
Abstract
Purpose: Practice-based research networks (PBRNs) have developed dynamically across the world, paralleling the emergence of the primary care discipline. While this review focuses on the internal environment of PBRNs, the complete framework will be presented incrementally in future publications.
Methods: We conducted a scoping review of the published and gray literature. Electronic databases, including MEDLINE (PubMed), OVID, CINAHL (EBSCOhost), Scopus, and SAGE Premier, were searched for publications between January 1, 1965 and December 31, 2020 for English-language articles. Rigorous inclusion/exclusion criteria were implemented to identify relevant publications, and inductive thematic analysis was applied to elucidate key elements, subthemes, and themes. Social network theory was used to synthesize findings.
Results: A total of 229 publications described the establishment of 93 PBRNs in 15 countries that met the inclusion criteria. The overall framework yielded 3 main themes, 12 subthemes, and 57 key elements. Key PBRN activities included relationship building between academia and practitioners and development of a learning environment through multidirectional communication.
Conclusions: PBRNs across many countries contributed significantly to shaping the landscape of primary health care and became an integral part of it. Many common features within the sphere of PBRNs can be identified that seem to promote their establishment across the world.
- Bibliometrics
- Communication
- Family Medicine
- Practice-Based Research Network
- Primary Health Care
- Quality Improvement
Introduction
Practice-based research networks (PBRNs) are collaborations of researchers and primary care practitioners who are engaged in conducting health/care research, addressing questions and problems that emerge from daily practice, translating research findings into evidence-based practice, and improving the quality of healthcare.1⇓⇓–4
The seminal idea of PBRNs was planted in the UK in the late 1800s, first by James Mackenzie, and later by Will Pickles and John Fry, who conducted research in their own practices.5 Starting in 1967, this effort became more systematic through the Royal College of General Practitioners Weekly Returns Service in Birmingham, UK, which systematically gathered morbidity data from specific practices.6 In the USA, Curtis G. Hames conducted observational studies in family practice settings in the early 1970s,5 while A. Huygen initiated research activities at first in his practice just after World War II and soon engaged 4 Dutch family practices in the Nijmegen area in1967.7 Since these early experiences, primary care research has expanded to more countries and healthcare settings, and many PBRNs have sprung up worldwide.4,8⇓⇓⇓⇓–13
Through the course of 5 decades, PBRNs developed new scientific knowledge and various health care innovations,14⇓–16 new research methodologies,17⇓–19 innovative Health Information Technology (HIT),20⇓⇓–23 and healthcare improvement programs that were, in some cases, supported by national legislation.24⇓⇓–27
While several publications exist describing the development of individual PBRNs or geographically clustered PBRNs (eg, at the regional or national level), there is a paucity of information about the establishment of PBRNs across the world and over 5 decades. The purpose of this study was to address this gap by conducting a scoping review of the worldwide English literature to synthesize what is known about the establishment of PBRNs and by constructing an overarching thematic framework, which has not been established before. This also allowed us to map the facilitators and barriers of building PBRNs based on the entire discoverable body of PBRN literature.
Due to the extent of our findings, the focus of this article is on the internal environment of PBRNs. Results derived from other domains (eg, the external environment) will be presented in subsequent publications.
Methods
We conducted a scoping review of the literature following a methodological framework described by Arksey and O'Malley,28 which was appropriate to map the key elements that underpin our area of interest, spanning across a broad scale of source data. This method is particularly suitable to examine a comprehensive set of data sources and various types of evidence that may be available, such as electronic databases, reference lists, manual searches of individual journals, online information on existing networks, organizations, and conference proceedings. This allowed us to search across the “universe” of PBRNs and any information that was accessible on their establishment.
We then applied analytic stages suggested by the chosen method: (1) defining the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, (5) collating and summarizing the findings, and (6) reporting the results. The purpose of conducting the scoping review was to identify key elements that were linked to the establishment of PBRNs and to create an overarching thematic framework that contextualizes the facilitators and barriers of this process. Our qualitative scoping review approach did not include a quality assessment of the examined articles, since we intended to incorporate any verifiable information available.
Identifying Relevant Studies and Study Selection
We identified relevant publications in 2 steps. In the first step, we searched the English-language literature systematically and reviewed publications listed in MEDLINE (PubMed), OVID, CINAHL (EBSCOhost), Scopus, and SAGE Premier, using the following search terms: “primary care,” “family practice,” “general practice”; in combination with: “practice-based,” “research,” “network,” “data,” and “infrastructure.” We identified publications that contained information on the establishment of PBRNs between January 1, 1965 and December 31, 2020 to establish a primary group of article abstracts.
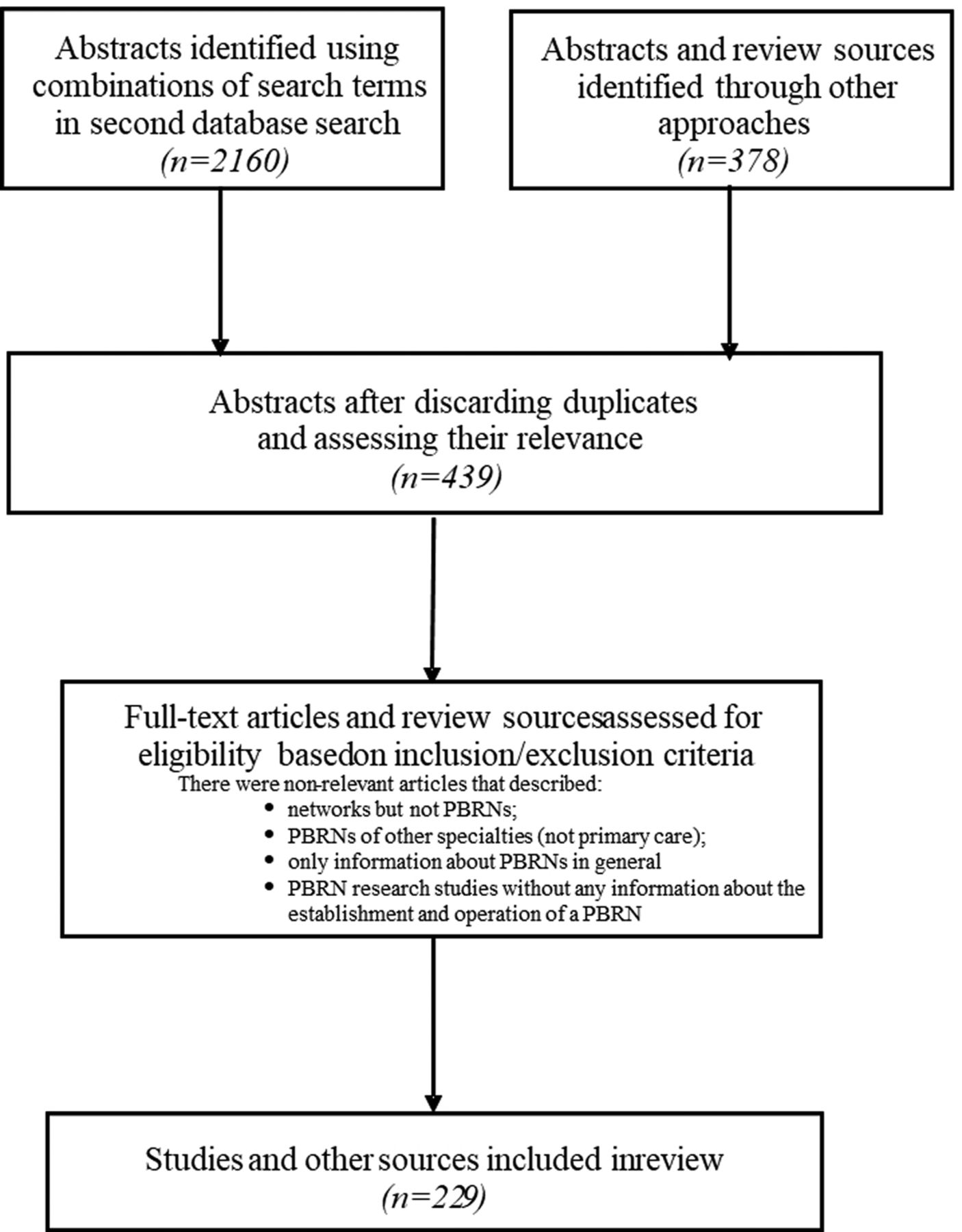
One of the authors (AD) reviewed the full-text articles and eliminated duplications and articles that were clearly irrelevant. Subsequently, 3 reviewers (AD, PM, and AH) scrutinized all articles separately to ensure that they were relevant to the research question and applied rigorous inclusion/exclusion criteria. The inclusion/exclusion criteria are presented in Table 1. The selection process yielded a total of 229 publications that included relevant information.
Inclusion and Exclusion Criteria for the Scoping Review
In the second step, we searched the “gray literature” for white papers, newsletters, conference abstracts, posters, proceedings, presentations, individual PBRN websites, editorials, and online materials published by national organizations; assessed the references in selected publications; and reviewed additional papers that emerged from bibliographic lists. An extended search was conducted using Google Scholar and public online sources. The lead author (AD) communicated with coauthors and colleagues to clarify ambiguities and bridge remaining gaps.
When there was any doubt about the relevance of a study, it was marked and remained in the list to be evaluated by another reviewer (ZN), who had in-depth understanding of PBRN research on an international scale and maintained professional relationships with many included PBRNs. This helped the authors put information published in the literature into a more granular context and gain a deeper understanding about its relevance and meaning. A more detailed description of the review process is presented in Figure 1.

Chart Flow Diagram. Abbreviation: PBRN, practice-based research network.
Charting, Collating, and Summarizing Findings
We explored the first 10 years of each PBRN's trajectory (when available) to capture all discoverable key actors and their attributes (interest, influence, goals), relationships and interactions between them, the nature of their relationships, and the resources contributed and properties of the PBRN that emerged during the establishment process. These key areas of our inquiry were anchored in social network theory.29,30 Four authors (AD, AH, ZN, JWMM) carefully reviewed selected publications, grouped those that referred to the same PBRNs, and implemented an iterative process to sort and characterize the material using a data charting form, including the following information: PBRN name, national affiliation, year of establishment, membership, information about PBRN leadership, geographical location and connection to other PBRNs, mission/purpose/goals/objectives/aims (when available), and narratives that informed us about the distinct groups of main actors (“nodes” of the network) and their contributions (“network resources”), their relationships and interactions (“ties” between the “nodes”), their relationship “features,” “properties” they developed, processes of establishment, and early operations. We considered “actors” to be individuals (eg, academics, clinician practitioners, practice facilitators) or groups (eg, PBRN members, boards of directors) who were interacting with each other.29⇓–31
An inductive thematic analysis approach32⇓–34 was implemented to identify key elements gleaned from the literature to generate themes and subthemes related to the establishment of PBRNs.
Our iterative content analysis yielded converging observations (analytic components). These basic components were grouped according to their relevance to already known specific activities or functions that were foundational to the establishment of PBRNs (eg, recruitment, membership, governance, communication, learning environment, and so forth). This process yielded the conceptualization of 57 key elements. These key elements were then linked to 12 subthemes based on higher-level similarities. The subthemes captured the distinct groups of main “actors” (or “nodes”) that contributed to the establishment of PBRNs.
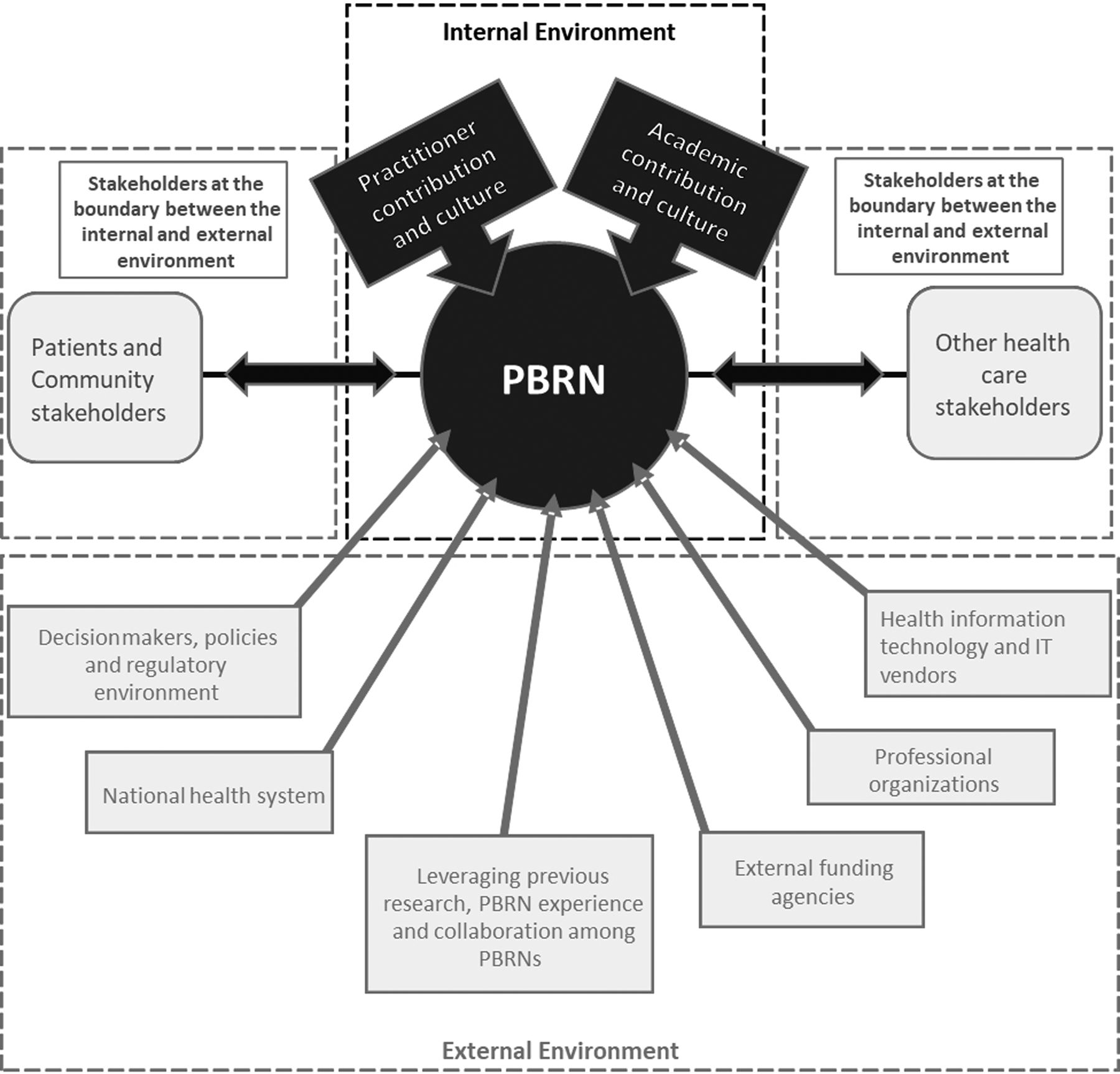
We then developed the final theme structure in relation to specific environmental domains where the subthemes most fittingly belonged. Our analysis defined 3 themes, including the external, the internal, and the boundary between external and internal environments. This article focuses on the theme of the “Internal Environment,” which consists of 25 key elements that can be grouped into 4 subthemes.
Some of the components from our review were then conceptualized as facilitators and barriers to establishing PBRNs, although not all components mapped to facilitators and barriers. In summary, our analytic pathway from data gathering to theme development can be described as follows:
Gathering original narratives from papers (relevant quotations)→Structuring and grouping narratives→ Developing components (eg, “Characteristics of a PBRN Leader”)→Grouping components→Developing key elements from groups of relevant components (eg, “Organizational Leadership”)→Grouping key elements→Developing subthemes from groups of relevant key elements (eg, “Network Infrastructure and Operations”)→Grouping subthemes→Coalescing themes (eg, “Internal Environment”)
Two examples of the methodological approach in synthesizing key elements, subthemes, and themes from the quotation level are presented in Appendix Tables 5 and 6. An illustration of the subthemes and their connections to the themes is presented in Figure 2.

The Thematic Structure of PBRN Establishment. Abbreviation: PBRN, practice-based research network.
Results
Our database search identified 2160 publications. A further search of references and the “gray literature” resulted in 378 additional publications. Of these sources, 229 met the inclusion/exclusion criteria. Information gleaned about PBRNs was often variable across publications and individual PBRNs. Included PBRNs and related literature are presented in Table 2.
Included Practice-Based Research Networks, Peer-Reviewed Articles, and Review Sources
Ninety-three PBRNs from 15 countries met the inclusion criteria from publications spanning a period of more than 50 years. We evaluated 37 PBRNs from the USA, 15 from the UK, 10 from Australia, 4 from Belgium (of which 2 were pilot projects), 6 from the Netherlands, 3 from Ireland, 2 from Switzerland, 2 from New Zealand, 2 from Canada, and 1 PBRN from Finland, Germany, Italy, Singapore, South Africa, and Sweden. ASPN and e-PCRN were binational and were established with contributors from the USA/Canada,35⇓–37 and USA/UK,23,38⇓–40 respectively and 4 were international networks.41⇓⇓⇓–45 PBRNs could be characterized as local, regional, statewide, interstate, national, or international.
The synthesis of our results yielded 3 main themes, 12 subthemes, and 57 key elements (see Table 3). In this article, we present 25 key elements that constructed the 4 subthemes that are linked to the theme of “Internal Environment.” An overarching thematic framework and thematic connections between its components are presented in Table 3.
Overarching Thematic Framework for the Establishment of Practice-Based Research Networks Focusing on the Theme of the Internal Environment Described in This Article
Foundation
We found 1 key element linked to the subtheme of “Foundation” that we analyze below (see also Table 3).
Most PBRNs articulated their core mission, goals, objectives, and aims at the time of their establishment. Sentinel surveillance and the study of population morbidity patterns were often in the focus in early networks.7,46⇓⇓–49 Real-world problems emerging in primary care settings, and improving clinical practice and health care through practice-based evidence were central to the interest of most PBRNs.9,35,36,50⇓⇓⇓⇓⇓⇓⇓⇓–59 These suggest that PBRNs have a widely shared focus and mission for evidence-based practice and quality improvement (QI) of healthcare services. In addition, numerous PBRNs aimed at the enhancement of practitioner knowledge.36,52⇓⇓–55,61,70,76⇓–78 This pattern has been consistent across academia-initiated and practitioner-driven activities by members who recognize the importance of practice-based research, which improves primary care practice. Furthermore, the UK and Australian networks explicitly stated the specific purpose of research capacity building in primary care.51,52,60⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–75 Later-generation PBRNs demonstrated more specific goals at their establishment, which defined their aims and partnerships.79⇓⇓⇓–83 We present PBRN goals and aims in Appendix Table 2.
As the PBRNs worked toward accomplishing their mission, they developed “ties” and “properties” that helped sustain their internal environment, but they also encountered a number of barriers and challenges, some of them were incidental, while some others were structural. These facilitators and barriers were mapped in relationship to specific key elements and are presented in the following and also summarized in Table 4.
List of Facilitators and Barriers
Practitioner Participation and Motivation
We found the following 5 key elements to be linked to the subtheme of “Practitioner Participation and Motivation” (see also Table 3). Most PBRNs were established on a core of research-motivated and experienced clinician members. Especially in the early networks, volunteer practitioner (“bottom-up”)7,84 support was instrumental.
The recruitment of members followed various paths. Some networks recruited a decisively selective group of practices, others tended to create either a representative or a convenience sample. Some sought specific practice or practitioner characteristics or PBRN-related criteria, especially in relation to research experience or interest in a specific research topic. In general, membership brought a set of benefits and obligations, which in some networks were more binding, while others applied a flexible membership model. The idea of providing value-added benefits to members was at the heart of most networks.
PBRN member recruitment often leveraged prior relationships with academia through training or research, relationships within professional organizations, connections established via social or professional venues, and various incentives.
Across the board, PBRN membership typically encompassed either general practitioners (GPs)/family physicians (FPs) or other primary care professionals, separately or together with GPs/FPs. Since the 1990s, numerous networks engaged multiple types of primary care disciplines, including allied health professionals and various levels of expertise.63,70,85,86 In the early years, mainly individual practices were involved, while later, membership was expanded to larger healthcare organizations.87⇓–89
Our analysis suggested 5 levels of member engagement on the research participation continuum: (1) practitioner-research leaders, who initiated, designed, and drove research; (2) champion members, who were active participants in all/most steps of research; (3) regular collaborators, who participated in research that was initiated, designed, and driven by others; (4) research advisors, who interacted with researchers and/or contributed data without conducting research; and (5) informed research users, who were interested in using research results without participating or contributing.
Common barriers for practitioner engagement and participation included lack of protected time, low interest in research topics, limited research skills, competing priorities, and maintaining practice efficiency.44,46,89⇓⇓⇓⇓–94 Obstacles to recruitment also included previous negative experiences with academic interactions.89,95
Practitioner focus on patient care excellence tended to form the cornerstone of PBRN activities. Practitioners were interested in research topics that were closely related to their daily work and were applicable to real-world conditions.9,18,36,60,69,79,80,92,96⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–108 As members, they aimed to contribute to new knowledge, implement research findings, and engage in healthcare policy or advocacy.
Member motivation was associated with the presence of a research culture in the clinic and the appreciation for research that members considered highly important in general practice.50,60,79,89,109 PBRN membership was perceived as professionally stimulating, increasing job satisfaction, supporting collegiality and peer learning, and facilitating professional development.
Networks that aligned their objectives with the needs of individual practitioners relied more on nonmaterial incentives, eg, a shared vision, participation in a learning community, dissemination of value-added resources, and diffusing knowledge. Such approaches created a solid foundation and strong incentive for PBRN research.39,66,67,69,78,81,82,86,99,105,108,110⇓⇓⇓⇓⇓⇓⇓–118.
Other nonmaterial incentives included simple projects at the start-up period, professional and practice benefits, and research assistance. Material incentives included training opportunities,61,63,65,66,69,73,78,86,111,119,120 small research grants,10,52,61,63,65,73,78,86,121⇓⇓⇓–125 and professional credits.46,78,80,125⇓⇓⇓⇓–130
Member financial support/remuneration has been applied broadly;60,61,65,73⇓–75,80,92,93,99,108,121,122,131⇓⇓⇓–135 however, in some cases professional credits proved to be enticing126 or preferable.46,73,80,102,125,127,129,130
Ongoing mentorship combined with practitioner empowerment built strong personal relationships, even when these were established through a “top-down approach,” and member compensation was limited.7,9,65,66,136
Academic Participation and Attitudes
Seven key elements were linked to the subtheme of “Academic Participation and Attitudes” (see Table 3).
The development of PBRNs was linked strongly to the development of academic centers of excellence in general practice/family medicine and coevolving with the primary care profession.6,7,47,56,70,137⇓⇓–140 Many networks were initiated and hosted by academic institutions, in part, by leveraging past professional relationships. A number of PBRNs also received infrastructure and technology support (financial and in kind) from academic organizations. In some countries, especially in the UK and Australia, most networks were developed based on national strategies and were supported by academic departments.51,63,65⇓–67,73,136,141⇓–143
A few networks included only academic professionals, while nonacademic practitioners had a minimal role, at least initially.129,140,144 However, some early networks expressed unease with strictly academically propagated PBRNs.54,145
Our study confirmed the notion that the history of PBRNs is inseparable from the development of family medicine/general practice as a distinct discipline. In countries where PBRNs were developed earlier (eg, UK and the Netherlands), these networks emerged together with the academic family medicine discipline.6,7 Based on our data, it seems that in those countries where the discipline was developed at a later stage, research that was able to inform the expansion of family medicine/general practice was also delayed.89,146 Likewise, in some countries where the discipline was not well supported until more recently, the development of PBRNs also seemed to have lagged significantly.76
Academic professionals recognized the importance of practice-based research for the discipline, professional growth, academic education, and careers and have often encouraged the work of PBRNs. They were also inspired and skillful leaders who contributed to the organization, expertise, research quality, reputation, and funding of networks. Academic expertise had a palpable influence on the prioritization of research as well.9,46⇓–48,57,60,66,75,86,90,91,119,122,125,136,137,140,144,147⇓–149
Academically supported PBRN databases allowed the management of a broader research portfolio and more focus on high-impact health conditions7,23,95,106,126,140,147,148,150⇓⇓–153 or facilitated increasing sophistication in primary care research, resulting in a definitive effect on practice improvement.7,21,93,109,126,129,140,147,149,152⇓–154
Academic educators frequently linked medical and resident training with PBRN activity, instilling research skills into future members. Through QI cycles and quality assurance in patient care, academics fostered an environment of excellence and facilitated knowledge transfer to learners, contributing to the growth of practitioners.50,52,93,109,112,130,137,154⇓–156
Academic departments benefited from working with PBRNs by increasing their publication output, strengthening professional training, acquiring grants, establishing fellowships, using or generating PBRN data for scholarly research, and making academic research more community focused and more relevant to primary care.6,47,57,108,124,137,140,157
Network Infrastructure and Operations
We found 12 key elements linked to the subtheme of “Infrastructure and Operations” presented in the following in groups, according to their relevance (see also Table 3).
Initial Partnerships to Establish PBRNs and Centers of Operations
In most PBRNs, academic institutions provided the backbone of network infrastructure, and they also became the center of operation. However, in some cases, professional organizations played this pivotal role.46,84,120,124,144,158⇓–160 Some PBRNs were affiliated with research institutes,47,76,158,161 some developed as community-based associations,81,107,110 in 1 case, without academic affiliation.111 Other PBRNs had more than 1 linkage,23,75,90,108,126 of which 1 was a HIT vendor.91 Some operated as affiliates of other PBRNs96,112,162 or developed as networks of PBRNs,21,60,75,108,126,163 or as subsets of networks,152 or incorporated previous PBRNs,164 or established multiple linkages combining the above affiliations.144 The maturity of PBRNs was clearly associated with more sophisticated research infrastructure development,21,39,60,75,133,153 including federated or “meta” networks (networks of networks).60,75,87,108,126,153,162,165 Information about various organizations that initiated and supported PBRNs is presented in Appendix Table 1.
Key Activities at Establishment, Infrastructural Funding
PBRNs were established through specific key activities that defined the nature of their network. Key activities at the establishment of PBRNs included those that initiated the formation of the network and transformed ideas and mission statements into activities. Some PBRNs followed a common pathway/approach to start their operations, eg, conducting a survey to establish the profile of their practices and practitioners or the routine collection of data in their practices. Representative key activities are illustrated with quotes from the literature in Appendix Table 3.
PBRNs received infrastructural funding from a variety of external sources; however, the most common infrastructural support came from hosting academic institutions.10,18,46,52,66,113,124,125,140 In some countries (eg, Australia and the UK), strategic infrastructural investments and enduring research capacity-building programs originated from national entities.6,52,63,66,69,73⇓–75,100 In some PBRNs, member dues and other in-kind contributions added to the infrastructure.35,52,84,124,130,166
Many networks recognized funding instability as a major challenge to sustainability. This compelled a number of PBRNs to develop business models to support their infrastructure longitudinally. We identified some business models that networks developed within the first decade following their establishment and during the time frame of our cross-sectional review. These models varied from contracting with external researchers who had long-term projects that ensured payments to practitioners or practices involved in these projects,78,124,167 to developing a diversified research portfolio60,115 or contributing with intellectual capital and infrastructure on a cost-recovery basis, to projects sponsored by major funding organizations.52,66 We also encountered more sophisticated business models that provided access to “big data” or other research data resources, which generated revenues for the network.153
Relationship Building between Academics and Practitioners in the Field
PBRNs based relationship building on the need to establish a shared identity among their members. Networks typically aimed at building long-term, constructive, collaborative, and reciprocal relationships and fostering collegiality, respect, trust, and mutual appreciation between academics and practitioners.
Synergistic relationships, which became pivotal for the long-term development of PBRNs, were implemented through all types of interactions between academic professionals and network members. Further, “conveners” that sustained the ties between them, such as practice facilitators, research coordinators, and assistants, were actively involved in these relationships. Thus, interpersonal multidirectional relationships were shown to be fundamentally important to the development of PBRNs. PBRN relationship-building activities are presented in Appendix Table 5, along with the steps of synthesizing this key element.
PBRNs reinforced relationships through training and education, applying multidisciplinary approaches and engaging key practitioners, practice managers, clinician champions,45,92,108 research assistants, and practice facilitators.168 Practice facilitation became a key component of many PBRN projects, supporting multidirectional communication between practices and network leadership and providing value-added assistance.
Dynamic practitioner–academic interactions fostered the emergence of a new model of primary care where research and QI are integral to the practice.9 This new model and vision of primary care, which has been developing since the early 2000s in some PBRNs,51,52,60,61,68⇓⇓⇓⇓⇓⇓–75 was expressed in a recent survey.89
Governance, Leadership, Communication
Strong leadership, multidirectional communication, and participatory governance that produces reciprocal benefits for all members were linked to PBRN growth already at the network establishment phase.43,60,90,92,124,125,153,157,167,169 The initial governance structure and multidirectional relationships leaders developed have influenced the network structure, how the network evolved in the following years, and the very first activities they engaged in.
Our data suggested that many networks were established around a recognized “research-enthusiast” and committed leader, with interest in improving primary care practice, developing new knowledge, and, in some cases, influencing policy. Leaders were either professionals73 who had senior academic positions169 and/or clinicians with long track records.67,124 Some also had previous PBRN experience with other networks.115,125 The components of key element “Organizational Leadership” are presented in Appendix Table 6 together with the steps of synthesizing this key element.
PBRNs used various pathways of a/synchronous communication to meet their goals for intellectual exchange, research capacity building, research prioritization, translation and dissemination of research results, and relationship building. On-site visits and personal communication were considered the most effective and motivating for research engagement. Conferences were used to generate new ideas and discuss their implementation.
Early PBRNs typically implemented an informal and low-cost governance model. We encountered a few networks with minimally structured governance, which were led by a director,84 while large single, international or federated networks and networks of PBRNs incorporated a more sophisticated and extensive leadership structure.41,43,44,60,75,92,96,108,126,132,153
Some networks operated as (semi)independent or nonprofit organizations, but there was limited information regarding their relationship to host organizations and how independently they operated.
Based on available data, PBRN governance models could be characterized as top-down, bottom-up, or a mixed model that engaged the entire organization, which some referred to as a “whole system approach.”66,86
Governing bodies of PBRNs tended to incorporate a mixture of member-practitioners, academics, or solely academic professionals, depending on their structure.
Typically, governance consisted of a leadership group with research expertise, which offered guidance to research proposals, and/or an oversight group, which contributed to planning and monitoring. In larger networks, subgroups/committees were established to attend to larger-scale issues. Administrative structures and day-to-day operations varied in size and complexity, depending on the robustness of the network.
Methodology of Prioritizing the Research Agenda and Topics of PBRN Research
We found that governance type was also linked to idea generation and research prioritization activities. Competing agenda was indicated by statements stressing that practitioner priorities were important.9,35,96,111,112,122,170⇓–172 In some publications, we also found information about leadership processes for cocreating the research agenda,81,83,86,99,110,125,132,173 data-driven research,21,90,153 evidence reviews,47,72,130 and the ranking of project ideas based on network priorities.35,99,110,115,132 Networks reported challenges when there were gaps between the interests of research funders and PBRN stakeholders, including divergence between the goals of granting agencies and interests of PBRNs.
We identified 5 levels of research outcomes based on the subjects of interest—patient-level, clinician-level, practice/health system-level, community/population-level, and PBRN-level—including work on the research capacity of the network. Many PBRN studies incorporated multiple levels of outcomes,52,60,84,94,116,130 which were closely linked to the types of data PBRNs collected.
Data Gathered from Networks, Data Management, and QI Activities
Some publications contained information about research data sources, data governance practices and ownership, data use and purpose, scope and representativeness, value (including capacity of data), and information about infrastructure for data management support, database development, warehousing, and interoperability. Ensuring data quality through ongoing improvement efforts was fundamental for PBRNs to operate as “real-world” research laboratories producing knowledge and resources that could be disseminated widely in primary care settings. Aggregation and systematic analyses of data emanating from large collaborations, eg, federated or “meta” networks, contributed to the generalizability of results and deeper research innovations.23,36,55,80,92,96,125,126,153
The issue of representativeness of the network was a concern in many PBRNs from the start. To prevent variations from national standards, some PBRNs developed confirmatory surveys to measure the external validity of their research,3,97,122,127,132,140,155,156,174⇓⇓⇓⇓⇓⇓–181 while some smaller/local networks were representative of the patient population of their area,152,156,182,183 or their data allowed extrapolation to a national population.129,137
QI was among the main objectives of many PBRNs, even before the year 2000.52,112 Our results indicate that QI has been a significant incentive for participation, and it was leveraged to improve clinical guideline implementation, stimulated the development of new methodologies,112,184 such as “best practices research,” played an important role in the translation of research into practice, helped identify research topics relevant to gaps in practice, and was also linked to collaborative learning.
PBRNs reported that QI activities enhanced the quality of healthcare in network practices.7,18,51,53,106,112 Numerous networks applied HIT to facilitate QI activities, such as quality feedbacks, clinical decision tools, and learning communities, and had a robust effect on QI implementations and QI capacity.21,74,95,103,105,133,185
Learning Environment
The learning environment was an integral part of the infrastructure and operation of PBRNs. Many findings indicate that colearning helped build a primary care research culture among PBRNs, especially through training/education7,52,55,63,66,69,70,73,75,78,79,81,109,111,179,186,187 or learning community activities.13,39,67,86,88,90,99,153,188
General training included educational courses, continuing medical education, annual training programs, higher degree education, and using interactive teaching methods, such as workshops, courses, and webinars. Mentoring, advising, research assistance, and QI training were frequently provided in the context of specific projects.7,38,43,46,51,52, 66,74,76,78,86,99,101,106,109,111,112,115,120,132,139,160,169,171,189
Training activities were targeted mainly to primary care practitioners interested in research, but they were also provided for emerging academic researchers. Residency and practitioner training programs linked to PBRN activities represented other components of the learning environment.
Research capacity building activities were pronounced among the priorities of UK and Australian networks and varied from simple research training courses to degree credits and higher-level education, allowing the more widespread use of clinical evidence gleaned from practice-based research.9,52,59,61,63,69,70,75,78,100 An example of research training is presented in Appendix Table 4.
More recent networks tended to emphasize the learning community aspect of PBRNs and considered it fundamental to the network's operation, but the seminal idea was rooted in early networks.54,111⇓–113 The function involved sharing resources and peer learning and the dissemination of best practices and QI methods based on facilitated member interaction.
Discussion
This article presents the findings of a seminal scoping review across the widest possible geographical and temporary scope, and it maps key elements contributing to the establishment of PBRNs in primary care settings. Our study examined a wide variety of publications spanning 5 decades. Our approach allowed us to explore key elements of establishing PBRNs, but it did not aim at a deep analysis of the underlying reasons.
Our synthesis yielded 57 key elements (see Table 3), of which 25 are discussed in this article. These belong to the subthemes of “Foundation,” “Practitioner Participation and Motivation,” “Academic Participation and Attitudes,” and “Network Infrastructure and Operations” and are linked to the theme of “Internal Environment of PBRN.” Our lists of facilitators and barriers were distilled from knowledge we derived from our synthesis, and they may be useful for those who plan to build PBRNs in the future.
The key elements presented in this review are in line with a study published in 2005 on infrastructural requirements of PBRNs in the American context.190 They are also coherent with network dimensions that create social and intellectual capital that were presented in an evaluation tool/kit by Harvey et al in 2000,191 although this article applies a different nomenclature. Harvey's study also underscores the existence of common features among PBRNs across all geographies.
In the subtheme “Foundation,” we linked mission, purpose, goals, objectives, and aims; however, not all PBRNs communicated their vision and goals clearly in discoverable publications, which does not imply a lack of goals. In this review, we did not investigate whether networks modified their mission during their trajectory or if they became incorporated into larger networks, but their continuity suggests that they may have reached at least some of their initial goals.
Our review suggests that network member profiling surveys,44,89,98,122,140,155,156,169 gauging practitioner motivation51,55,56,78,79,102,127,138,145 or training needs,63,67,69,70,100 and assessing the external validity of research97,179⇓–181 were common in the early phase of networks, underscoring the importance of membership and/or population characteristics, practitioner motivation, and the research capacity of the network.
We found a shift in later-generation PBRNs toward more specific goals articulated at their establishment, which expressed their partnership interests.79⇓⇓⇓–83 These trends indicate an increasing sophistication of PBRNs, either through broadening their membership, which reflects their transformation in the primary healthcare environment, or through research specialization.13,85,192 The evolution of the goals of new networks over time may indicate that PBRNs adjusted to the emerging needs of communities for better primary healthcare practice.
Specific network objectives and pathways of starting networks were dependent on available resources that fostered PBRN activity in each country and network. Most of these resources were influenced by external factors, which in turn could alter resources that are internal to the PBRNs. These connections will be reviewed in a subsequent article.
The development of large networks often incorporated an objective to ensure the viability of emerging PBRN partners.21,75,96,108,126 These networks had access to a variety of populations, leveraged wider interests, engaged in multiple types of research, and focused on research topics that were broadly generalizable. This trend seems to have developed around 2010, and it is consistent with the findings of other studies that show that there is a tendency toward multinetwork collaborations, especially when they leverage advanced HIT.13,133 As a further expansion of PBRNs, the establishment of PBRN “meta-networks” led to a transformation into “communities of solutions”193 supported by Centers for Primary Care Practice-Based Research and Learning (P30 Centers), in the USA,194 and the extension of the clinical research network approach to all healthcare, in the UK.195
In these transformations, the focus of the research partnership was gradually extended from individual practitioner to practice, then clinic, and finally to the broader PBRN membership even in the early phases of PBRN development. These seem to parallel a similar methodological evolution, which progressed from studies addressing existing knowledge gaps of primary care to more sophisticated comparative effectiveness research based on large primary care data sets. This transition was anchored in increased research capacity and technological innovations that enabled additional functions, such as accredited evaluations,126,153 advanced clinical decision support,93,95,96,153 and learning communities.88,90,153 In many PBRNs, practitioners seemed to be more poised to improve the quality of care than to do academic research. These findings are in line with a recent survey.196
Importance of Communication, Learning Environment, and Relationship Building
Our analyses, which were anchored in social network theory,29,197 indicated the highest levels of associations in the following areas: (1) communication; (2) learning environment; and (3) relationship building between academics and practitioners in the field. These key elements included numerous components describing facilitators as well. The first and second areas indicate that PBRNs evolved as learning organizations applying multidimensional communication, which enabled them to shorten the time of spreading innovations among stakeholders, underscoring that research is not the only activity in the scope of PBRNs.198,199 The third area in the internal environment of PBRNs was linked to key elements for relationship building between academics and practitioners in the field and reflects features of these relationships that propagated the establishment of PBRNs.
Our findings are also convergent with previous studies that present key elements of high-quality practice organizations in primary care.200,201 This may indicate that practices engaged in PBRN activity are endowed with properties that enable them to improve care quality or that QI is organically linked to PBRN activity. The richness of data related to communication, learning environment, and relationship building in PBRNs, using multidirectional and multiple means communication, suggests more intense interactions and knowledge exchange among PBRN members.
The Impact of PBRNs on Primary Care Practice and Professionals
Our findings demonstrate a reciprocal relationship between the development of PBRNs and the generation of new knowledge for primary healthcare improvement, the enhancement of the discipline of primary care, and the acceleration of primary care practice reform through transformative collaborations. Although our review suggests that practices that participate in PBRN research may be somewhat different, and therefore may not be representative of primary care in general,41,97,122,148,174,181,202 in some networks, participation seemed to enable the implementation of care innovations. Through their broader impact on healthcare, policy, and education, members may have also accelerated innovation transfer to other practices.203⇓⇓⇓–207
Based on our findings, we formulated 5 levels of member engagement on the research participation continuum (see Table 3), including literature-concordant “research leaders,” “network champions,” “regular collaborators,” “advisors,” and “informed research-product users.” The latter describes practitioners who are influenced by PBRN activity passively (“listeners”).69,100,208,209 This may be noteworthy, since academic funders typically do not support the dissemination and “consumption,” only the “production,” of knowledge and resources.
Our findings indicate that the 50-year development of PBRNs gave rise to a new thinking and way of practicing general medicine, which gradually integrated research into community practice. This notion might be called “researcher-in-community,” which describes practitioners who pose questions emerging from daily practice to a dedicated network of like-minded colleagues, supported by academic researchers. Their aim is to answer practical questions through practice-based research by bringing the university to community practice and incorporating the community into academia.
This is analogous to the model of “researcher-in-residence,”210⇓–212 an arrangement that may provide additional benefits through broader cross-pollination, learning, and diffusion of healthcare innovations.19,203,213
Governance Models
Our analyses indicated “top-down,” “bottom-up” or mixed (“whole system”) governance models in PBRNs.66,142 We found other typologies for PBRN governance in a study from the UK214 and in a publication from Institute for Health Policy Studies (IHPS), in the UK.215 There was limited information on governance models PBRNs adopted over the period of their establishment. Some articles suggest that a mixed-type model tended to develop in most networks over time. For example, the Nijmegen Family Practice Academic Network started as a top-down network, but practitioner empowerment resulted in stronger bottom-up governance.9,10
Reciprocal Benefits between PBRN Practices and Academic Departments
The key elements “Learning Environment” and “Academic Contribution to PBRNs” reflected strong support academicians provided to facilitate the professional growth of primary care practitioners.
Our synthesis established 6 key elements that describe the contributions of academia and 1 element that points to benefits that academic institutions received from PBRNs (see Table 3). It is important to note that this is not a quantitative measure of academic benefits, which included publications, enhanced graduate education, grants supported by PBRN data, excellence in teaching medical students and training residents, and better proximity to community, which were facilitated by working with PBRNs. This reflects the reciprocity between academician and practitioner benefits from PBRN participation.
Business Models of Supporting the Work of PBRNs
Financial instability was another significant challenge for PBRNs. Prior research has underscored the importance of infrastructural and research funding for PBRN operation.11,190,216⇓–218 To address ongoing infrastructural support, some networks developed a business model at the time of their establishment52,66,82,124,153 or later.172 The PBRN infrastructure has been promoted in the USA through training and technical assistance provided by the Agency for Healthcare Research and Quality,219 while in the UK, a diverse research portfolio elicited by the needs of academia and industry has been driving research in primary care settings.75
Geographical Variations in PBRN Development in the Internal Environment
We have not seen substantial geographical variations in the “Internal Environment” of PBRNs (the focus of this article) by region or country. However, we observed a clear and strong thrust toward research capacity building in primary care settings among the UK and Australian networks. These networks tended to attribute similar importance to practice-based evidence and evidence-based practice in family medicine/general practice and primary care, compared with networks from other countries. Dutch networks were characterized by the development of registries of data recorded by FPs. Data collection capacity and modalities defined the use of study methodologies in different countries. Examples include sentinel surveillance networks and relevant studies in the UK, Australia, Belgium, the Netherlands, or the Dutch registries and their observational studies, and card studies plus flow charts in American networks.
International networks shared similar infrastructural problems with large national networks in the USA and UK, including study coordination, network logistics, challenges with the management of large data sets, and the costs of big-scale activity. In addition, international networks encountered other problems that emerged from differences between the local and/or national environment (eg, different ethical and regulatory frameworks across different countries); interpretation bias (eg, local differences in understanding of key research concepts); and challenges from different structures of member networks depending on varying levels of development and organization.
In the UK, Dutch, Canadian, and Australian networks, we observed more top-down PBRN governance, although it was not always communicated explicitly. In the American networks, there was more emphasis on practitioner engagement and empowerment (participatory networks). Various governance types defined pathways of practitioner empowerment as well. In this way, top-down networks more commonly implemented audit cycles, educational and degree courses, and academic appointments, whereas more bottom-up type networks more frequently promoted shared resources and learning communities. However, top-down networks also developed learning communities, eg, through the audit cycle sessions of the Dutch networks, and, vice versa, bottom-up networks in the USA promoted the professional development of their members through degree programs.
Financial incentives showed similar patterns. In the UK and Australia, providing PBRN member financial incentives was more common practice, but this type of incentive expanded over time, together with professional credits. Typically, the use of financial incentives seemed more common where top-down governance was prevalent, while the importance of intellectual exchange and development of new knowledge was a superior motivator in bottom-up networks. The use of financial incentives expanded in the last category of networks over time, underscoring the value of the time and effort of practitioners and also indicating a movement from single-practitioner practices, where the practitioner's membership was based on personal motivation, to larger organizations where financial motivators may play a greater role.
Suggestions for Developing New PBRNs
Our review indicated a clear emphasis on specific activities and practices that led to the development of new PBRNs. We summarize these in Table 5.
Suggestions for Developing New PBRNs
Limitations
According to our knowledge, this is a seminal and novel scoping review and a mapping of what can be gleaned from the international literature about the establishment of PBRNs in primary care across multiple countries and over a period of more than 50 years. Our ongoing work may be a foundation for future studies on the development of PBRNs; however, this article was limited to the key elements of the main theme “Internal Environment.” Future studies will explore other domains, including the external environment and those spanning the internal and external environments.
We relied only on English-language sources since our team did not have the capacity to review scientific papers in several languages. However, most of the PBRN literature is in English, which favors our approach.
Our decision to review up to 10 years of each network's development can be challenged, since some networks may not need 10 years to develop a mature operation. However, we observed that some pioneer networks developed more gradually without well-tried templates, so we wanted to ensure that we can capture this important process.
The list of PBRNs that met our inclusion criteria is more limited than those identified in the USA,220 Australia,221 the UK,70 and Canada222 and in sources that refer only to specific PBRN activities. We excluded articles that did not contain sufficient information on PBRN establishment. We also omitted data that we found exclusively on PBRN websites without any supporting literature. In some cases, our search of the “gray literature” was extended by communicating with key informants or authors. This approach may result in the omission of some less accessible information.
Scoping reviews may carry some bias of various kinds because a critical appraisal of the included literature's quality is often beyond their scope. Selection bias may occur, if not all available data on a topic are identified or included. In this study, we implemented an inductive thematic analysis methodology. Themes, subthemes, and key elements emerged from the data. However, we purposefully leveraged some well-established a priori knowledge about PBRNs that had a guiding effect on the development of our thematic model.
Conclusions
PBRNs have emerged through reciprocal relationships and interactions between academicians and primary care professionals. They evolved not only as research communities but also as learning organizations with multidirectional communication that shares the new knowledge and best practice innovations across the membership. They had a marked impact on the landscape of primary healthcare of the academic disciplines and became an integral part of primary healthcare practice in their countries. Although there are country- and PBRN-specific features, most facilitators and barriers of developing PBRNs, as viewed from their internal environment, are shared throughout the world and over 5 decades.
Appendix
Types of Organizations That Initiated and Supported PBRNs at Their Establishment and Relevant Quotations
Identical PBRN Missions, Purposes, Goals/Focuses, Objectives, Aims, and Relevant Quotations
Key Activities at Establishment and Relevant Quotations
Example of Practice-Based Research Network Research Training
Example of Synthesis of Key Element “Relationship Building between Academics and Practitioners in the Field”
Example of Synthesis of Key Element “Organizational Leadership”
Notes
This article was externally peer reviewed.
Funding: None.
Conflicts of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/4/762.full.
- Received for publication November 16, 2020.
- Revision received February 9, 2021.
- Accepted for publication February 10, 2021.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.↵
- 203.↵
- 204.↵
- 205.↵
- 206.↵
- 207.↵
- 208.↵
- 209.↵
- 210.↵
- 211.↵
- 212.↵
- 213.↵
- 214.↵
- 215.↵
- 216.↵
- 217.↵
- 218.↵
- 219.↵
- 220.↵
- 221.↵
- 222.↵
- 223.
- 224.
- 225.
- 226.
- 227.
- 228.
- 229.
- 230.
- 231.
- 232.
- 233.
- 234.
- 235.
- 236.
- 237.
- 238.
- 239.
- 240.
- 241.
- 242.
- 243.
- 244.
- 245.
- 246.
- 247.
- 248.
- 249.
- 250.
- 251.
- 252.
- 253.
- 254.
- 255.
- 256.
- 257.
- 258.
- 259.
- 260.
- 261.
- 262.
- 263.
- 264.
- 265.
- 266.
- 267.
- 268.
- 269.
- 270.
- 271.
- 272.
- 273.
- 274.
- 275.
- 276.
- 277.
- 278.
- 279.
- 280.
- 281.
- 282.
- 283.
- 284.
- 285.
- 286.
- 287.
- 288.
- 289.
- 290.
- 291.
- 292.
- 293.
- 294.
- 295.
- 296.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Looking Back to Move Forward: Reflections of PBRN Directors
- A Review of 50 Years of International Literature on the External Environment of Building Practice-Based Research Networks (PBRNs)
- Building a practice-based research network for healthcare integration: a protocol paper for a mixed-method project
- Family Medicine Research on Health Equity, Addiction, and Eating Breakfast--Just for Starters