
Abstract
Background: This article is the second part of a novel scoping review of the international literature that presents those key elements that underpin the foundational activities of Practice-Based Research Networks (PBRNs). In this article, we examine the external environment and the intersection between the internal and external environment domains.
Methods: We searched electronic databases, including MEDLINE (PubMed), OVID, CINAHL (EBSCOhost), Scopus, and SAGE for publications in English between 1/1/1965 and 9/15/2021. We also searched reference lists of selected publications, gray literature and other online sources. Inductive thematic analysis was applied to construct the main themes, subthemes, and key elements from a scoping review covering up to 10 years of reported experiences of each of the 98 PBRNs that met the inclusion criteria.
Results: In this study we present 2 main themes: “Stakeholders at the Intersection Between the Internal and External Environment” and the “External Environment.” The first is linked to the subthemes “Patient and Community Stakeholders” and “Other Healthcare Stakeholders” and 11 key elements. The second relates to the subthemes “National Health System,” “Institutional/Governmental Support, National/State Policy and Regulatory Environment” “Professional Organizations,” “Leveraging Previous Research and PBRN Experience and Interacting with Other Networks” and “Health Information Technology (HIT) and HIT Vendors” and 21 key elements.
Conclusions: Despite variations in geography, time, and healthcare context, PBRNs shared many similar developmental experiences over the past 5 decades. Their external environment contributed significantly to their developmental trajectories during the first 10 years of their operation.
Introduction
Practice-Based Research Networks (PBRNs) are collaborations of academics and practitioners in the field working together as research laboratories for primary care, to generate and implement practice-based evidence and quality improvement in primary healthcare.1⇓⇓⇓–5
PBRNs initiated their activity over 5 decades ago in several pioneering countries. In Birmingham, UK, a group of general practitioners started collecting morbidity data systematically in their practices and developed the first primary care research collaboration in 1967.6 In the Netherlands, Huygen engaged 4 Dutch family practices in the Nijmegen area in1967.7 In the USA, the Family Medicine Information System in Colorado (FMIS) and the Cooperative Information Project (COOP) were developed in the 1970s to investigate problems encountered in primary care.8⇓⇓–11 Since these early initiatives, research-driven community family physicians, academics, and researchers, increasingly committed themselves to working collaboratively to improve and transform primary healthcare.2,12,13
Although there is information about the development of PBRNs around the world and in specific countries, it remains unclear what characteristics they may share with regards to their developmental trajectory and what may be unique to each PBRN's own history of development. We addressed this gap in the literature by conducting a scoping review of publications and sources from as many countries as possible. We reviewed English-language publications to elucidate the broadest information about the factors that enhance or impede PBRN development. In a previous article14, we presented facilitators and barriers of the internal environment related to the creation of PBRNs. In contrast, this article explores the 2 distinct domains of the external environment that include the “Stakeholders at the Intersection between the Internal and External Environment” and the “External Environment” in terms of facilitators and barriers in building PBRNs.
Methods
We completed a scoping review of the literature following a methodological framework described by Arksey and O'Malley.15 This type of review was considered appropriate to map key elements from a broad variety of data sources and various types of evidence about building PBRNs across the world.
We followed specific analytic steps suggested by the method: (1) defining the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, (5) collating and summarizing the findings, and (6) reporting the results. The methodology was identical to what we used in a previous publication.14
Identifying Relevant Studies and Study Selection
We identified relevant publications in a 2-step process. In the first step, we searched the English literature systematically and reviewed articles published between 1/1/1965 and 9/15/2021 in the following databases: MEDLINE (PubMed), OVID, CINAHL (EBSCOhost), Scopus, and SAGE Premier, using the following search terms: “primary care,” “family practice,” “general practice”; in combination with: “practice-based,” “research,” “network,” “data,” and “infrastructure.” In the second step, we searched the “gray literature” for white papers, newsletters, conference abstracts, posters, proceedings, presentations, individual PBRN web sites, editorials, and online materials published by national organizations. We also assessed the references of selected articles and bibliographic lists. Google Scholar and public online sources were searched as well. Additional communications with authors and colleagues helped clarify knowledge gaps.
Three reviewers (AD, PM, and AH) scrutinized all articles separately and applied rigorous inclusion/exclusion criteria.14 (Appendix Table 1) The lead author (AD) communicated with authors and colleagues to clarify ambiguities and another reviewer (ZN) evaluated uncertainties about specific studies. The details of the review process are presented in Figure 1.

Chart flow diagram of the process of systematic selection of articles. Abbreviation: PBRNs, Practice Based Research Networks.
Charting the Data, Collating, and Summarizing the Findings
We examined the development of PBRNs in a period of over 50 years and we focused our study on the first 10 years from the inception of each individual PBRN. We gleaned information about each network during their first 10-year period using specific sources listed above. Some PBRNs had only 1 relevant publication, while others had multiple data sources that they produced. The data we collected were limited to those available in our selected sources. We reviewed identified sources to discover key actors, attributes, relationships between them and the nature of these relationships, resources contributed, and properties produced, using social network theory-concordant key concepts.16⇓–18 Thus, we considered each network to develop relationships and interactions (“ties”) with actors from the external environment (“nodes”), and we looked at the “features” of their relationships and interactions with the PBRNs, and the outcomes (“properties”) that were derived from these relationships and interactions.
We applied an inductive thematic analysis approach19⇓–21 using an iterative process that allowed us to group the narrative observations into components. We clustered the components into key elements according to their relevance to specific domains of building PBRNs. Then we linked the key elements to subthemes that corresponded with groups of actors that influenced the establishment of PBRNs, considering their high-level similarities. Finally, we connected the subthemes with the main themes, which were developed to reflect the environmental domains where the subthemes clearly belonged.
Our synthesis resulted in the conceptualization of 3 main themes, 12 subthemes and 57 key elements. Many components captured information about the facilitators and barriers for building PBRNs, although not all components delineated facilitators and barriers. This article focuses on the 2 main themes “Stakeholders at the Intersection between the Internal and External Environment” and “External Environment,” and the 8 subthemes and 32 key elements that are linked to them.
In summary, our analytic pathway from data gathering to theme development can be described as follows:
Gathering original narratives from articles (relevant quotations) > Structuring and grouping narratives > Developing components (eg, “Commitment and motivation to improve health in community”) > Grouping components > Developing key elements from groups of relevant components (eg, “Motivation of Community Members for Research Participation”) > Grouping key elements > Developing subthemes from groups of relevant key elements (eg, “Patients and Community Stakeholders”) > Grouping subthemes > Coalescing themes (eg, “Stakeholders at the Intersection between the Internal and External Environment”).
An example of the methodological approach to synthesizing components, key elements, subthemes, and main themes is presented in Figure 2.

An example of the methodological approach in synthesizing components, key elements, subthemes, and themes from the quotations.
Results
Our original database search identified 253814 publications and the updated literature search yielded 53 publications. The inclusion/exclusion criteria were identical to the previous publication14 and applied on now 2591 publications, of which, 31 new sources met our inclusion/exclusion criteria. Of these 31 sources, 19 came from the same PBRNs reported in the previous study14 and 12 led us to the identification of 5 new PBRNs. This resulted in 260 articles for this study.
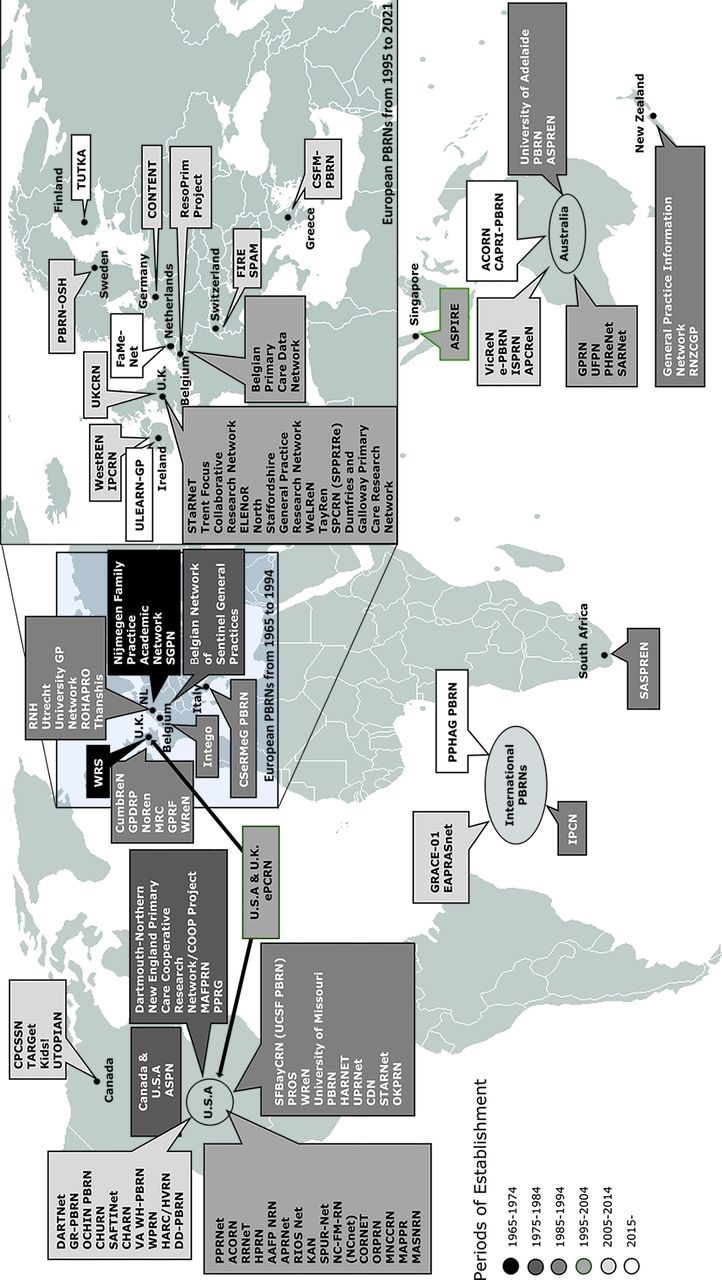
Our review yielded 98 PBRNs, 2 of which were binational, 4 multinational, 37 from the USA, 15 from the UK, 12 from Australia, 4 from Belgium, 7 from the Netherlands, 3 from Ireland, 2 from Switzerland, 2 from New Zealand, 3 from Canada, and 1 PBRN from Finland, Germany, Greece, Italy, Singapore, South Africa, and Sweden, respectively (Figure 3).
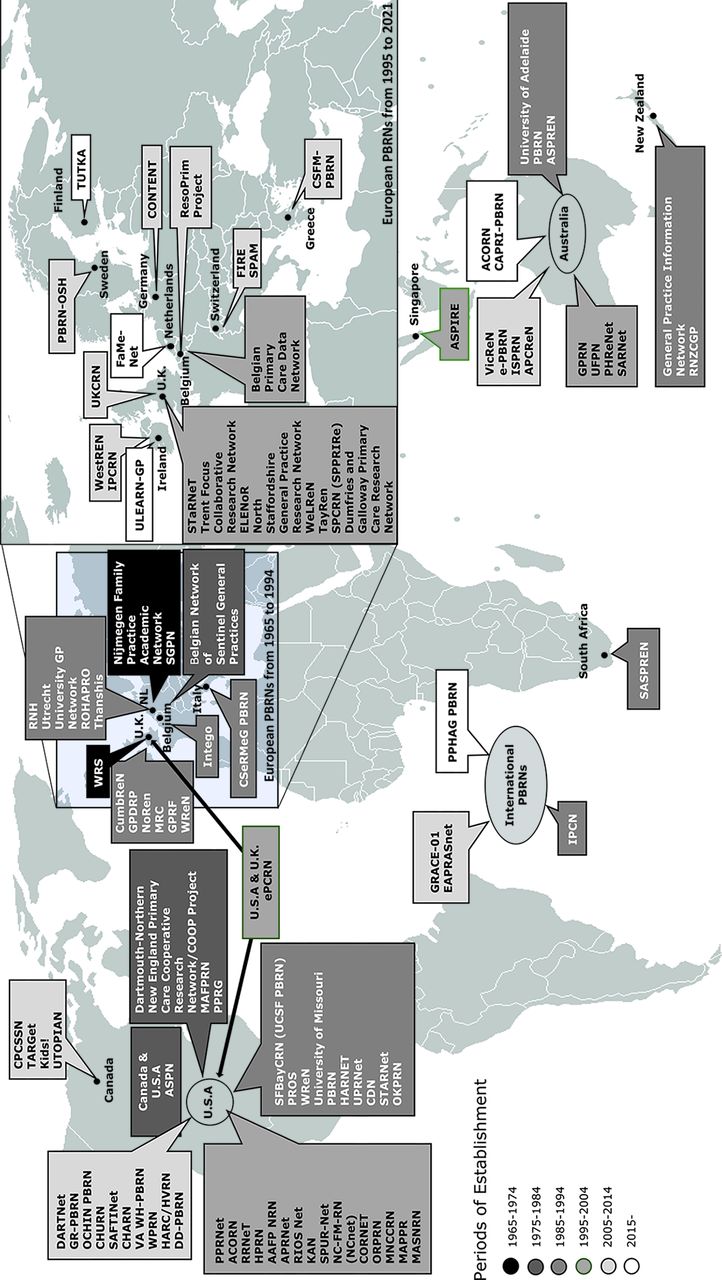
The world map of Practice-Based Research Networks (PBRNs).
The synthesis of our results yielded 3 main themes, 12 subthemes, and 57 key elements. The overarching thematic framework and thematic connections between its components are presented in a previous publication,14 while in Appendix Table 2 we show the key elements related to the internal environment (not included in this study; see shaded cells).
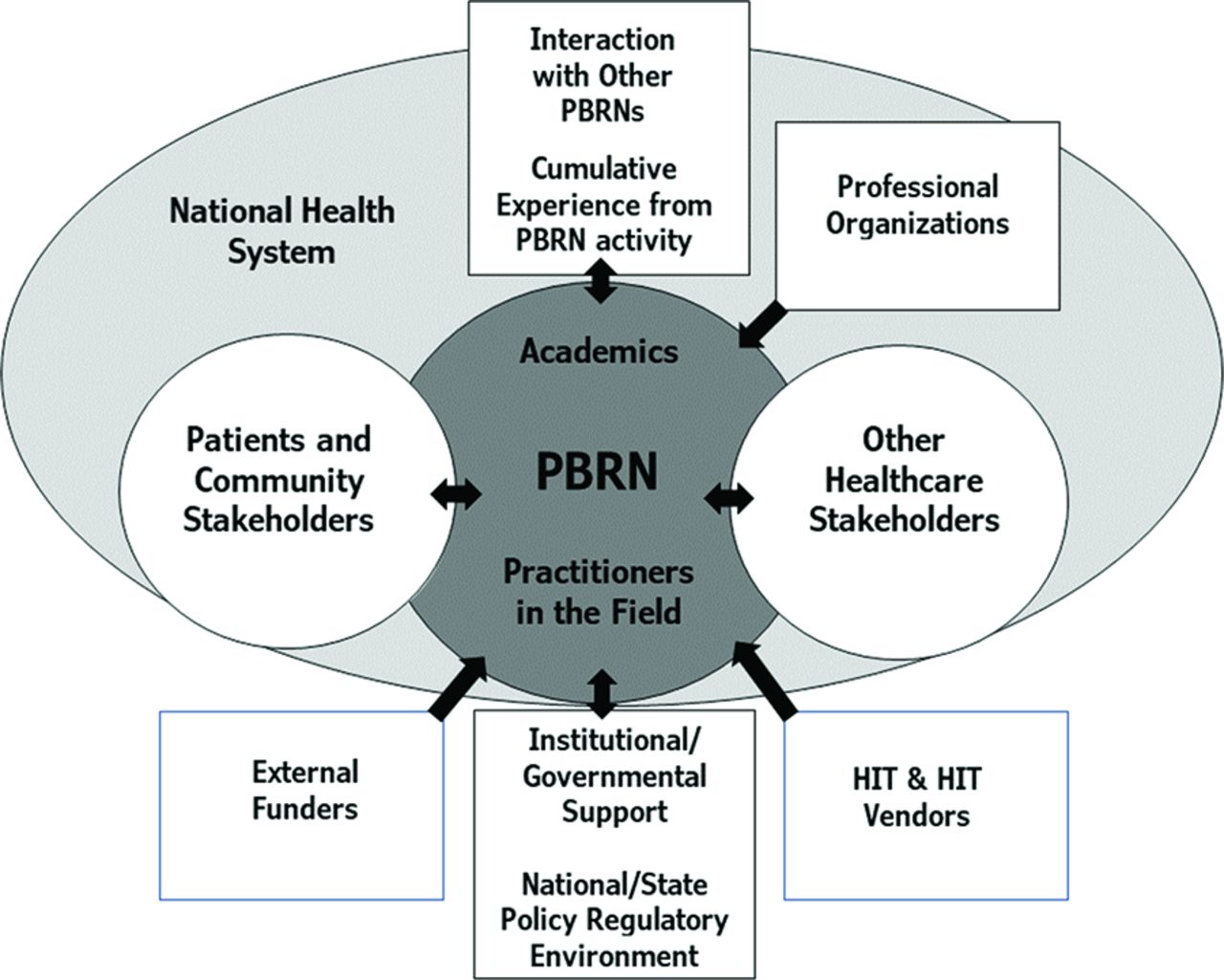
In this study, we identified 2 main themes that represented 2 groups of stakeholders. The main theme “Stakeholders at the Intersection between the Internal and External Environment” reflects the group of “boundary spanners” between the internal and external environments. These stakeholders spanned both the external and internal environments in the networks we explored, which were created at various times during a period of over 50 years, and so we categorized these in a separate main theme. The other main theme “External Environment” includes stakeholders that, although located in the external environment,22 influenced the development of PBRNs. (Figure 4)
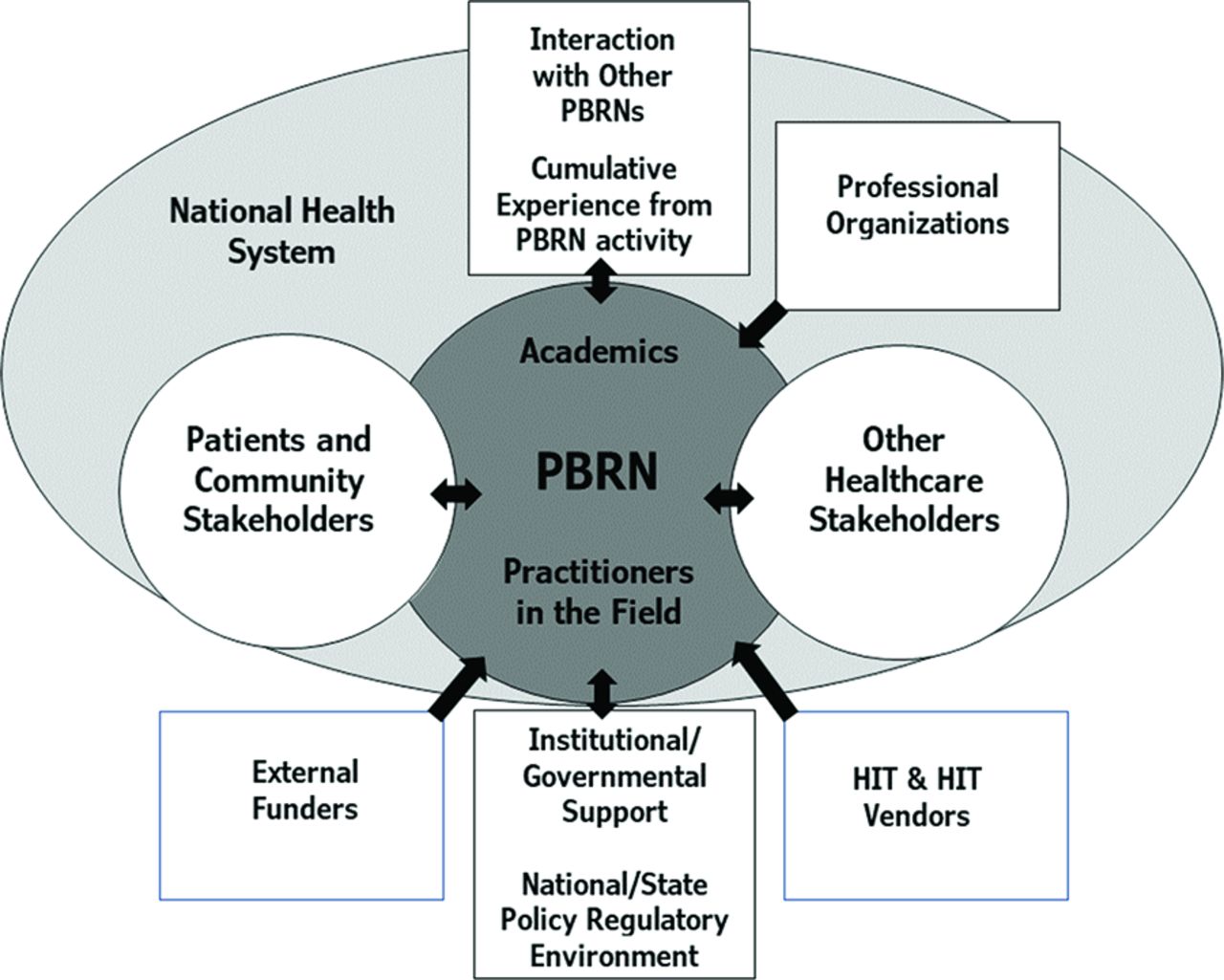
Stakeholders influencing the development of Practice-Based Research Networks (PBRNs). Abbreviation: HIT, Health Information Technology.
Main Theme: Stakeholders at the Intersection of the Internal and External Environment
We identified 2 subthemes and 11 key elements linked with the main theme “Stakeholders at the Intersection of the Internal and External Environment.” The overarching thematic structure of this theme (subthemes, key elements, and components) are presented in Table 1. The included components are facilitators and barriers for building PBRNs.
Subthemes, Key Elements and Components Linked to the Main Theme “Stakeholders at the Intersection Between the Internal and External Environment”
Subtheme: Patients and Community Stakeholders
Our review identified an increased focus on rural,9,22⇓⇓–25 nonmetropolitan,26⇓–28 or disadvantaged communities29,30 across American PBRNs that emerged before the 2000s. A considerable number of PBRNs aimed to address health disparities among underserved, minority, or vulnerable populations in the community they served,30⇓⇓⇓⇓⇓⇓⇓⇓⇓–40,41,66 or participated in consortium of PBRNs with similar missions.42 Australian PBRNs expressed interest in rural populations through the membership of local practitioners.42⇓⇓⇓–46,157 We also identified several UK PBRNs that focused on rural populations.47⇓–49
A few of the early networks linked patient care excellence to patient-centeredness and community engagement,29,50,51 This spread across the majority of networks over time and highlighted the importance of patient-engagement to improve patient outcomes and satisfaction.33,40,51⇓⇓⇓⇓⇓⇓–58 Fundamental components of the key elements “relationships with patients and community groups” included trusting and long-standing partnerships to promote equity and address health disparities.25,31,34⇓⇓⇓⇓–39,48,53,57⇓⇓⇓⇓⇓⇓⇓⇓⇓–67
Networks with more “bottom-up” governance17,68,69 implemented Community-based Participatory Research (CBPR) methodologies at least in some of the steps of their research, to increase the impact of research on their community,25,29,31,32,40,54,59,62,70 The work of Community Advisory Boards (CABs) was essential to CBPR research.55,62,66,67,70,71,73 On the other hand, several networks with a more “top-down” (hierarchical) approach17,68,69 also established collaborative relationships, shared decision-making and research dissemination activities with patients, and incentivized patient participation in research to generate benefit for broader populations.58,63,74⇓–76
Subtheme: Other Healthcare Stakeholders
Various healthcare stakeholders such as academic institutions, health systems, public health entities, industry, insurers, health organizations, and policy advocates were involved in the activities of PBRNs.10,38,39,46,51⇓⇓–54,60,61,63,66,69,77⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–90 The majority of UK PBRNs started in the 1990s reported engagement of health authorities and community trusts in their partnerships,48,69,78,79,92 while they also integrated social care research into their activities.48,49,60,78,93,94
In the past 2 decades, more emphasis was placed on the engagement of stakeholders from different levels of healthcare (national, state, and local) and educational institutions.37,38,52,66,68,69,71,72,77⇓⇓–80,84,88,89,94⇓–96,237,250 Shared mission between a PBRN and other healthcare stakeholders for the improvement of healthcare engendered relationships for R&D and learning in a wide array of projects.34,36,39,47,48,53,62,69,79,89,93,98⇓⇓⇓⇓⇓⇓⇓⇓–107 Further, a considerable number of more recently created PBRNs established such partnerships from their inception.39,54,55,63,72,80,88,89,97,108,109
Main Theme: External Environment
We identified 6 subthemes and 21 key elements linked with the main theme “External Environment.” The overarching thematic structure of this theme (subthemes, key elements and components) are presented in Table 2. These components are facilitators and barriers for building PBRNs. In addition, a condensed presentation of the subthemes is presented below.
Subthemes, Key Elements and Components Linked to the Main Theme “External Environment”
Subtheme: National Healthcare System
Many publications indicate that PBRNs were anchored in the broader healthcare system in their country.7,32,35,45,58,63,67,78,81,86,89,106,116,120,121,135 A strong position of general practice/family medicine in the healthcare system positively influenced PBRN development, whereas networks reported more barriers to their development in countries with less primary care support or no requirement for patients to have a primary care/family doctor as their coordinator of health services.45,52,63⇓–65,81,115⇓⇓⇓⇓⇓⇓–122
In some countries, where PBRN activity was appreciated, networks were incorporated into the broader healthcare system.63,117,121,151 to function as research laboratories of primary care,63,86,102 or as organizations that conducted research that focused on the priorities of the healthcare system.63,86,123 In some other countries PBRNs built on their linkages to the broader healthcare system with objectives for optimizing the quality and efficiency of healthcare28,33,39,44,50,51,62,64,67,80,81,84⇓–86,105,111,113,120,122⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–133 and for timely knowledge translation and dissemination.25,53,55,67,70,80,85,89,95,97,114,128,129,135⇓⇓⇓–139
Subtheme: Institutional/Governmental Support, National/State Policy, and Regulatory Environment
Many PBRNs provided an interface for collaborative effort with governmental bodies and institutions.9,38,52,89,92,97,109,136,149⇓⇓–152 They disseminated their results to the government and health authorities, influenced health policies and recommendations and advocated for R&D programs and practice-based and/or community-based evidence.29,38,40,52,57,58,70,80,81,89,92,106,109,114,120,130,149,152,153 In some countries, their recognition secured more systematic and substantial funding, via national-level initiatives.22,86,104,114,125,154,157
In other cases, PBRNs were influenced by national initiatives and policies that either supported networks at their inception45,47⇓–49,52,63,68,69,72,75,79,102,104,109,120,155⇓–157,161,165,184,250 or later,32,36,52,75,138,158⇓⇓⇓–162 or they were linked to their transformation,63,85,123,163,164 or to the dissolution of some PBRNs.165,166 The regulatory environment in different countries facilitated commitment to long-term funding to help improve evidence-based practice and research capacity in primary care,46⇓⇓–49,63,68,69,72,78,79,86,102,123,149,155⇓⇓⇓–159 shored up indirect support through development of agencies which became pivotal supporters of PBRNs,32,34,35,40,51,54,87,89,128,139,141,158,159,161⇓–163,188 or positively influenced the research impact of PBRNs34,39,55,82,108,113,128,132,169,171,172 and reinforced the patient-centeredness of their research38,39,56,57,62,70,73⇓–75,87,113,128
Subtheme: Professional Organizations
National or local-level professional organizations identified a need for collaborative practice-based research and helped establish it as part of the development of the academic discipline.5,11,22,28,89,92,99,110,136,141,143,148,150,175,188 A number of networks were initiated by professional organizations26,92,136,141,148,166,167,176⇓⇓–179 alone or in collaboration with academic departments and/or (research) institutes,28,64,77,82,85,92,97,109,119,130,134,178 to link PBRNs to education and professional development.
In the USA, UK and Netherlands these organizations collaborated closely with PBRNs, promoting participation in research studies among their members.22,56,92,110,126,141,150,175,235 In the Netherlands, professional organizations supported the development of Electronic Health Records (EHRs) appropriate for primary care practices.126,180 Publications suggested that international professional organizations such as the World Organization of National Colleges and Academics (WONCA), the North American Primary Care Research Group (NAPCRG), the European Academy of Pediatrics (EAP), and the European General Practice Research Network (EGPRN) played an important role in linking and motivating academics and professionals with shared research interests to initiate international,11,22,112,143,181 and national22,48,67,145,250 or even regional PBRN22,67,91 activity. WONCA also facilitated the spread of the International Classification of Primary Care (ICPC) system over the PBRN registries.7,126,130,184
Subtheme: External Funders
In addition to base-level funding from academic departments, which belong to the internal environment of PBRNs,14 PBRNs reported that received infrastructural financial support from a range of entities, including professional organizations, government-based funding agencies, academic and private institutions and foundations, national healthcare organizations, hospitals and other healthcare stakeholders,33,52,54,63,72,79,85,87,95,99,102,104,109,119,121,125,128,138⇓⇓⇓⇓⇓⇓⇓–146,250 and even HIT vendors.83
A number of PBRNs reported that their early projects were conducted on small, local grants and as they matured and their methodological approaches developed, they were able to secure more substantial funding from a broader set of sources.22,147,148 However, we found a few networks that started their research activities with sizeable funding.29,63,123,136
Some other networks used a 3-pronged mechanism to fund their research: Large-scale, externally funded projects that pooled recognized researchers, internal network-wide projects that were supported financially by the network partnerships, and small-scale projects conducted by clinician-members, which addressed their individual research interests and provided limited funding from the network.22,68,69,83,218
Subtheme: Leveraging Previous Research and PBRN Experience and Interacting with Other Networks
Our findings suggest that many PBRNs were developed based on experience gleaned from previous long-standing PBRNs and by interacting with other networks on a national or international level.11,22,45,48,63,75,92,102,109,110,112,120,130,136,181,182,183,184 In some cases, they simply relied on literature reviews and presentations/publications by other PBRNs to translate and apply knowledge gathered from networks either from the same or other countries.103,120
Some of the networks were founded to accomplish goals that were complementary to those of a previous network,111,127 or to leverage the research capacity of a dissolved1 or older network,185 or merging older networks,57,215 while others adopted specific PBRN practice models borrowed from prior networks48,92,112,181,187 and a considerable number tapped into previous research experience of their members and peer interaction.22,29,37,63,86 Federated networks could upscale research, quality improvement, and learning community activities, and provide economies of scale critical for the infrastructure of PBRNs.55,114,128,188
Subtheme: HIT and HIT Vendors
Various HIT applications were used by PBRNs at their foundation phase, as early as the 1980s.9,11,83,116,125,126,180 Contributions of HIT sustained the development of PBRN infrastructure, either directly empowering networks to meet their growing research needs, or indirectly, when the use of a specific EHR was required for PBRN membership.36,38,53,73,81⇓–83,109,130,132,133,138,146,185,191⇓–193,197,236
Many articles stated that PBRNs leveraged the potential of EHRs for healthcare data standardization, motivated HIT vendors to improve the quality of EHRs, and developed tools that facilitated data extraction and sharing,53,57,61,81,106,110,114,128,130,133,138,185,186,192⇓⇓⇓⇓–197 clinical decision-making, learning communities, and quality improvement activities.40,51,53,55,57,61,105,106,109,114,130,133,138,197
PBRNs in collaboration with vendors, gave rise to numerous innovative HIT applications for example, technologies developed by e-PCRN,105,138,160,199 the shared EHR of OCHIN32,53,107 and the data-driven CPCSSN infrastructure.109,198,200,201 The expansion of EHR use facilitated “big data” aggregation and the development of Federated Networks87,114 and Distributed Data Networks (DDNs).39,128 These “big data” networks, contributed to the utilization of PBRN data by various healthcare stakeholders, including research institutes and government organizations, and advanced data-driven and policy-informing research for the benefit of wider populations.39,90,114,123,168,237
Discussion
We conducted a scoping review of all discoverable literature on building PBRNs in an over 50-year period. Our analyses elucidated many facilitators and barriers for building PBRNs but our study was not limited to these exclusively. In this article, we present 32 key-elements related to the main themes of “Stakeholders at the Intersection between the Internal and External Environment” and “External Environment.” Some of the stakeholders that belong to the first main theme (patients, community groups and other healthcare stakeholders) gradually moved from an initially external position (“recipients” or “organizers),” toward PBRNs as “co-organizers” or “co-founders” and increasingly engaged in evidence generation, implementation, and training partnerships over time. These transitions occurred at different times for PBRNs, but they were clearly visible over the 50-year study period. Thus, the separation between the main PBRN constituents, academics and practitioner members and external stakeholder groups, has diminished over time. The main theme “External Environment” represents the social context of family medicine where PBRNs were developed, which influenced their evolution, since there was a need to adjust to new challenges, but also to leverage new opportunities and experience that emerged from each particular context. In addition, as PBRNs matured, the influence of prior experience with PBRN work and interaction with other networks increased, likewise the impact of HIT and HIT vendors.
An extensive amount of evidence from the literature that we examined suggests that there are specific processes and activities that are necessary for creating new PBRNs. The cornerstone of developing PBRNs seems to be the reciprocal relationships and trust between the actors engaged in PBRN activities.14 Other pivotal ingredients include the participation of community stakeholders and other healthcare stakeholders in PBRN activity. Just as significantly, partnerships should be developed with actors of the external environment that augment the PBRN's impact on the community that the network serves or on the broader social environment. Finally, we must note the importance of the healthcare context where PBRNs are developed and the role of infrastructural funding.
Some of our findings do not apply to all networks that are in the establishment process. For example, not all networks were shaped by all aspects of collaboration that were included in the key element “Other Aspects of Working with Healthcare Stakeholders.” In addition, some facilitators and barriers we listed in the Results section may be sensitive to the context of occurrence. For example, quality improvement tends to emerge as a strong driver to engage in a PBRN,14 but it is usually curbed by the specific healthcare environment the PBRN is situated in.
This study was based on scoping review methodology which explores and assesses the available body of literature and allows the identification of key concepts that underpin the research topic.15,248,249 In addition, for the reasons we outlined in the Methods section, we purposefully selected social network theory to organize our data and structure our analysis, which provided our specific investigative lens. Although there may be other possible approaches to analyzing the data (eg, based on organizational theory), these were not in our scope. It may be beneficial for future studies to explore these alternative methods.
Beyond the immediate findings of this study, we also generated a repository of the international literature which may provide further information on the developmental experience of PBRNs across the world. From this repository, we also plan to create various resources that may help support the diffusion of PBRNs internationally.
Connection of Findings with Social Network Theory
Our analyses, anchored in social network theory,16,18 indicated that the highest density in thematic associations in our findings was identified in “relationship building,” and it was expressed by the degrees of interconnections between the individuals (eg, practitioners or academics)14 and between nodes (eg, practices, institutes, stakeholder groups) and the actual number of ties between them. The most common features of these relationships (ties) were multiplexity, reciprocity and reachability and express the qualities the PBRNs were built on and sustained their ties. The ties are strongly homogenous within the network, less homogenous when they connect the network with “boundary spanners,” and more heterogenous when they link the network with stakeholders of the external environment.16,18 These findings underscore that in addition to academic-practitioner relationships that shaped the internal environment of PBRNs, networks developed relationships with a diverse set of actors that were “boundary spanners” or were located in the external environment and they influenced the formation of networks directly or indirectly. The intensity and density of these ties indicates that PBRNs operated as an interface for multilateral communication, interaction, and knowledge-sharing that shortened the time of spreading innovations from the “early majority” to the “late majority” of stakeholders. The first group includes practitioners and academics of the network and the second includes patients, community and other stakeholders (eg, healthcare authorities) or policymakers, who engage more actively in PBRN projects.202,203
Other Interpretations on Key Elements of PBRNs
Publications indicate that each network was influenced by the timing and location of its development and many of them reported that previous experiences with healthcare systems, professionals, research policies or resources had an impact on them.206,214 Our review suggests that the cumulative experience gained from PBRN activity and advancements in HIT was time-dependent. The same applies to the depth of engagement of patients, community members, and other healthcare stakeholders in PBRN activity. In addition, we identified bidirectional interactions between PBRNs and health policymakers, through which PBRNs became not only the subjects of policies that supported or hindered their inception or activities,154,156,158,159,165,172⇓–174,209,238⇓⇓⇓⇓–243 but they also emerged as developers of priorities that influenced health policy.9,10,13,28,33,37⇓–39,51,52,67⇓–69,76,79,88,91,97,110,118,119,125,128,135,150,170,183,211,216,217,237 In some situations, they acted as “conveners” who actively engaged health policymakers in the mission of PBRNs narrowing the “distance” between PBRNs and policymakers.9,53,85,88,89,142,237
Through collaboration with patients, community groups and other healthcare stakeholders PBRNs paved the way for direct translation of research into policy and practice.29,39,48,54,67,80,86,88,89,97,109,152 Some of these partnerships also became “communities of solutions”219 and were considered necessary to develop better health systems, health policies and guidelines.220,221 Health disparities played an important role here, through which PBRNs were able to shape a “geographic footprint” of their community to respond to the needs of their constituents and to consider the local primary care clinician as part of the community.222 Our review suggests that a strong community and health equity focus was articulated by PBRNs by envisioning community-based research to be more pragmatic when it engages a wider variety of populations (eg, rural, uninsured, minorities) that experienced community-based care as the only accessible care option. In addition, the interdependence we found between the pronounced motivation of practitioners to contribute to community health excellence and to serve these populations14 supports previous literature which suggests that PBRNs strengthen the ties between their internal structure and the community they serve when they embrace health equity and community engagement.222⇓–224
The Effect of National Environments
Variations in PBRN goals and pathways of network formation14 depended on specific national characteristics, of their health system over time that accentuated the role and the underlying culture of family medicine/general practice/primary care.
In our first scoping review,14 we found that most PBRNs were created either as a practitioner or academic initiative. In the current article, we show that networks were established either in the context of a national strategy that supported and defined their trajectory (a more centralized approach), or as a professional initiative that originated from groups of academics and individual practitioners, in addition to collaborations with professional organizations (decentralized or individualized approach). A decentralized approach for building PBRNs tended to be more common in the USA and the Netherlands, while a centralized (eg, national strategy-based) approach was more prevalent in the UK, Australia and Canada, in addition to the supportive involvement of the professional organizations in these countries.45,92,109
Our results suggest that the characteristics of the national environment and various approaches to building PBRNs14 influenced the structure of research governance (who is leading); the priorities of research (who decides on research topics); and the methodology of research. The literature indicates that research priorities in the UK are typically defined by the national healthcare system,86,204,237 while in the USA, emerging funding opportunities tend to direct, but do not completely define research priorities of PBRNs.205⇓⇓–208 Methodologically, Dutch PBRN data registry networks were positioned well to conduct observational studies, while many local, regional and statewide networks in the USA were designed to facilitate quality improvement activities,14 capitalizing on the understanding of the local culture, interests and closer relationships with their members and the community. In this context, practitioner aspirations for care quality improvement created a solid foundation and strong incentive for PBRN research, while community-based participatory research (CBPR) and patient-centered outcomes research (PCOR) methodologies also found fertile ground209 and fostered a stronger community-based role of primary healthcare.31,154,156,158,189,209⇓⇓⇓–213
Collaborations of PBRNs and the Benefits of HIT
PBRNs developed various types of collaborations and “federations” to enhance their sustainability and to foster collaborations with advocacy groups.12,137,226 They also leveraged HIT advancements that enabled the development of large databases and HIT-driven multi-network collaborations57,61,114,123,128,138,168,190,197 This type of infrastructure helped extended access to a variety of populations, leveraged wider stakeholder interests, engaged in multiple types of research and focused on research topics and innovative methodologies190,229 leading to broader generalizability.123,168,244,245 These resources became more common in the late 2000s, which was expressed by the development “meta-networks” (ie, networks of networks) in USA and UK.14,86,123,170,189,227,228 PBRN meta-networks asked more ambitious research questions by pooling their resources and expertise and managed diversified research portfolios and business models that facilitated external stakeholders to influence PBRN research priorities and to accelerate the dissemination of research findings.114,189,230,231
Financial Stability and Sustainability Models
The timing of building networks and the characteristics of the national environment defined PBRN management approaches and their funding opportunities. Early regional American and Dutch PBRNs received limited infrastructural support from professional or academic organizations. Conversely, the binational ASPN network received funding from private foundations and national organizations. Networks gradually benefited from supportive national strategies and more tangible infrastructural support from various funding bodies, as a result of recognizing the value of PBRN research and its impact on healthcare and policy.29,36,58,68,85,89,114,121,128,137,158,159,165,170,227,228 This underscores the importance of external relationships and support in the development of PBRNs,209,210,246 but also the risk of becoming dependent on these relationships.206,246,247 In addition, research funds targeting the collection of data without much relevance to primary care, might also be seen as barrier. Some PBRNs responded to financial instability by developing either a model of limited resources125,153,232 or a business model that involved relationships with stakeholders in the external environment, as we reported in our previous article.14
Limitations
In this scoping review we completed the widest possible search in English-language publications and sources, and we explored a 10-year period of each network's initial development, which may have influenced our frame of reference. Therefore, PBRNs that published in other than English language or never published, although they may have substantial experience, are not included in this review. However, the parameters we used were congruent with the temporal and source-language distribution of most PBRN literature.
The list of PBRNs that met the inclusion criteria is more limited than those that ever existed in the USA,233 Australia,238,250 the UK48, Canada,234 the Netherlands,175 and in web-based sources that refer to particular PBRNs, since there was no supporting literature in every case. We also excluded articles with insufficient information on the development of PBRNs.
Scoping reviews may carry selection bias, if all available data are not identified or included in the study. Inductive thematic analysis methodology was implemented in this study, however, some a priori knowledge about PBRNs may also contributed to the development of the thematic model.
Conclusions
This analysis highlights the importance of the external environment in the development of PBRNs, in addition to the previously reported role of the internal environment. A key finding is that “internalizing” the “outside world,” by involving patients, community leaders, health authorities and policymakers in their mission, makes the functioning of PBRNs more robust and the impact of their work on the health of populations more tangible. Understanding the health and social environment in which they operate is therefore a key to success in PBRN development.
Appendix
Inclusion and Exclusion Criteria for the Scoping Review
Overarching Thematic Framework for the Establishment of Practice-Based Research Networks (PBRNs) Focusing on the Themes of the External Environment and Stakeholders at the Intersection between the Internal and External Environment Described in This Article
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/4/762.full.
- Received for publication October 15, 2021.
- Revision received January 6, 2022.
- Revision received January 14, 2022.
- Accepted for publication January 20, 2022.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.↵
- 203.↵
- 204.↵
- 205.↵
- 206.↵
- 207.↵
- 208.↵
- 209.↵
- 210.↵
- 211.↵
- 212.↵
- 213.↵
- 214.↵
- 215.↵
- 216.↵
- 217.↵
- 218.↵
- 219.↵
- 220.↵
- 221.↵
- 222.↵
- 223.↵
- 224.↵
- 226.↵
- 227.↵
- 228.↵
- 229.↵
- 230.↵
- 231.↵
- 232.↵
- 233.↵
- 234.↵
- 235.↵
- 236.↵
- 237.↵
- 238.↵
- 239.↵
- 240.↵
- 241.↵
- 242.↵
- 243.↵
- 244.↵
- 245.↵
- 246.↵
- 247.↵
- 248.↵
- 249.↵
- 250.↵




{kind=link}
{kind=link}
{kind=link}
{kind=link}