et al 2014115 Cole et al 2016293 84. Illawarra and Southern Practice Research Network (ISPRN) Australia 2011 Dijkmans-Hadley et al 201567 85. PBRN-OSH Sweden 2011 Jensen et al 202083 86. Irish Primary Care Research Network (IPCRN) Ireland 2012 Galvin et al 2015294 Dillon et al 2015154 IPCRN127 87. Home Visiting Applied Research Collaborative/Home Visiting Research Network (HARC/HVRN) USA 2012 Duggan et al 201379 88. Swiss Primary Care Active Monitoring Network (SPAM) Switzerland 2012 Selby et al 2015176 89. Developmental Disabilities Practice-Based Research Network (DD-PBRN) USA 2013 Tyler and Werner 201481 90. Australian Chiropractic Research Network (ACORN) Australia 2015 Adams et al 2015295 Adams et al 201680 Adams et al 2017296 ACORN250 91. Tutka Primary Care Research Network (TUTKA) Finland 2015 Koskela 2017118 92. University of Limerick Education and Research Network for General Practice (ULEARN-GP) Ireland 2018 O'Regan et al 202089 93. Pacific People's Health Advisory Group (PPHAG) PBRN Samoa, Tonga, Cook Islands, Niue, and New Zealand 2018 Lamont et al 202045 PBRN, practice-based research network.
- Table 3.
Overarching Thematic Framework for the Establishment of Practice-Based Research Networks Focusing on the Theme of the Internal Environment Described in This Article
Theme Subtheme Key Elements (i) Internal environment of PBRN (ii) Foundation (i) Setting up mission, purposes, goals, objectives, and aims (ii) Practitioner participation and motivation (i) Recruitment (ii) Membership (iii) Levels of member engagement (iv) Intrinsic motivators to participate and benefits for practitioners (v) Extrinsic motivators to participate and benefits for practitioners (iii) Academic participation and attitudes (i) Type of affiliation and advantages–disadvantages of affiliation (ii) The role of academics and academic departments in developing, hosting, and sustaining the network (iii) Academic contribution to governance and leadership (iv) Contribution of academic research expertise (v) Academic support for research culture development and practitioner empowerment (vi) Academic initiative to link medical students and residents to PBRN activity (vii) Benefits for academia from PBRN collaboration (iv) Network infrastructure and operations (i) Initial partnerships to establish PBRNs and centers of operations (ii) Infrastructural funding (iii) Key activities at establishment (iv) Relationship building between academics and practitioners in the field (v) Governance (vi) Organizational leadership (vii) Methodology of prioritizing the research agenda (viii) Topics of PBRN research (ix) Data gathered from networks and data management (x) QI activities (xi) Learning environment (xii) Communication (ii) Stakeholders at the intersection between the internal and external environment (i) Patients and community stakeholders (i) Patient-centeredness and community engagement in PBRNs (ii) Relationship building with patient or community groups as an essential part of research (iii) QI activities guided by patient feedback (iv) Involving patients or community members in PBRN governance (v) Integrating CBPR methodology into PBRN research (vi) Community engaged research methodology in PBRN research (vii) Motivation of community members for research participation (viii) Community engagement in health policy making through PBRN activity (ii) Other health care stakeholders (i) Identification, engagement, and contribution of health care stakeholders (ii) Relationship building with health care stakeholders (iii) Other aspects of working with health care stakeholders (iii) External environment (i) National health system (i) The impact of primary health care structure on PBRN development (ii) Institutional/governmental support, national/state policy and regulatory environment (i) Decision-makers (ii) National policy (iii) Regulatory environment (iv) Interaction with policy-makers (v) Community impact on public health policy-makers through PBRN (iii) Professional organizations (i) National professional organization contribution and support (ii) International professional organization contribution (iii) External funders (i) External funder contributions (iv) Leveraging previous research and PBRN experience and interacting with other networks (i) International experience (ii) National experience (iii) Leveraging previous research expertise (iv) Leveraging PBRN practice models (v) Leveraging experience from peer networks (vi) Interacting with other networks (vii) Developing networks of PBRNs (v) HIT and HIT vendors (i) HIT applications sustain the infrastructure (ii) HIT applications facilitating or supporting the PBRN operation (iii) HIT vendors contribute to sustainability (iv) HIT vendor in the partnership of the network (v) Challenges from the variety of EHR systems EHR, electronic health record; HIT, health information technology; PBRN, practice-based research network; QI, quality improvement.
Facilitators Practitioner Participation Recruitment Identification of key issues of successful recruitment (using tools such as surveys, panels, forums, professional events, site visits, or face-to-face meetings)
Development and implementation of a recruitment strategy
Leveraging prior relationships with university faculty (personal/professional relationships, teaching practices, residency programs)
Leveraging previous research experience or PBRN experience
Recruiting members of existing PBRNs
Leveraging the potential of recently retired clinicians
Leveraging the experience of practitioner champions or research-motivated practitioners
Membership Identifying practitioner motivation through surveys
Personal motivators for PBRN membership
Practitioner scientific interest, self-motivation, and commitment
Flexibility in research participation (time, level of effort, methods) or protected time for research and research training
Expanding membership to all primary care professionals
Tailoring research to practitioner interests and encouraging practitioner empowerment
Engagement in development of research ideas and research prioritization and proposals
Research with direct impact on practice improvement
Higher degree of education that facilitates PBRN activity
Professional benefits and career development linked to participation
Educational opportunities
Participation in QI activities
Participation in research that is valued or what the practitioners perceive as rewarding
Financial and other incentives
Integrating new knowledge from research into teaching and linking research with practitioner growth
Relevant and easily applicable projects
Development of an integral relationship between practice and research
Structural benefits of data sharing
Direct incentives for investing time and effort into innovations
Research participation that is made motivating or even fun
On-site, hands-on research assistance
Other support or benefits/perks incorporated into membership
Membership in Large Networks/Networks of Networks Access to more robust resources and benefits derived from economies of scale
Reaching a large sample size
Enabling research on unexplored/understudied topics
Access to large, geographically dispersed, and demographically diverse populations allowing research that cannot be conducted otherwise
Access to technological, administrative, and scientific resources and expertise through a shared infrastructure
More rapid diffusion of learning and resources
Rich diversity of member experiences and backgrounds
Academic–Practitioner Partnership Availability of highly research-motivated academics who can help initiate the network
Knowledge and resources that reside within the academic discipline
Academic contribution to the development of a real-world research laboratory
Academic research expertise, scientific rigor, and fundraising potential
Academic contribution to research capacity building and practitioner empowerment including mentoring and supervising emerging researchers
Publications that enhance the primary care discipline
Better fundraising potential by leveraging the reputation of academics
Academic contributions to infrastructural funding and in-kind support (including academic and PBRN staff, logistics, administration, technology)
Academic engagement in the governance of PBRN
Academic support for career development (fellowships, grants, support for further education)
Academic initiatives to link medical students and residents to PBRN activity (“pipelining”)
Development of PBRNs that can supply data for external research
Practice-based research infrastructure may become cost-effective over time
Low-cost research assistance by involving medical learners
Cost-effective research by leveraging longitudinal data flowing from the membership
Networks that can be built more rapidly through academic connections
Infrastructure and Operations Infrastructure Funding Dedicated funding for infrastructure or long-term funding commitment (eg, from national agencies, national professional organizations or health organizations, international governing bodies)
Contributions from members
Dedicated funding for research capacity building
Development of business models for research and QI activities
Relationship Building between Academics and Practitioners in the Field Development of shared vision and common identity
Sustainable relationship building through on-site visits
Development of long-lasting collaborative relationships within and beyond the PBRN
Multidirectional communication, participatory membership model, appreciation of each other's preferences, values, and culture
Fostering research relationships by establishing partnerships along common interests, collegiality, and maintaining enthusiasm
Establishing collaborations across various disciplines and levels of seniority
Developing relationships of trust and respect between clinician members and academics and between members, governing boards, and practice managers/staff
Peer support from practitioners-champions (in research) to novice practitioner-researchers
Linking academicians with novice practitioner-researchers through mentoring
Satisfaction emerging from the achievements of small start-up projects
Developing strong bonds with academic mentors
Skill development based on mutual support and shared resources that add value to network products
Leveraging prior relationships with academia
Leveraging relationships established during previous QI activities or training
Partnering for shared learning and best practice implementation
Building on the ties between residents and community preceptors
Linking students to network activities
Linking practitioner research capacity building to asking timely research questions and the integration of practice-based research and QI outcomes into practice
Governance and Organizational Leadership Setting up a network upon a core of practice-based research motivated and experienced members
Governance that provides benefits for all members
Leaders who are champions and possess knowledge, energy, enthusiasm, and commitment to promoting PBRNs or practitioners with strong bonds to academic faculty
Reputation/track record of recognized academics involved in organizational leadership that help sustain the network
Strong leadership that applies close monitoring and frequent multidirectional communication
Data Collection and Management Data that are representative of the populations of interest
Data interoperability that facilitates collaborative medicine and the implementation of multiple functions such as clinical decision tools
Data that can support QI activities
"Big data” aggregation that allows population-level information on primary care delivery and building capacity for multiple concurrent (or longitudinal) studies
QI Activities A specific QI-informed mission that becomes an incentive for PBRN membership
Social and collaborative learning aspects of QI
Development of combined research and QI methodology promotes faster research translation
The impact of QI activities on daily practice through the implementation of best practices
Supporting QI activities using well-designed HIT tools
Learning Environment Training Training activities as a bridge to building relationships between practitioners and academics
Linking professional development with PBRN activity and providing dedicated funding to academic departments to participate in PBRN activity
Dedicated funding and supportive initiatives for training
Engagement in PBRN activity during and as a follow-up to residency
Fostering Learning Communities Building learning communities as one of the main objectives of a PBRN
Member motivation to share resources and to learn from and share practice-based knowledge and best practices
Member motivation to participate in the development and sharing of practice innovation and/or transformation
Member motivation to experience an exchange of knowledge and expertise between academia and practitioners
Communication Open and frequent communication using multiple means of synchronous and asynchronous methods
On-site visits of practitioner champions/exemplars/peers when they may exchange hands-on experience and advice and teach by example
Frequent on-site visits for research assistance to maintain interest and enthusiasm
Facilitating problem solving in everyday practice as part of a community
Events that promote interaction between members (academic–practitioner/practitioner–practitioner), intellectual exchange, and matching
Breaking down practitioner isolation
Sharing information about the progress of research (feedback, eg, via newsletters)
Frequent meetings of the oversight bodies
Empowering practitioners through ongoing communication
Barriers Clinical Practices Clinician and staff turnover
The burden (time, effort, and cost) of research
Larger practice size may result in increased research demands
Competing organizational priorities and workflow changes
Concerns for lost productivity due to research
Research ethical oversight-related challenges
Attracting and maintaining practice interest
Lack of support for research activities by practice leadership
Lack of cooperation from the clinic staff
Lack of research champions in the practice
Limited research support by experts
Low research capacity resulting in low engagement in research
Reorganization or transformation of practices
Limited practice space available for research activity
Negative research experiences in the past
Practitioners Not valuing practitioner contributions to research
Time constraints to participate in PBRN activities
Competing priorities between providing clinical services and research participation
Sustained participation in network activities (membership retention)
Moderate motivation for research
Barriers related to professional role (eg, nurses have no access to clinician records)
Lack of research skills and support to develop research skills
Lack of understanding the research methodology and low scientific rigor in research procedures
Restricted career opportunities for FPs/GPs and other primary care professionals
Lack of skilled mentorship
Insufficient access to a pool of scientific knowledge and resources necessary for research and evidence-based practice
Lack of academic connections or knowing who to turn to for information
Lack of remuneration for practitioner time spent with research
Poor self-image of FP/GP when envisioning their role and their position in the health care system or seeing themselves as researchers—lack of confidence in their ability as researchers
Academia A delayed development of family medicine/general practice as a distinct discipline
Lower capacity of primary care academics to attract external funding
Academia-driven PBRN research, which may not be important for the practitioners in the field
Academic-dominated research topics and top-down research processes
Financial Barriers Lack of continuity in administrative and/or overall infrastructural funding and dependence on project-based grant funding for infrastructure support
Discrepancies between network mission and funder interest
Lack of systematic support to cover infrastructure cost
Lack of financial compensation for PBRN member participation in research
Limited funding for practice-based research
A vicious circle where outside project-related funding is difficult to obtain until the network has a track record, but it is difficult to develop a track record without outside start-up funding
Relationship Building Criticizing instead of supporting low-performing practices in research projects
Low trust between academics and practitioners
A fear of displacement of practitioners by academics in research
PBRN Structure Creation of a sense of identity
Geographic dispersion of networks as a logistical challenge
Lower generalizability of research due to small numbers of participating practices
Challenges related to local and national realities, cultures and structures, and the additional length and cost of processes that define wide-scale activity in large networks
Complexity of maintaining a multilevel infrastructure in international PBRNs
Research Data Concerns Research data quality pertaining to recording (documentation), coding, and confidentiality
The importance of patient data privacy for the primary care practitioner
Setting agreements/rules about research data ownership, security, use, and sharing
Health data quality as it relates to the quality of documentation
Maintaining data quality in longitudinal studies
Data duplication as it relates to overlapping care episodes and care sites
Small network size may affect the validity of outcomes
Retrospective collection/analyses of recorded data
No uniform diagnostic and classification criteria or terminology for health conditions across the network
Variable primary care service coding practices
Representativeness of practices, practitioners, and patient population
Selection bias when establishing patient database
Voluntary membership may affect the quality of data
Research Study Design Interpretation bias may occur in research where different cultures and education are involved in international networks
Multipractice studies require more personnel time, travel, equipment, and supplies
Research may be more difficult in international networks that interact with populations associated with different language, means, and social context
Increased complexity of research coordination, lengthened timelines, and higher research costs in large networks
Identifying appropriate research study designs for specific studies that are also sensitive to the network environment
The model of health care delivery affects research planning and sufficient subject recruitment and retention
Restricted opportunities to frame and translate research results when practitioners have no strong participation in research
Communication Risk for communication gaps between practitioners and academics in large networks where communication happens through conveners
Communication clarity may be challenged by time constraints
Lack of good communication and understanding during research activities
Problems deriving from distance communication during research studies
FP, family physician; GP, general practitioner; HIT, health information technology; PBRN, practice-based research network; QI, quality improvement.
Recruitment Identify key issues of successful recruitment strategies (using tools such as surveys, panels, forums, professional events, on-site discussions)
Capitalize on opportunities for fostering participation within the network, eg, quality improvement activities, practice evaluations, practice transformation, data quality assurance
Leverage prior relationships with trusted and well-known academic faculty (personal/professional relationships, teaching practices, residency programs) and previous research experience or PBRN experience
Relationship Building Make research easy for the busy practitioner—eg, use research assistants or practice facilitators, pragmatic research designs, and incentivize practitioners when their effort is requested (“value proposition”)
Build reciprocal long-lasting collaborative relationships based on trust and let these to be the context of decision-making in the network
Develop member groups with matched interests
Value member participation in research in many ways and choose those that they most appreciate, eg, provide professional credits
Research Capacity Building Support the research capacity building and professional development of primary care practitioners with diverse opportunities that may respond to all educational preferences varying from online workshops and training to academic educational curricula
Foster learning communities across the members of the network
Communication Support open and frequent and multidirectional communication using multiple means of synchronous and asynchronous approaches
Offer community practitioners on-site (or virtual) visits with peers where exemplars may demonstrate the benefits and/or feasibility of research in their practice
Funding for Infrastructure Ensure sufficient funding for infrastructure through national agencies, local organizations, and the academic institution and develop a strategic plan for a business model with diversified portfolio for the future
PBRN, practice-based research network.
- Appendix Table 1.
Types of Organizations That Initiated and Supported PBRNs at Their Establishment and Relevant Quotations
Type of Organization Quotations A professional organization initiated the network “PROS is a program of the American Academy of Pediatrics.” (Wasserman et al 2011)“The RNZCGP Computer Research Network is a development of the Dunedin RNZCGP Research Unit. This unit was established in 1984 by a single $7000 grant from the RNZCGP, and is maintained by further research grants from peer-reviewed research funding agencies and the pharmaceutical industry.” (Dovey and Tilyard 1996) A special interest group within the national professional organization initiated the network “CORNET is the practice-based research network (PBRN) of pediatric resident continuity practices that developed from the APA Continuity Special Interest Group (SIG). In 1995, the Task Force of the Continuity SIG presented a workshop at the APA national meeting. In preparation for this workshop, more than 70 manuscripts of research studies completed in pediatric residency continuity practices were collated.” (Wassermann et al 2011) An academic department initiated the network “Recognizing that collaborative research networks were needed in California, the Division of Family and Community Medicine at the University of California, San Francisco (UCSF), discussed a proposal for collaborative research at its annual meeting.” (Osborn and Petitti 1988) More than one academic department initiated the network “In 1996, a joint proposal for funding a new network of research and development general practices was put to the regional R&D directorate by the three heads of departments of general practice in South Thames, Professors Sean Hilton (St George's), Roger Jones (UMDS) and Roger Higgs (King's), in collaboration with the two postgraduate deans of general practice education, Drs Ri Hornung and Alan Ruben.” (Carter 1998, p. 85) An academic department initiated the network and based the operations “UPRNet is a program of Michigan State University College of Human Medicine's Upper Peninsula campus, from which we receive infrastructure support.” (Pearls of Research 1998) An academic department together with a regional health authority initiated the network “The North Staffordshire General Practice (GP) Research Network was established by the Primary Care Sciences Research Centre (PCSRC) at Keele University, the North Staffordshire Health Authority, and local general practices in 1997.” (Porcheret et al 2004) A professional organization and the academic department initiated the network “The Oklahoma Academy of Family Physicians in collaboration with the University of Oklahoma Health Sciences Center established a primary care practice-based research network with thirteen family practice offices currently participating.” (Mold and Barton 1996) A clinical and translational science institute affiliated to a university initiated the network “The University of Rochester's CTSA-funded Clinical and Translational Science Institute established the Greater Rochester PBRN (GR-PBRN).” (Gibson et al 2010)“As part of an effort by the Community Outreach and Research Translation Core of the University of Washington's CTSA (the Institute of Translational Health Sciences—ITHS) to build a PBRN in the Washington, Wyoming, Alaska, Montana, Idaho (WWAMI) states, seven clinical practices in the University of Washington's (UW) Family Medicine Residency Network (FMRN) participated in a study of clinical importance to the practices that simultaneously built research capacity and infrastructure at the sites.” (Baldwin et al 2012) The academic department together with HIT vendors initiated the network “The PPRNet activities will be conducted under a set of operational procedures that are consistent with contracts between the Medical University of South Carolina (MUSC), IMS America, and Physician Mirco Systems Inc. (PMSI), and IMS America (IMS).” (Ornstein and Jenkins 1997) A consortium of research organizations initiated the network “FIMMG (FederazioneItaliana Medici di MedicinaGenerale), CSeRMEG (Centro Studi e Ricerca in MedicinaGenerale), CoS (ConsorzioSanità), Ass. Cu.M.I. (AssociazioneCulturaleMedicaInterdisciplinare), AMISI (Associazione per la MedicinaIntegrativa e la Sanità Integrata) and Istituto di RicercheFarmacologiche ‘Mario Negri’ supported and stimulated the interest in practice-based research activity. This collaborative will be the basis of the research infrastructure.” (Visentin 2005) The network was built upon existing networks “The Scottish Primary Care Research Network was finally built upon existing networks of teaching and training practices centered on research active departments of general practice and primary care. This meant that a climate already favorable to research existed and several of the necessary skills were available.” (Sullivan et al 2014) A national federation of PBRNs in collaboration with a PBRN and HIT infrastructure from a university initiated the network “The ePCRN integrates the practice-based research expertise from the community practices of the Federation of Practice-based Research Networks (FP-BRN) with the advanced “Grid” electronic infrastructure of the University of Minnesota (UM), and the Midlands Research Practices Consortium (Mi- dReC), one of the largest PCRNs in the United Kingdom.” (Peterson et al 2006) A group of community health centers initiated the network “CHCs [Community Health Centers] governed by patient boards, community advocates, and other safety net organizations from multiple communities formed a member-based, nonprofit collaborative, originally called the Oregon Community Health Information Network (renamed “OCHIN, Inc.” as members from other states joined), to facilitate adopting health IT and a learning environment to improve care quality for vulnerable populations.” (2013) “The PBRN…was housed at OCHIN to maximize its independence and focus on community-based research.” (DeVoe et al 2011) A public health agency and a national professional organization initiated the network “In 2006, the Canadian Institutes for Health Research funded a workshop at Queen's University, bringing together primary care researchers from across the country interested in building a national network. Representatives of the Public Health Agency of Canada (PHAC) were also in attendance and were looking for opportunities to establish primary care data sources for chronic disease surveillance.” (Birtwhistle et al 2009)
“In 2008, PHAC issued a request for proposal for a primary care sentinel surveillance system for chronic disease. The chronic diseases of interest were cardiovascular disease, chronic respiratory disease, mental health, arthritis, and diabetes. The CFPC's application was successful and the Canadian Primary Care Sentinel Surveillance Network (CPCSSN) was born.” (Birtwhistle et al 2009)A group of community stakeholders and a PBRN shared resource initiated the network “The DD-PBRN is a multistakeholder, community-based PBRN established in 2013 with the support of the PBRN Shared Resource at Case Western Reserve University through the National Institutes of Health–funded Cleveland Clinical and Translational Science Collaborative.” (Tyler and Werner 2014) A professional organization initiated the network and based its operations “The WRS developed out of the Royal College of General Practitioners' Epidemic Observation Unit.” (Fleming and Crombie 1985) A professional organization initiated the network and the academic department based the center of operations: “The Wisconsin network was initiated by the Wisconsin Academy of Family Physicians (WAFP) and is managed and receives support from the University of Wisconsin.” (van Weel 2000) A professional organization and an academic department based the center of operations “We have also established a central office at the CFPC [College of Family Physicians of Canada] for the project manager/director and support staff. The chair of the board of CPCSSN is currently at Queen's University, where the central repository is housed. In the future, however, the chair may be at another network so the funding for the office of the chair will float.” (Birtwhistle et al 2009) An academic department based the center of operations “The University Family Practice Network is composed of five practices and is managed jointly by the Department of General Practice.” (Laurence et al 2001)“The Primary Health Care Research Network (PHReNet) is being established by the University of NSW as part of the NSW Primary Health Care Research Capacity Building Program. This program is funded by the Commonwealth Department of Health and Aged Care to develop and support research and evaluation in general practice and primary health care in Australia.” (Mehmet et al 2004)“KAN is administered through the Department of Family and Community Medicine at the University of Kentucky in Lexington.” (Love et al 2006) HIT, health information technology; PBRN, practice-based research network.
- Appendix Table 2.
Identical PBRN Missions, Purposes, Goals/Focuses, Objectives, Aims, and Relevant Quotations
Missions Quotations “to explore the morbidity pattern in the Dutch population as far as it could be diagnosed in GP care, to signal diseases as well as shifts in disease patterns.” (Schweikardt et al 2016)
“to meet the need for a community based research ‘laboratory’ for child health research focused on issues central to the delivery of preventive pediatric care and across the spectrum of health and illness.” (LeBailly et al 2003)
“to facilitate practice-based research partnerships between academic researchers and community based clinical teams that can lead to improved primary care clinical outcomes.” (Jame et al 2015)
“to improve the health of children and enhance primary care practice by conducting national collaborative practice-based research.” (Slora et al 2006)
“to conduct and disseminate practice-based research that results in new knowledge and improves the health of patients in South Texas.” (Hayes et al 2011)
“to conduct practice-based research designed to improve health care in the United States.” (Ornstein and Jenkins 1997)
“to inform and influence decisions along the continuum of service to patients, from research to practice and policy.” (http://acornpbrn.org/mission/, accessed November 8, 2019)
“to conduct and facilitate practice-based research relevant to APRN primary care practice, develop culturally competent, evidence-based practice models for APRNs, and enhance the translation of research findings into primary care practice.” (Deshefy-Longhi et al 2002)
“to improve the quality and safety of health care in primary care settings by identifying and solving problems commonly encountered in practice.” (Kuo et al 2008)
“to generate new knowledge about basic pediatric issues of prevention and medical effectiveness—knowledge that can have a significant impact on the health of children.” (Del Torso et al 2010)
“Its mission is to support primary care research and education in order to improve the quality of care delivered to patients in the community in the West of Ireland.” (Kavanagh et al 2010)Purposes Quotations “Its purpose is the international study of problems and concerns presented at the level of the primary care to improve the understanding, organization, and implementation of appropriate health care for people throughout the world.” (Culpepper and Froom 1988)
“for the purpose of facilitating research on chronic disease and related health care problems commonly addressed in primary care settings.” (Sloane et al 2006)
“to demonstrate the impact of nursing centers on the health of communities; foster understanding, recognition, and use of nursing centers for essential primary health care; provide a forum for communication and collaboration among consortium members; and support the growth of nursing centers nationally.” (Anderko et al 2005)
“to offer a managed approach to hosting high quality research in the health service and to assuring recruitment and retention of study participants.” (Sullivan et al 2007)
“to improve the health and health care of underserved, low-income, multiethnic populations of the South-west.” (Sinclair-Lian et al 2008)
“to participate in clinical research for the benefit of their patients and to enhance the discipline of general practice through research training and activity.” (IPCRN, accessed May 17, 2017)
“to study problems as they present in the primary care setting and to increase the knowledge base regarding how modern primary care medicine is practiced.” (Iverson et al 1988)
“offers epidemiological information to the health service and the possibility of scientific research by the university departments.” (Middelkoop et al 1995)Goals/Focuses Quotations “To screen and facilitate the increasing number of researcher requests for Academy support in approaching family physicians about participation in their projects. To encourage and support individual or group research projects by its members. To train members in research methodology. To develop and coordinate research support resources for members.” (Solberg et al 1986)
“The main goal of the Transition Project is the analysis of the content of family practice in great clinical detail, for epidemiological purposes and to support quality assessment, health care policy, medical education and research.” (Okkes et al 2001)
“Focusing on research strategies for integrating epidemiological research, community-based primary care research and outcomes assessment in practices serving the medically underserved…To involve larger numbers of clinicians at health centers in community-based research.” (Sardell 1996)
“In our network the focus is on an intensive contact monitoring of patient diagnoses.” (Hak et al 1998)
“The SPAM network, with its focus on processes of care in PC and national representation, should be complementary to other efforts.” (Selby et al 2015)
“WH-PBRN specializes in multisite women's health research and recruitment of women to multisite, practice-based research studies.” (Frayne et al 2013)
“The chief goal of the Registration Network Family Practices is to establish a computerized database containing certain patient characteristics and all relevant health problems excluding minor, temporary illnesses.” (Metsemakers et al 1996)
“Investing in people. Recognizing that meaningful change is effected by motivated individuals and not systems alone. Creating an environment in which research is seen as a positive attribute and a necessity for the development of the profession.Preparing a structured support system for fostering research. Developing an education and career structure for practice-based researchers, including attachments and appointments, and help towards higher degrees and diplomas. Being part of an integrated drive towards research and development and to ensure representation for primary care researchers at policy making and resource allocation level.” (Carter 1998, p. 77)
“The overall CORNET research goals are to study the health care of minority and underserved children, to examine health care disparities, and to study resident education, with comparisons of physician behaviors between pediatric residents and pediatricians in practice.” (Serwint et al 2006)
“The overall goals of TARGet Kids! are:
1. to establish a ‘proof-of concept’ community-based primary care research network;
2. to learn from the ‘proof-of-concept’ experience and to scale up to a provincially-based network with sentinel sites to ensure representativeness;
3. to build partnerships between child health researchers, community-based practitioners and public health researchers and practitioners;
4. to build a platform to advance evidence for community-based prevention and health promotion;
5. to build a platform to advance population-level child health surveillance.” (Carsley et al 2015)
“Create a trusted, valued multi-state community of safety net stakeholders and researchers to lead and participate in a learning community to address evidence-gaps relevant to the safety net populations—with special emphasis upon those populations served by Medicaid and State Child Health Insurance Program (SCHIP”). (Sills 2015)
“The goals of CHARN are to:
• Foster practice-based collaboration among personnel, practitioners, and researchers at various clinics and centers;
• Create infrastructure for pooling patient data across different sites;
• Train CHC personnel in research methods and protocols;
• Develop and conduct study protocols;
• Expand the research agenda via additional funding; and
• Develop improved approaches for transferring research findings into practice.” (Likumahuva et al 2013)
“Goals of building GP research in the community. Develop professional development opportunities for GP supervisors and GP registrars. Goals of improving GP clinical academic's professional development.” (Dijkmans-Hadley et al 2015)
“Its goal is to promote the translation of research findings into policy and practice.” (Duggan et al 2013)Objectives Quotations
“To improve on knowledge of infectious diseases gained from the national notification system. The difference between notification and true incidence has been emphasized; To estimate the importance of other infectious diseases in general practice; To inquire into the field of health problems observed in general practice.” (Lobet et al 1987)
“The Primary Care Cooperative Information Project consists of a network of 44 free-standing primary care practices that are working with medical school faculty to (1) establish a professional environment that can help, attract, retain, and educate primary care physicians in a rural area, (2) develop practice based quality assurance systems, (3) improve management efficiency and heighten clinical cost consciousness in the daily practice of medicine, and (4) build a better system for continuing education based on practice self-study and cross-practice research.” (Nelson et al 1981, Part 1)
“Its objectives are to (1) develop a national home visiting research agenda, (2) advance the use of innovative research methods, and (3) provide a research environment that is supportive of the professional development of emerging researchers interested in home visiting.” “An overarching goal is to promote the translation of research into policy and practice.” (Duggan et al 2013)
“Support community physicians research. Support research interests of family physicians. Conduct collaborative research among family physicians. Train physicians in research methods. Provide access to community practices for (academic) investigators.” (van Weel et al 2000)
“to develop an epidemiological database for diseases to a central unit for Northern Ireland of morbidity within the community as presented to general practitioners. To support epidemiological research in general practice.” (Boydell et al 1995)
“The objectives of the network are: (i) to monitor trends in acute and chronic illness seen in primary care; (ii) to investigate the role of psychosocial factors in illness and disease; (iii) to examine aspects of medical practice, eg, the use of drugs, tests and procedures; (iv) to promote cost-effective management of medical problems in the community; and (v) to establish a databank for undergraduate and postgraduate training of primary care providers.” (Volmik et al 1996)
“The objectives are to co-ordinate research projects in general practice, to assist legitimate organizations and individuals undertaking research projects, to facilitate appropriate feasible and high-quality research being undertaken in practices, and to develop the skills and confidence of practices undertaking such research.” (Frew et al 2001).
“1. Develop an infrastructure for CPCSSN that will underpin the operations of a robust,longitudinal data collection and maintenance of a primary care data repository on chronic disease.
2. Demonstrate the ability to extract relevant data from multiple EMRs in multiple primary care practice sites.
3. Create a usable CPCSSN database that will be a searchable data repository for primary care researchers and will be the basis for reports for government and others about chronic disease in Canada.” (Birtwhistle et al 2009)
“to share data extracted from health information systems to facilitate professional collegiality and coordination of health services, quality monitoring and research and development to improve health documentation, patient care and health outcomes in an integrated health neighborhood.” (Electronic Practice Based Research Network, accessed January 7, 2020)
“Establish and maintain a broad, safety-net focused, research partnership and learning community to govern relationships, establish priorities, provide data quality oversight, and evaluate the purpose and value of the community's effort.” (Sills 2015)Aims Quotations “We aimed to develop a practical, ethical, long-term means of undertaking research in general practice by adjusting research methods to the everyday procedures of general practice teams, rather than asking doctors and nurses to change the way they recorded care in order to accommodate research requirements.” (Dovey and Tilyard 1996)
“Its aim has always been to provide an efficient and effective support network for all interested healthcare researchers in what are now the three North Cumbria PCT's; Carlisle & District PCT, Eden Valley PCT and West Cumbria PCT.” (Robertson et al 2005)
“The aim of the network is to promote a research and development culture through primary care in order to secure high quality, evidence-based, clinical care.” (Smith and Dunleavey 1996)
“The network aims to operate as a complex adaptive learning system (a whole system approach) by resolving a number of seeming paradoxes: There is a need for simultaneous ‘top down’, ‘bottom up’ and ‘coalition’ led research…The ‘whole system’ is big but resources permit only a small number of people to be involved at any one time…There is a need to harness individual enthusiasm but multidisciplinary working, quality and equity also need to be assured…Research needs to be focused and rigorous but reflective inquiring practice is a goal for all involved in primary care development.” (Thomas and While 2001)
“The overall aim of research networks is to support and promote high quality research aimed at improving the quality and cost-effectiveness of services offered by the NHS as well as securing lasting improvements to health nationally and internationally.” (Sullivan et al 2014)
“Known as ASPIRE or ‘A Singhealth Polyclinics Initiative for Research Excellence’, the committee aims to develop a comprehensive research program consistent with the vision and mission of the Singhealth network and to cultivate research culture in the polyclinics.” (Chuan and Gan 2001)
“The aims of the PCRN were: 1) To develop a culture of research in primary care in South West Scotland. 2) To provide research training. 3) To provide support for researchers in primary care. 4) To develop and conduct non-commercial research which would inform the provision of primary care.” (Hannay 2006)
“The major aim of the work of the MNCCRN is to discover new knowledge that will inform primary care practice, health professional education, and health care policy.” (Anderko et al 2006)
“One of the main aims of GRACE was to establish a multi-disciplinary network of research to address a complex problem and to establish an enduring European-wide primary care research network for future research.” (Nuttall et al 2011)
“To spur the development of important and high-quality primary care research that is relevant to clinical practice. To influence primary care policy making through its research.” (Soos et al 2010).
“Our aim is to improve the evidence for population health and primary prevention using a research platform embedded in primary care practice.” (Carsley et al 2015)
“The ongoing FIRE project (Family Medicine ICPC-Research using Electronic Medical Record) aims to embed standardized collection of research data by means of an EPR into routine clinical practice.” (Chmiel et al 2011)
“The aims of the Tutka network include developing research activity and capacity by learning, by researching together, by creating important research questions from the point of view of primary care health care professionals, by involving health centers in data collection, and by linking to external research projects.” (Tuomas Koskela 2017)GP, general practitioner.
Key Activities Name of PBRN, Nationality, and Quotations Initiating networks with routine collection of data The Nijmegen Family Practice Academic Network (NL): “The Nijmegen network collects patient-related data on an ongoing basis.” (van Weel 2000) “In a practice-based setting, data were collected concerning health problems patients presented to their general practitioner.” (van Weel 2008)
The Transition Project (Thanshis) (NL):
“54 FPs in 23 practices distributed over the Netherlands routinely collected and coded data for all face to face (direct) encounters with their listed patients.” (Okkes et al 2001)
GPDRP (UK):
“The project is a sentinel network of 23 general practices in Northern Ireland that report the incidence of a list of selected diseases to a central unit for analysis.” (Boydell et al 1995)
RNH (NL):
“This is a continuous and computerized database in which 42 general practitioners, working in 15 different practices in the south of the Netherlands, are participating. All relevant health problems are registered. A health problem is defined as ‘anything that has required, does or may require health-care management and has affected or could significantly affect a person’s physical or emotional well-being.''' (van den Akker et al 1998)
ASPN (USA and Canada):
“ASPN routinely collects and maintains data in four areas of network operations. First, all ASPN practices annually submit a report, which describes their active patient population,…ASPN collects data that update the characteristics of the practices and individual clinicians in ASPN…ASPN has replicated the National Ambulatory Medical Care Survey (NAMCS) in all practices and instituted by policy that requires NAMCS in all practices joining the network. Finally, ASPN practices report data on specific topics on a ‘weekly return card.’” (Green et al 1994)Initiating networks through specific projects CSeRMeG PBRN (Italy):
“A research project that is becoming the paradigm of the Italian research on General Practice. It started from a survey showing that treatment and control of cardiovascular risk is still far from optimal even in very high-risk patients. A group of general practitioners, coordinated by Istituto Mario Negri, wrote the protocol of the study with various proposals: Creating a research network.” (Visentin 2005)
GRACE-01 (International):
“We aimed to set up a European-wide primary care research network to deliver an ambitious observational study during one winter period. We succeeded in establishing a clinical platform for the GRACE 01 study, and many of the PCNs [primary care networks] have continued to recruit patients into subsequent GRACE studies. We achieved recruitment targets in many PCNs in GRACE 01. GRACE 01 continues to generate data that has clinical relevance.” (Nuttall et al 2011)
Tutka (Finland):
“The first study, focusing on the non-acute use of ECG in primary health care, has been carried out and infrastructure for future studies has been established.” (Koskela et al 2017)Initiating networks focusing on capacity building activities Trent Focus Collaborative Research Network (UK):
“The network commenced its activities with a detailed needs assessment exercise to identify the research skills and needs of practitioners.” (Comino 2002)
WeLReN (UK):
“The evidence suggests that it is possible to operate a primary care research network in a way that develops coalitions of interest from different parts of the health care system as well as both ‘top down’ and ‘bottom up’ led projects.” (Thomas and While 2001)
“The network aims to operate as a complex adaptive learning system (a whole system approach).” (Thomas and While 2001)
TayRen (UK):
“An early priority was to increase the research skills across the network by investing in a broad range of training, from critical appraisal skills, searching for evidence, managing data to detailed research methodology.” “As research expertise within the network increased, more novice researchers could be integrated into the network, have access to training in research skills and gain experience by working within project teams.” (Pitkethly and Sullivan 2003)
The Dumfries and Galloway Primary Care Research Network (UK):
“All primary care professionals working in the region were offered an initial grant to buy time for research training to develop their own research ideas.” (Hannay 2006)Initiating networks developing a survey SFBayCRN (ex-UCSF) (USA):
“Recognizing that collaborative research networks were needed in California, the Division of Family and Community Medicine at the University of California, San Francisco (UCSF), discussed a proposal for collaborative research at its annual meeting. A pilot study of more than 400 clinical faculty was conducted in spring 1985 by the Division of Family and Community Medicine, University of California, San Francisco, to identify physicians interested in participating in collaborative research.” (Obsborn and Petitti 1988)
ORPRN (USA):
“It was the goal of ORPRN to conduct a survey of its members to develop a comprehensive descriptive database of participating practices, clinicians, and patient populations.” (Fagnan et al 2007)EAPRASnet (International):
“Every pediatrician joining the network has been asked to complete a recruitment survey. The aims of the survey were to characterize pediatricians' demographics, practice arrangements and patients' demographics, to define main incentives for research, and to learn what pediatricians view as unsolved issues that need to be studied.” (Del Torso et al 2010)
WestREN (Ireland):
“In September 2009 all member practices were issued with a questionnaire with two objectives: to describe the structure and characteristics of the member practices and to compare the results to the national profile of Irish general practice.” (Kavanagh et al 2010)
CORNET (USA):
“the Task Force undertook a research study in 1999 that included a multi-site evaluation of pediatric residents' continuity experiences. CORNET was born when 42 continuity practices expressed interest and 36 programs completed the study, with over 1100 resident responses—a powerful demonstration of the potential and power of collaboration.” (Wasserman et al 2011)
GR-PBRN (USA):
“Before engaging practices in PBRN-related research, we surveyed physicians about practice-based research to assess facilitating factors regarding physician participation in practice-based research and to compare the perspectives of internists, family physicians, and pediatricians” (Gibson et al 2010)
SPAM (Switzerland):
“The Quality and Costs of Primary Care in Europe (QUALICOPC) survey served as a starting-point for creating the SPAM network.” (Selby et al 2015)Initiating networks with a survey to identify training needs and subsequent training WReN (UK):
“Before setting-up the network a survey was conducted of GPs in Wessex to estimate the level of interest in research and the perceived barriers to participation in research activity.” (Smith and Dunleavey 1996)
“WReN has identified primary care teams interested in research and provided training in research methods, provision of research support and opportunities for collaborative research” (Smith and Dunleavey 1996)
SARNet (Australia):
“We designed a survey questionnaire to assess network members' research experience and interest in developing further skills.” (Ried et al 2006)
“At the time of joining SARNet, members are sent a survey asking their specific interests and needs for research and evaluation training. Data from these returned surveys are now being used when planning courses and activities to be undertaken or repeated.” (Waters et al 2004)Initiating networks leveraging health information technology developments or aggregating electronic health data PPRNet (USA):
“The Practice Partner Research Network (PPRNet), a practice-based research network consisting solely of physicians that use Physician Micro Systems Practice Partner, CPR system.” (Ornstein and Jenkins 1997) “PPRNet involvement is voluntary and offered to all practices that use Practice Partner's EMR.” (Wessell et al 2008)
ePCRN (USA and UK):
“The electronic infrastructure of the ePCRN is being built on a web-enabled distributed database technology that makes use of cutting-edge web technologies such as the OGSA and WSRF. This allows creation of distributed clinical information systems located at the site of practice that can be appropriately and securely linked together. Exciting possibilities for this technology include the potential for patient eligibility searches across wide geographic areas, real-time video conferencing, implementation of medical record communication standards, and real-time clinician access to standard clinical performance measures.” (Peterson et al 2006)
DARTNet (USA):
“A federated network links geographically and organizationally separate databases so that a single database query can return results from multiple databases while maintaining the privacy and confidentiality of patient data.” (Pace et al 2009)
CPCSSN (Canada):
“In 2008, PHAC [Public Health Agency of Canada] issued a request for proposal for a primary care sentinel surveillance system for chronic disease.” “All of these academic primary care research networks had associated family medicine practices that used EMRs…Because of the work involved with assessing data extraction capabilities from individual EMRs, each network was restricted to recruiting up to 10 practices using the same EMR.” (Birtwhistle et al 2009)
IPCRN (Ireland):
“Through participation in the IPCRN, the extraction of anonymised patient prescribing records is possible through the integration of an electronic tool for remote data extraction into the General Practitioner's (GP) patient management software system.” (Galvin et al 2015)Initiating networks developing a patient cohort TARGet Kids! (Canada):
The development of an open longitudinal cohort of children enrolling from early childhood and following-up until adolescence. “The Applied Research Group for Kids (TARGet Kids!) is an ongoing open longitudinal cohort study enrolling healthy children (from birth to 5 years of age) and following them into adolescence.” (Carsley et al 2015)NC-FM-RN (USA):
“This paper describes the development of a different type of primary care research laboratory—a cohort of adult patients recruited from a representative sample of primary care offices and maintained for use on multiple projects. The cohort, the North Carolina Health Project (NCHP) research cohort, was developed by faculty of the University of North Carolina (UNC), in collaboration with the North Carolina Academy of Family Physicians, for the purpose of facilitating research on chronic disease and related health care problems commonly addressed in primary care settings. As such, it may represent a new model of primary care research infrastructure development—different from, and complementary to, traditional PBRNs.” (Sloane et al 2006)Initiating networks following other approaches or combinations of approaches HARNET (USA): Peer intellectual exchange and development of research questions
“The HARNET came into existence as an outgrowth of the Harrisburg (Pa) Hospital Family Practice Residency Program. In 1988, clinicians from six local practices (four suburban and semirural private practices and two residency-based family practice centers in urban and semirural areas) met to discuss their mutual interest in practice-based research. Clinicians from these practices teach in the family practice residency program. Initial discussions held at monthly faculty meetings centered on a list of clinical research questions arising from the members' practices.” (Slawson et al 1993)
CDN (USA): Development of a peer network for implementation of better practice and to start a big-scale research project
“Since the mid-1980s, clinicians working in community and migrant health centers formed clinical networks to provide administrative and clinical training, regular interaction with peers, and opportunities for participation in policy formulation. The subject of this article is the most developed of the regional clinical networks, the Clinical Directors Network of Region II (CDN),” (Sardell 1996)
“During its ten-year history, CDN has responded to the needs articulated by clinicians at health centers. It has provided managerial training and clinical education, strategies for increased involvement of clinicians in health center management and opportunities for engagement in community-based primary care research…
During the 1990s, CDN's annual conferences dealt with both clinical and managerial issues, focusing on strategies for integrating epidemiological research, community-based primary care research and outcomes assessment in practices serving the medically underserved. These conferences were linked to research activities in which CDN was involved and were part of efforts to involve larger numbers of clinicians at health centers in community-based research. CDN has, since 1989, functioned as a practice-based research network.” (Sardell 1996)
COOP (USA): Developing a forum of intellectual exchange and common software
“The core of the COOP project is development of a medical information system in all practices that is tailored to the requirements of each, yet contains a basic data set common to all participants in the network.” (Nelson et al 1981, Part 1)
“As a forum for intellectual exchange, the COOP has enabled clinicians to serve as sources of information for each other, which has affected clinical practice.” (Mold and Peterson 2005)
ASPIRE (Singapore): Developing a forum of communication for potential researchers
“It [the network] serves as a forum of communication for potential researchers, a platform to exchange research ideas and a base for methodology capacity building and collaborations with external research agencies.” (Chuan and Gan 2001)
MAFPRN (USA): Developing a research panel
“In 1978 the MAFP's Committee…decided the participation in practical research was one of the best ways for practitioners to continue their educational growth. In order to foster this participation, the committee formed a small research panel of interested practitioners…This research panel's goals included (1) increased research acceptance and skills by practicing doctors, (2) development of a list of practitioners interested in research, (3) development of a technique for multiclinic collaborative projects, and (4) completion of several practical demonstration studies that would produce information about the problems and activities of practitioners.” (Solberg et al 1983)
RRNeT (USA): Linking residents to practice-based research activity
“Each year, RRNeT recruited medical students through various events and assisted them with applications to the dean's program, focusing on the current RRNeT study. Since 2006, RRNeT recruited 40 UTHSCSA medical students, four to eight per year.” (Burge and Hill 2014)
OKPRN (USA): Sharing resources
“OKPRN currently includes thirteen family practice offices across Oklahoma connected by computerized e-mail and a mission to share resources, support decision-making in private practice, and conduct research.” (Mold and Barton 1996)
SPCRN (UK): Leveraging previous PBRN experience and active in training and teaching practices
“The Scottish Primary Care Research Network was finally built upon existing networks of teaching and training practices centered on research active departments of general practice and primary care. This meant that a climate already favorable to research existed and several of the necessary skills were available.” (Sullivan et al 2014)
OCHIN (ex-Safety Net West) (USA): Development of patient-centered medical village (community centers network) with a shared EHR enabling data aggregation and colearning
“One model of shared IT resources and learning is a “patient-centered medical village…the OCHIN Community Health Information Network is an example of this model; community practices have come together collectively to form an organization that leverages shared IT expertise, resources, and data, providing members with the means to fully capitalize on new technologies that support improved care.” (DeVoe et al 2013)“The opportunity to harness data from many practices was another major facilitator of our PBRN's development and echoes others' observations about the power of networks to collect data on large numbers of diverse patients. Our PBRN's data on a large patient population is in one shared and linked EHR which is centrally maintained and housed at OCHIN. This unique data resource helped to catalyze the formation of our PBRN and obtain some early grants to conduct secondary data analyses.” (DeVoe et al 2012)
“The collaborative and its member groups also provide a structured environment with peer mentors and a shared EHR to enable practices to come together, share their individual innovations, and spread them across the network.” (DeVoe et al 2013)
CHARN (USA): Providing research capacity and infrastructure
“CHARN offers opportunities to bridge clinical practice and academic environments to improve research infrastructure and capacity.” (Likumhuva et al 2013)
ISPRN (Australia): Development of relationships and communication pathways
”The framework developed by Barnett et al (2012) was found to be more useful in its application to ISPRN, which had a better balance of face-to-face interaction than online interaction, when the seven principles were collapsed into five…: (1) the establishment of a recognized leader (to promote and facilitate research idea development); (2) the development of relationships (between network members and stakeholders); (3) the evolution of communication pathways (through various mediums); (4) the collaboration of CoP members involved in developing shared goals and objectives; and (5) the role of evaluation in improving the CoP.” (Dijkmans-Hadley et al 2015)
DD-PBRN: Collaborative management, problem solving, and cocreation in training
“The idea of a DD-PBRN slowly emerged following years of affiliation between constituent members…It developed in the context of a series of success experiences in which future PBRN members engaged in tasks beyond the scope of their usual daily work, for example, co-creating training and clinical resources and educating health professionals.” (Tyler and Werner 2014)
“self-advocates, family members, and service providers began to see a role for themselves as vitally important educators of physicians. Many became involved in ongoing training of resident physicians at their local family medicine residency training programs. They recognized that the education of health professionals was a concrete means of ensuring and advocating for better health care.” (Tyler and Werner 2014)
“Mutual respect and understanding further developed between members of these 3 communities through collaborative management of complex client situations in which extensive communication and problem-solving between groups were required.” (Tyler and Werner 2014)
HVRN: Advances of implementation science and input of stakeholders
“Advances in dissemination and implementation science and comparative effectiveness research can and should be applied to home visiting. These advances include conceptual frameworks, operationalization of framework components, approaches to match administrative data, and development of designs and analytic techniques to test multilevel factors for the dissemination, implementation, and sustainment of innovations.”
“In summary, a rigorous program of research is needed to advance the field of home visiting. Such a program should draw on advances in implementation science, input from stakeholders, and the experience of practice-based research networks.” (Duggan et al 2013)
e-PBRN (Australia): Data extraction from EHRs and an integrated care model implementation
“Electronic health records (EHR) of all patients are extracted routinely from the general practices (3 using MD3, one originally used MD2 and one using Practix) using GRHANITETM and sent encrypted to a secure data warehouse at the University of NSW.” (Taggart et al 2012)
“The overarching conceptual framework highlights the socio-ecological complexity that influences the sharing and use of skills, information and resources to maximize the benefit to the patient, community and health system over time. It includes elements identified in the review of integrated care programs…Effective integrated care requires a transformational change towards teamwork, information sharing and work practices; a systems approach to managing chronic disease; eHealth; and continuous quality improvement with ongoing monitoring and evaluation. Higher level policy drivers include reforming health care financing to promote and sustain multidisciplinary integrated care.” (Liaw et al 2011)WPRN (USA): Leveraging existing strengths from QI activities and data sharing HIT infrastructure“Developing a practice-based research network (PBRN) with a model that integrates research and QI builds on the existing strengths of QI efforts, adding research incrementally rather than building a research program from the ground up.” (Baldwin et al 2012)
WPRN (USA): A HIT infrastructure of data sharing across practices
“Our CTSA efforts at the University of Washington's Institute of Translational Health Sciences (ITHS) include the Locally Controlled Data QUery, Extraction, Standardization and Translation (LC Data QUEST) pilot project aimed at creating data sharing capacity within the Washington, Wyoming, Alaska, Montana, Idaho region across primary care based practices.” (Stephens et al 2012)
ACORN (Australia): Developing a survey across the practitioners and developing a database of research interested practitioners
“One major task for the ACORN Project Steering Committee was to decide the method by which to recruit registered chiropractors via the invitation pack (database questionnaire and ACORN national practitioner database consent form).” “the ACORN project initially employs what we call a sub-study model to PBRN design whereby initial data collection is focused exclusively on practitioner-relevant information collected via self-report aimed at establishing a practitioner PBRN database.” (Adams et al 2016)
ULEARN-GP (Ireland): Developing a profiling survey and in-depth interviews on research engagement on GPs
“A profiling survey questionnaire was posted and e-mailed to all practices affiliated with the University of Limerick Graduate Entry Medical School…The profiling questionnaire used in the study gathered demographic details on practices, including details on practice staff, organization, size and academic activity…GPs affiliated with the University of Limerick-Graduate Entry Medical School were invited by email to participate in an interview.” (O'Regan et al 2020)
PPHAG PBRN (Samoa, Tonga, Cook Islands, Niue, and New Zealand): Developing a community advisory board to be the basis of the PBRN
“Over the next year, Rose recruited a group of Pacific Island community members, and formed the Pacific People's Health Advisory Group (PPHAG). Members were invited from personal and professional networks, reflecting the core values of connectiveness and relationships in Pacific cultures…PPHAG members discussed their areas of possible research interest over the next few months…Co-design and action research were explained—where research is actively done by, with, and for the stakeholders who will benefit from it, such as patients, community members, and clinicians, rather than done on them.” (Lamont et al 2020)EHR, electronic health record; FP, family physician; GP, general practitioner; HIT, health information technology; PBRN, practice-based research network; QI, quality improvement.
Topics of research training “At the first STaRNet teaching session a research methods resource pack was distributed to each lead practice. This was developed by the STaRNet project team, and included information, references and key articles on: literature reviewing, questionnaires and surveys, qualitative research, epidemiology, clinical trials, evaluating healthcare, health economics research, statistics, ethical issues, writing up and disseminating research, applying for funding and using the Internet in research. A second resource pack was developed on evidence-based healthcare to support the STaRNet lead practices in their work on implementing clinical guidelines and developing evidence-based practice. The pack provided references to key publications and detailed information about groups and resources concerned with evidence-based healthcare and included sections on: an overview of the evidence-based healthcare movement, how to find research evidence, critical appraisal, systematic reviews, guidelines, audit and managing change.” (Carter 1998, p. 90–1). - Appendix Table 5.
Example of Synthesis of Key Element “Relationship Building between Academics and Practitioners in the Field”
Subthemes Key Elements Components Related Quotations Network infrastructure and operations Relationship building between academia and practitioners Long-term relationships “This entire recruitment process involves relationship building, not just for CaRESS [study] but also for KAN. This defining feature of a PBRN, the long-term relationship with the clinicians, is the context for all our contact and decisions with the practices.” (Love et al 2006)
“The organizational model developed for the MNCCRN is one that builds on long-standing relationships with community groups, other health care providers, and organizational linkages that will facilitate trust, increase communication, maximize the use of limited resources, and enhance the dissemination of new knowledge generated to multiple constituencies, including consumers, health professionals, and policy makers.” (Anderko et al 2005)Development of common identity “ASPN conducts an annual convocation of its practices. The primary objectives of this meeting are to get acquainted; share information; develop an “esprit de corps” among network members; review, modify, and approve studies; and generate new study ideas.” (Iverson et al 1988)
“We have two meetings a year, because—unlike WReN—we have a very tightly knit group. The doctors and nurses and their support staffs know that they are in UPRNet, and therefore most UPRNet practices participate in most UPRNet studies…we are, after all, a small, regional, highly committed group.” (Pearls of Research 1998, p. 72)
“Appropriate resources should be identified for face-to-face meetings/teleconferences and annual events, since getting to know fellow researchers within a network helps to attract commitment and a sense of common purpose and camaraderie. An interactive (rather than didactic) approach to training a multilingual group worked well.” (Nuttall 2011)
“What is not captured in this description of the formal program is the value of WReN members meeting as a group, this is much better reflected in the many compliments received from participants.” (Smith and Dunleavey 1996)
“establish annual network meetings, which will provide a sense of ‘family’ of like-minded practitioners with a common purpose to network members.” (Deshefy-Longhi et al 2002)Based on common mission “CHCs [community health centers] are ideal partners with whom to conduct patient-centered outcomes research because they engage in quality improvement and evaluation with a mission to provide efficient and effective care that advances health and reduces disparities.” (Likumahuva et al 2013) Collaborative philosophy “The collaborative nature of ASPN means that the results are not the property of any one center or any one individual but belong to all involved and should be published under the aegis of ASPN.” (Green et al 1984) Matching practitioners and researchers with common interests “‘Matchmaking’ providers and researchers with common research interests using as liaisons the PBRN coordinators, community research liaisons to build personal relationships. Likewise, clinic champions operated as liaison for their clinic.” (Likumahuva et al 2013) Building research relationships upon the enthusiasm of researchers and practitioners “building upon the enthusiasm of researchers and clinicians at the geographically dispersed sites will be key, so as to assure that these busy professionals with competing priorities remain engaged over time.” (Frayne et al 2013) Collaboration across various disciplines and levels of seniority “Of particular note is the heartening and consistent multidisciplinary mix of all WeLReN activities but the difference between the doctor:nurse ratio in Theme Group and Expert-Led projects is noteworthy (2:1 vs 6:1). The WeLReN approach facilitates team working across traditional boundaries and across different levels of seniority which may make it easier for research activity to be enhancing of local education and service development activity, through the desirable development of informal inter-organizational connections.” (Thomas and While 2001) Mutual appreciation between practitioners and academics “While a motivating factor of other PBRNs, our two ‘different worlds’ do not always understand each other, possibly because our PBRN is based in the community rather than an academic setting. Building cohesion among PBRN clinicians and researchers required time to develop relationships so that our clinicians and researchers better appreciate each others' worlds.” (DeVoe et al 2012) Strong bonds between academia and practitioners “Its success is mainly contributable to the participating GPs' strong academic bonds, to its relatively small size, and to its consistent emphasis on completeness of data and, by organizing monthly meetings, on the assurance of data validity.” (Schers 2008) Constructive relationship between practitioners and academics “The objective of the first set of clinical and management studies presented in the preceding section were to do the following: (1) form a constructive relationship between medical school faculty and community physicians.” (Nelson et al 1981, Part 2) Relationships with key practitioners and practice managers “Other ways that ISPRN has developed relationships over time in the organization and implementation of projects has been through establishing a dual relationship with the practice manager and key GPs involved in the project.” (Dijkmans-Hadley et al 2015) Collaborative relationship focused on practitioner interest “The first premise is that COOP Project aims to meet the educational, managerial, and research interests of primary care physicians. It is a collaborative effort involving a medical school, community practices, and policy makers, but the direction of the COOP Project is determined by interest of the physicians.” (Nelson et al 1981, Part 1) Maintaining respectful and trusting relationships “the core tenet of successful PBRNs is developing and maintaining respectful and trusting long-term relationships that continue beyond research studies.” (Hayes et al 2011)
“Over the course of years, members of the disabilities and service communities slowly developed trusting relationships with a small cadre of physicians who demonstrated expertise and commitment to this population. Mutual respect and understanding further developed between members of these 3 communities through collaborative management of complex client situations in which extensive communication and problem-solving between groups were required.” (Tyler and Werner 2014)Networking and interaction “In addition to opportunities to increase knowledge and skills in clinical and managerial areas, CDN's conferences and workshops also provide opportunities for professional peer networking and interaction. According to CDN activists, sharing experiences and ideas with colleagues who work in similar organizational environments and respond to the needs of similar patient populations helps to enrich professional life.” (Sardell 1996) Efforts to increase trust “Strong leadership and frequent communication meant that NNCs [National Network Coordinators] and NNFs [National Network Facilitators] got to know well and grew to trust the GRACE-01 coordinating team.” (Nuttall 2011) Development of trust and boundaries about data sharing “Building a PBRN with a common EHR, or the ability to merge data from multiple EHRs into a common repository, requires that trust and boundaries around data sharing be established.” (DeVoe et al 2012) Sharing experiences “This unit provided a forum for general practitioners interested in the epidemiology of common infectious diseases to share experiences about the spread and the impact of conditions diagnosed and treated in their practices.” (Fleming 1999) Leveraging personal relationships “Another advantage of regional networks is that a more personal relationship with physicians, office staff, and patients is possible. Physicians and their office staff members generally know the PPRG staff personally.” (LeBailly 2003) Fostering collegiality “Fostering ongoing research relationships and a sense of camaraderie that advances the cause of child research and invigorates participating clinicians.” (Slora and Wasserman 2010)
“A shared sense of the importance of the research questions to improving clinical care was the foundation for establishing a common purpose and a spirit of camaraderie.” (Nuttall 2011)Support the links between practice and research “The 3 networks expressed the need to support routine practice, do research, and, at the same time, raise the quality of care in the network. An integral relationship between practice and research is apparent in each of the networks.” (van Weel 2000) Leveraging the prior relationships with academia “Two rural practices with residency graduates of the University of Missouri expressed an interest in collaborating. In addition, the Department of Family and Community Medicine sponsors two rural satellite practices which are used as educational bases for residents.” (Williamson et al 1998) Leveraged relationships with teaching practices “The network is both a research and teaching network. Interestingly enough, however, we have done more research than teaching.” (Pearls of Research 1988, p. 72) Collaborative relationship based on the strengths of each part “The combination of a central university faculty, which has an understanding of research methods and design, statistical analysis, and grant writing, with rural practitioners, who have “real world” practices, values, and clinical institutions, is a good one. This type of collaboration is professionally satisfying and is likely to result in valuable new primary care knowledge.” (Williamson et al 1998) Synergies developed during training “Since beginning collaborative working in 2002, a synergy has developed between CumbReN and HRDNoW [Health R&D North West] that has helped build research capacity at an individual and organizational level within the North Cumbria PCTs.” (Robertson et al 2005) Synergy and collaboration developed during research process “The network enables primary care practitioners with interesting clinical questions to work with expert researchers. From this synergy have developed large R&D projects of national importance.” (Smith and Dunleavey 1996)
“The investigator and one provider then engaged another physician, both of whom were not previously involved with research. Collaboratively, they developed a project to address clinical questions they had encountered in practice.” (Likumahuva et al 2013)Synergy developed through bidirectional collaboration “WH-PBRN…represents a long-term partnership of clinicians and researchers who together strive to improve the health and health care of women Veterans. Powerful synergies arise from this bi-directional collaboration, which aligns the perspectives and experience of clinicians and researchers.” (Frayne et al 2013) Cycles of collaborative activity The cycle can itself be viewed as participatory action research in that collaborative cycles of reflection, inquiry, feedback and action occur in each project and throughout the network.” (Thomas and While 2001) Collaboration with other research interested groups out of primary health care “NoReN's activities are geared towards research training, mentoring and fostering collaborative research. Specific activities during 1997 included…Providing an interface with other local groups, eg, hospital research committees.” (Carter 1998, p. 80–1) Collaboration among all stakeholders “Collaboration is the key to ACORN's success, relying on strong partnerships with practices, health systems, other universities and PBRNs, community organizations, businesses, insurers, and public health entities. Our relationships help to inform study ideas, carry out interventions, interpret and disseminate findings, and ensure that positive transformative methods found are implemented into practice.” (ACORN, accessed June 28, 2020) Partnering for shared learning and best practices implementation “Partnering with OCHIN, researchers, and payers, many practices are organizing themselves as Patient-Centered Medical Homes. We envision a synergy between practice transformation and research activities, strengthened by a ‘learner’s bridge' that provides opportunities for community partners to learn the skills for implementing and evaluating practice interventions…This type of partnership ensures that meaningful activities will be documented and will contribute to the growing fund of knowledge about evidence-based, best practices in primary care. Further, engaging learners in this partnership further strengthens the benefit for spread of innovation and sustainable future change.” (DeVoe et al 2011) Development of relationships with vendors (or HIT stakeholders) and members “Our system architecture design was a result of partnerships between multiple stakeholders including our CTSA, community practices and tribal partners, and national research communities. Developing the LC Data QUEST data sharing architecture involved significant time and effort in creating and sustaining relationships among all partners involved and required an iterative process to allow stakeholders to give valuable input into system requirements.” (Stephens et al 2012) The relationship with the network is beneficial for the members “Maintaining an engaged and productive network that is able to provide high reliability research activities and attract potential investigators requires a skilled and committed central organizing body to facilitate collaboration, to lessen the burden of research participation for practices, and to govern the network such that that all members receive benefits from participation.” (Pace et al 2014) Linking through research assistants, research facilitators, clinician champions Clinician champions: “Members of the clinician committee, who are physician champions from participating clinics, may vary from project to project. Physician champions inform their colleagues about the study and help solve logistical problems that arise during the project.” (Kuo 2008)
Coinvestigators: “To ensure consistency of intervention and reliability and validity of data, there must be a seasoned coinvestigator at each site who is ultimately responsible for each research study, in collaboration with CNC clinicians.” (Anderko et al 2005)
Research assistants/facilitators for research: “These assistants identify and exchange ideas, methods, questions, and challenges between practices within their pod and, through the central office, to the rest of the network; facilitate QI; and assist practices to participate in network-wide projects and for the research results implementation in practice.” (Mold and Peterson 2005)
“…the Oklahoma Physicians Resource/ Research Network (OKPRN) uses five full-time equivalent (FTE) facilitators, called practice enhancement assistants (PEAs). The PEAs help member practices participate in individual and network-wide research and quality improvement projects. Initial PEA training includes a comprehensive introduction program followed by project-specific training.” (Nagykaldi et al 2005Relationship brokering “Since our network would not be able to depend on much income, it should serve primarily a brokering function, bringing together researchers and interested practitioners for specific studies that are financially supported by the researchers.” (Solberg et al 1986)
“In research linking primary care practitioners and hospital-based consultants, complementary strengths can be linked, thereby improving the potential for understanding the natural history of disease.” (Christoffel et al 1988)Key tips for relationship building, mentorship, and leadership “Cultivate and support; Leaders and collaboration; Share resources; Build bridges and partnerships; Add value in multiple differing spheres.” (DeVoe et al 2012) Challenges deriving from practice comparisons “PBRNs must take precautions to avoid group comparisons so that ‘low performers’ are not embarrassed or jeopardized.” (Kuo 2008) Challenges related to relationships maintenance “Maintenance and updating of contact information on cohort [patient] members requires ongoing effort.” “There are, however, challenges involved in this type of infrastructure development. They include involvement of practitioners, minimization of selection bias, and maintenance of funding to support the network and cohort infrastructure.” (Sloan et al 2006) Subthemes Key Elements Components Related Quotations Network infrastructure and operations Organizational leadership Characteristics of a PBRN leader Recognized and enthusiastic leaders: “A worthy project such as an APRN research network requires recognized spokespersons in primary care research who are well regarded in both the nursing and medical fields for the importance and integrity of their work. They need to be relatively established in an academic setting that recognizes and supports their research and allows them ready access to other leaders in their field, both nationally and internationally. They must be willing to make the time to start such a project and must have the energy and enthusiasm to see it through. For an APRN research network, they need a clear vision of such a network, a solid perspective of both its promise and limitations, and a sense of humor to communicate that vision to fellow colleagues and staff.” (Deshefy-Longhi et al 2002)
“Generally the network has no track record other than the reputation of its director and the members of its planning committee.” (Deshefy-Longhi et al 2002)Leaders with engagement and motivation:
“PBRNs also require a champion that has the knowledge, energy, enthusiasm, and commitment to share the PBRN's vision with others.” (Deshefy-Longhi et al 2002)
“The former National Association of School Nurse's (NASN) Research Consultant who had worked with other PBRNs served in this capacity.” (Vessey et al 2007)Leaders and/or founders with senior academic and clinician background “The network Director is a long-standing GP in the area who now has a senior academic role with the Graduate School of Medicine, University of Wollongong. The Director, as a GP peer, provides an experienced perspective regarding the reality of implementing research within general practice.” (Dijkmans-Hadley et al 2015)
“Visible leadership by the university and hospital Chairman of Pediatrics (J.A.S.) has helped to provide authority and prestige to the organization.” (Christoffel et al 1988)
“The PPRG was founded in 1984 by Katherine Kaufer Christoffel, MD, MPH, in partnership with leaders in the Department of Pediatrics.” (LeBailly 2003)
“In the case of WreN, the initial organizer was a physician in an academic setting who was able to arrange for protected time to facilitate the network development and who had ready access to secretarial and related support services.” (Beasley 1991)Leader is academic professor in the department “The appointment of a professor of primary care research and development at the Tayside Centre for General Practice coincided with this successful bid.” (Pithketly and Sullivan 2003) Leader has previous PBRN experience “I have been involved with practice-based research for more than 17 years on several levels. I have been an Ambulatory Sentinel Practice Network (ASPN) clinician since 1982, an ASPN board member since 1993, and ASPN's president since 1997.” “I cofounded the Michigan Research Network (MiRNet) in 1984.” (Pearls of Research 1998, p. 72) Leadership providing critical momentum for capacity development and research activity “The combination of factors—a multi-state network of safety net clinics, an EHR with rich data linked across the network, and support from OCHIN's leadership—provided momentum for developing capacity to improve care quality in the safety net by optimizing practice through research.” (DeVoe et al 2011)
“…as described in the quality improvement and practice transformation literature, engaged leadership and a willing champion within each individual practice (eg, quality improvement leader or office manager) helped to maintain momentum, to demonstrate the value of the data for improving quality of care, and to provide audit and feedback to providers and staff.” (Kwan et al 2016)Leadership with interest to improve practice and influence policy “OCHIN leaders had a vision that extended beyond supporting the delivery of clinical care in safety net settings. There was interest in developing resources to improve practice and to influence policy.” (DeVoe et al 2011) Key recommendations for leadership “Cultivate and support; Leaders and collaboration; Share resources; Build bridges and partnerships; Add value in multiple differing spheres.” (DeVoe et al 2012) EHR, electronic health record; HIT, health information technology; QI, quality improvement.
In this issue




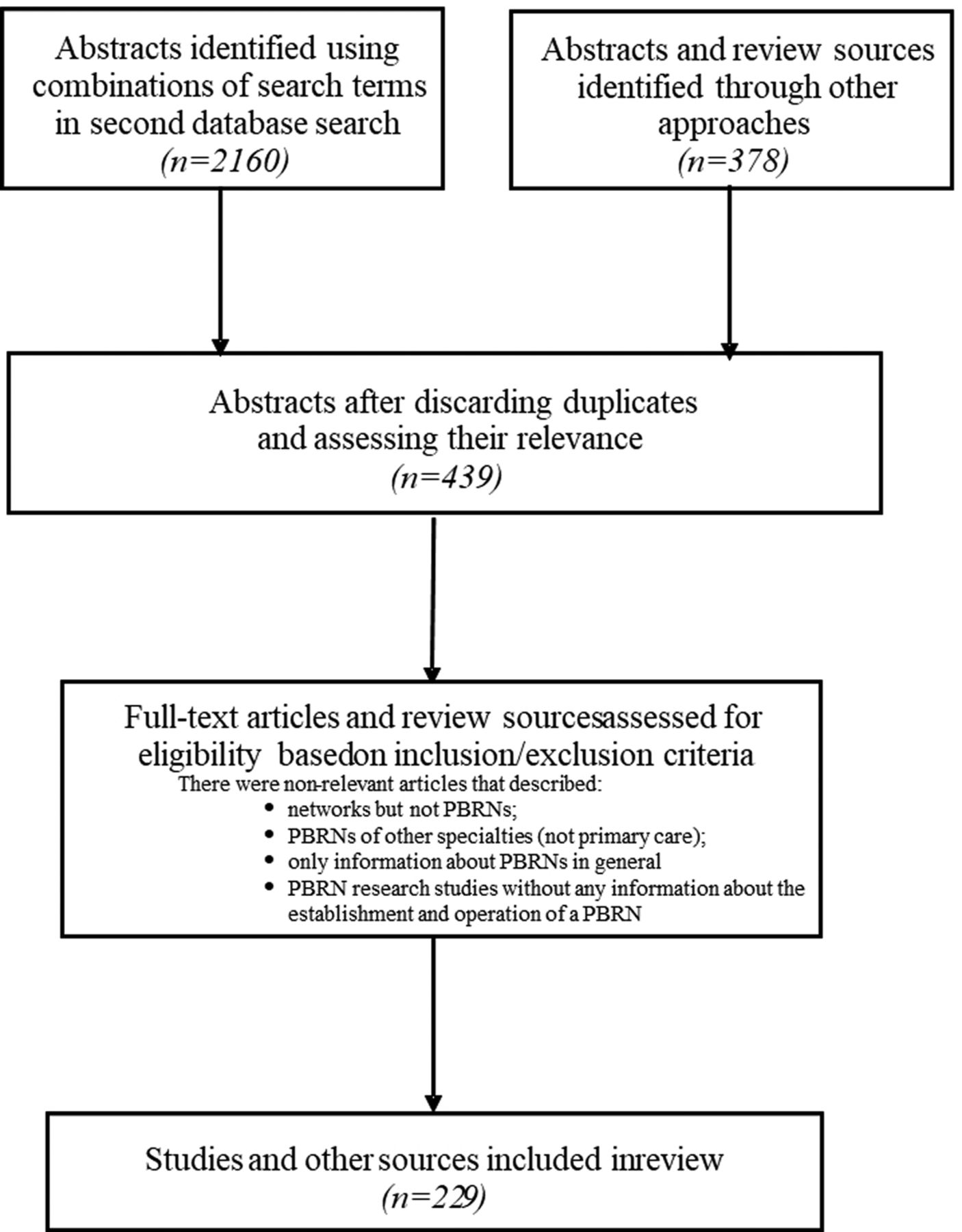{kind=link}
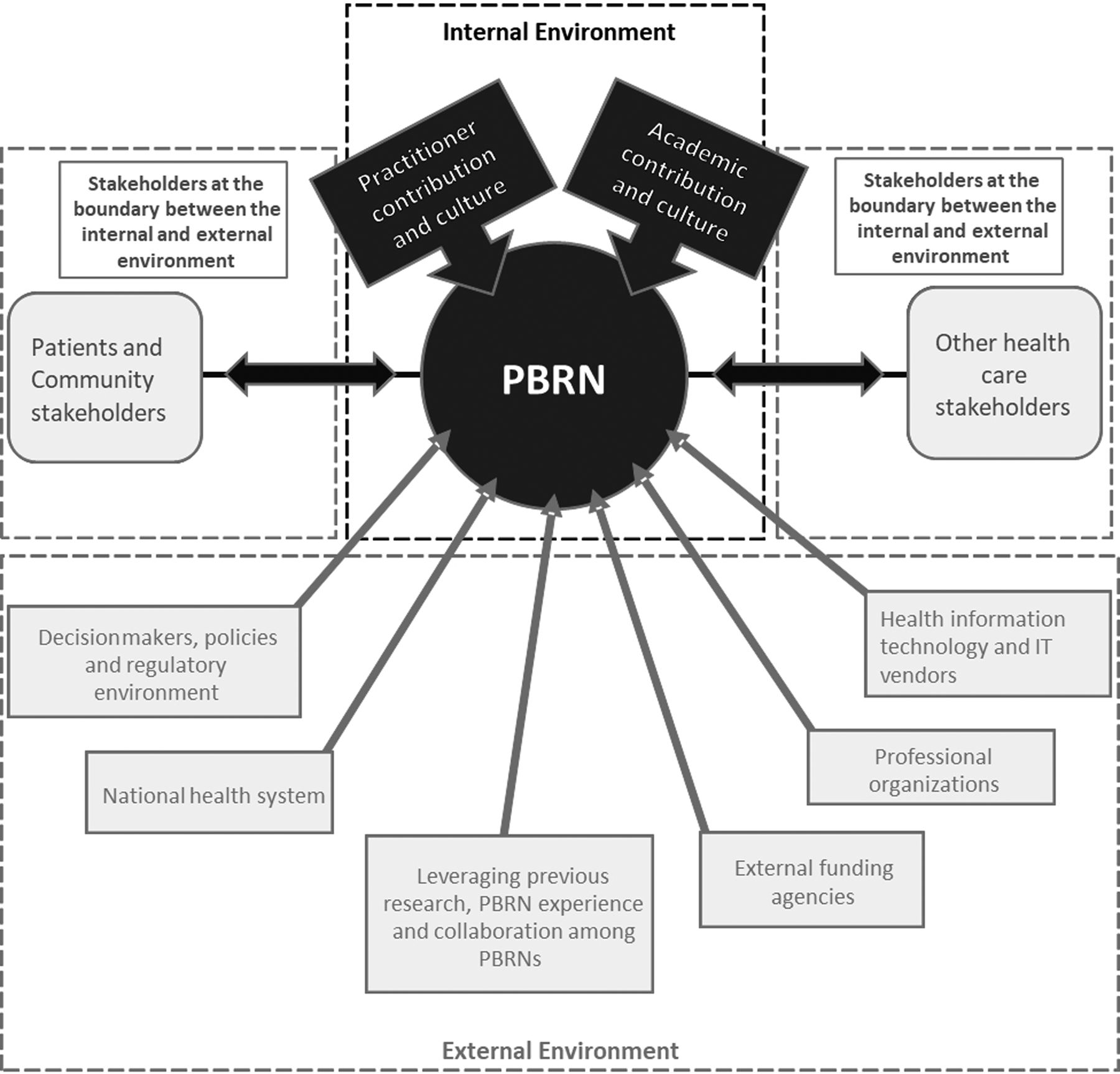{kind=link}
Jump to section
Related Articles
Cited By...
- Looking Back to Move Forward: Reflections of PBRN Directors
- A Review of 50 Years of International Literature on the External Environment of Building Practice-Based Research Networks (PBRNs)
- Building a practice-based research network for healthcare integration: a protocol paper for a mixed-method project
- Family Medicine Research on Health Equity, Addiction, and Eating Breakfast--Just for Starters