
Abstract
Objective: The benefits of Social Determinants of Health (SDoH) is well documented but several studies highlight the complexity of collecting and standardizing SDoH data in a way that makes it relevant to the standard clinical interaction. The purpose of this study is to examine how leveraging an Electronic Health Record (EHR) system can facilitate SDoH screening and its integration into Primary Care encounters, while also using the data collected to meet the identified needs.
Methods: This is an observational study design. EHR and SDoH screening data from 2020 to 2023 at 3 primary care sites were gathered. The study was implemented in 3 phases to streamline and establish the screening and referral processes.
Results: SDoH screening increased by 95% from 2020 to 2022 with a consequent increase in social work referrals and the allocation of resources to a targeted patient population.
Conclusion: Identifying SDoH unique to a community or population can be strategically used to deliver relevant and timely services to patients. This fosters a multidisciplinary, collaborative and integrated approach to patient care.
- Community Medicine
- Community-Based Participatory Research
- Doctor-Patient Relations
- Electronic Health Records
- Family Medicine
- Health Disparities
- Needs Assessment
- Physician's Practice Patterns
- Primary Health Care
- Resource Allocation
- Social Determinants of Health
Introduction
Interventions aimed at addressing Social Determinants of Health (SDoH) reduce health care costs and improve health outcomes, including those related to obesity, diabetes, and asthma.1⇓⇓–4 As a result, efforts to address SDoH are increasingly being prioritized in the health care industry.1 Nonmedical factors such as health behaviors, social, and environmental factors, which fall under the umbrella of SDoH, have been shown to have as much impact on general health as medical factors.5,6 To adopt a more comprehensive approach to health care, initiatives like Medicaid, the Children’s Health Insurance Program (CHIP), and the Access Commission’s Delivery System Reform Incentive (which aims to fundamentally redesign state Medicaid programs) are offering financial incentives to bring social determinants to the attention of clinicians.6 In the past, data on individual-level determinants were collected using various complicated and time-consuming survey instruments, including the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE), among others. While these surveys aim to comprehensively capture measures, they are not easily integrated into short primary care visits. New, innovative strategies are required to more effectively capture these factors.
Electronic Health Records (EHR) are integral to physicians' workflows and could serve as effective tools for capturing SDoH.7 As of 2021, nearly 9 out of 10 (88%) of US office-based clinicians had adopted an EHR.8 The digitization of clinical records has brought new opportunities to collect nonclinical information for population health purposes.9 This includes data elements such as age, race, and ethnicity, along with features covering lifestyle domains like preferred languages, smoking status, environmental factors, social housing, and financial resources.9 These expanded data provide an existing opportunity to better screen for, identify, and address SDoH.
Star Community Health, a Federally Qualified Health Center Look-Alike (FQHC-LA) with 3 primary care sites, embarked on a targeted effort to leverage the EHR system (EPIC) to better capture SDoH. The Community Health Centers (CHS) see together 45,000–underserved, uninsured, and insured–patients from various races and ethnicities in an urban setting. The primary goal of this initiative was to increase the frequency of SDoH screenings within the health clinics, in alignment with the regulation of the Health Resources and Services Administration (HRSA), which oversees FQHC-LAs’ integration of SDoH into health center operations. This article describes an iterative 3-phase project to develop a screening tool for SDoH and to develop a subsequent referral workflow for patients with unmet social needs.
Methods
The intervention was executed in 3 phases. The goal of each phase was to refine the screening process from the previous phase.
Phase 1 (2020 to 2021)
In the first phase, an SDoH questionnaire was generated by selecting predesigned questions from an EPIC Healthy Planet–a population health management module from the EPIC system–guided by our health needs assessment. The 2019 St. Luke’s University Health Network Community Health Needs Assessment (CHNA) was used to determine the most prescient social needs to be screened.10 Ten screening questions were ultimately chosen, focusing on key aspects of health including food access, financial insecurity, transportation, alcohol use, smoking, and social history. These questions were integrated with various parts of the screening and rooming protocol found in EPIC and required documentation during patient interviews.
In the course of administering the survey, it became apparent that many patients did not fully disclose their needs, especially those related to financial, housing, or transportation access, possibly due to perceived stigmas. For example, a patient would state they have no financial need when initially questioned and only later do they divulge that information during their interaction with the clinician. In an effort to address the possibility that staff behavior might have contributed to this barrier, an effort was made to educate the medical team to address these stigmas in patient care. The training incorporated information and demonstration from the FindHelp website. FindHelp is a national database of assistance programs for patients with social needs. The FindHelp.org website serves as an endpoint in the referral pipeline, where users can be connected to local resources such as food, housing, and financial assistance. The online training was a combination of explanation of the process, sensitivity when asking questions, and FindHelp education. In addition to the online training, there were 12 in-person training sessions for medical assistants, clerical staff, and medical personnel on SDoH and how to approach these questions with patients. All these resources were then integrated into the onboarding training for new staff members joining the team.
Phase 2 (Mid-2021 to Dec 2022)
There was a significant time constraint with asking the 10-point questionnaire, and patients felt overwhelmed during the initial phase. The Community Needs Assessment tool was used to streamline the screening process by selecting the top 3 needs most represented among the patient population: food insecurity, financial constraints, and transportation access (Figure 1). To further simplify the process, these questions–previously scattered in the EHR–were consolidated into an EPIC rooming tab and integrated into the rooming procedure. The EHR has a rooming section built for all rooming tasks. Medical assistants (MAs), licensed practical nurses (LPNs), and registered nurses (RNs) asked patients the questions and entered responses into the EHR. In addition, the questions were available on article and could be completed in the waiting room, then entered into the EHR by the rooming staff. The questions were also accessible in the patient electronic health portal to be answered before a visit. Some practices adopted a hybrid approach, using an iPad for patients to answer the questions, with the rooming staff later entering the responses into the EHR. If a patient responded positively to one or more of these domains, a Best Practice Advisory (BPA) pop-up screen was triggered. The BPA in this phase automated a social work referral, and the result was entered into a database specific to the patient's SDoH needs. As part of this process, patients were also connected to the FindHelp.org resource website, linking them to resources in their ZIP code that addressed their specific needs. The team from FindHelp.org worked closely with our leadership and care management teams to assist with creating and streamlining a process for patients who provided positive responses to SDoH surveys. During this process, we also established community partnerships to address the needs identified through the referrals. A training module was also integrated into the employee learning platform, a mandatory online education resource for all health center employees.

The EPIC Toolbox Questionnaire is available to staff during the rooming process. The process is simplified through a click-box selection function.
Phase 3 (Jan 2023 to 2024)
Once the workflow and EPIC integration were established, a comprehensive discussion shared between operational and clinical leadership took place, focusing on the roles and responsibilities of clinicians in light of these changes. The automated workflow referring patients with positive screens to social work was revised due to the overwhelming burden on care managers. When a positive answer triggered a BPA, rather than automating the referral, the patient was first asked if they would like a social work consult. If the patient agreed, a referral was sent and signed by the clinicians during the encounter. Furthermore, 2 separate FindHelp.org links into EPIC were integrated, making them easily accessible to both staff in the EHR and to patients on their MyChart platform–a secure online portal that allows patients to access their personal health information and communicate with their health care clinicians. The network’s case management and community outreach manager continued to work on engaging the community to be able to track how many referrals resulted in resource allocation. In addition, staff were trained to navigate the FindHelp.org resource page and monitor patients who use the community services. Staff began to collect data to measure impact/outcome.
Results
Data were tracked across 3 medical primary care sites of Star Community Health in the Lehigh Valley district (Table 1). The primary care sites saw 35,105 patients in 2020, with only 39% of them being screened for SDoH during phase 1 of the study. In 2021, phase 2 of the process was initiated. Out of the 41,874 patients seen at the center, 51% were screened for SDoH. In 2022, among the 42,335 patients seen, 76% were screened for SDoH. In the year 2020, 24% of the screened patients had positive screening results. In 2021, this figure was 18%. Out of the 42,335 screened in 2022, 15% received a positive screening result. Among them, 2,623 reported financial hardship, while 1,390 patients confirmed food insecurity, and 967 reported transportation issues. FindHelp.org resources were provided at that time.
SDoH Screening
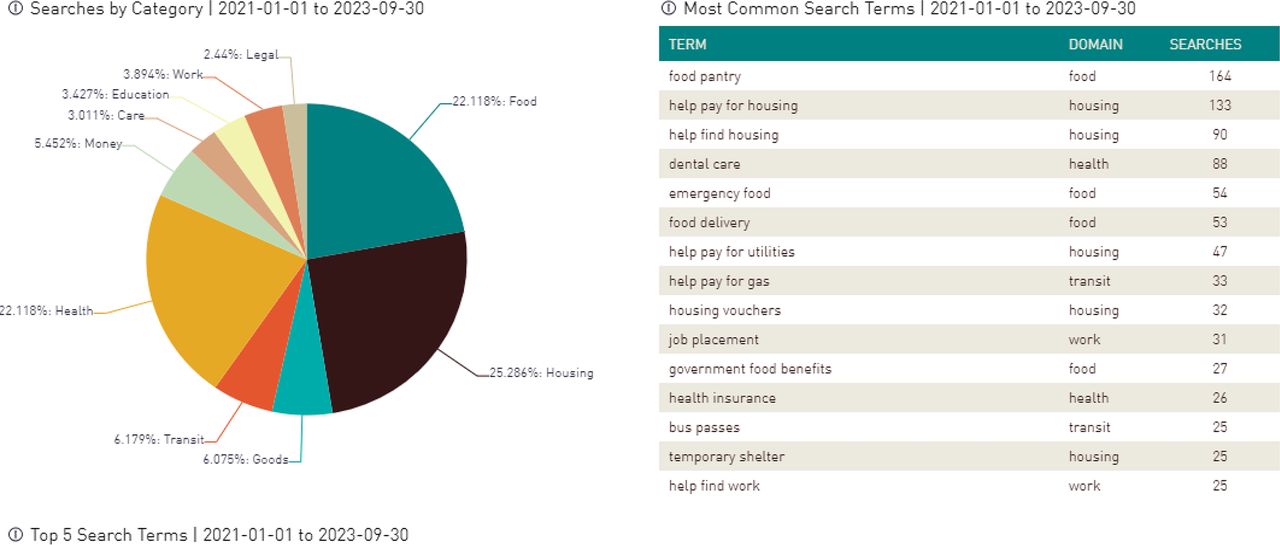
In 2020, there were only 111 users for the FindHelp.org website, and 16 of them were connected with programs. The user count rose to 2,283 in 2021, with 178 patients being connected to a program, and 3,888 in 2022, with 977 being connected to a program. In that time, 25.27% of the searches were related to housing, and 22% were related to food (Figure 2). Following Phase 3 implementation in 2022, ambulatory referrals to social work totaled 375, including 12 from FindHelp.org. During that time, 97% of the social work referrals made contact with the patients to directly address their positive screen.

Illustrates the search interaction on FindHelp.org by category, with Food, Health, and Housing being the most searched functions.
Discussion
There is strong evidence that integrating SDoH into EHRs can assist in risk assessment and predicting health care utilization and health outcomes.9 EHR offers the potential to be able to integrate and aggregate patient-level SDoH across settings and over time.9 This study was conducted across multiple Star Community Health center sites with different patient demographics to better capture the drivers of health in each unique population and assist in strategizing the approach to improve the effectiveness of care.11 The administrative team prioritized this task due to new HRSA suggestions and recent literature demonstrating SDoH accounting for up to 40% of a patient's overall health.12 Before the intervention, patient screening was not routinely done. Strategy and training were the primary drivers of the increase in screening from 39% to 76% of the patient encounters—a 95% increase over 3 years. While there was an increase in the number of patients that were screened, it is important to note that there was a decrease in the percentage of positive patients that were captured. However, despite the percentage decrease, there was an increase in the absolute number of positive screenings.
Screening tools to identify individuals with unmet social needs help to link patients to services.13 Nevertheless, capturing patient-specific information has its challenges.11 Nationally, there is a lack of consensus on standards for capturing and representing social determinants of health in EHRs.12,14 To address this shortcoming, the Institution of Medicine (IOM) recently called for the Office of the National Coordinator for Health IT (ONC) to require vendors to expand their structured fields as a condition of product certification.12 The IOM requested that each EHR platform include standard measures for educational attainment, financial resources strain, stress depression, physical activity, social isolation, and neighborhood median household income to better identify risk for SDoH factors such as food inequities and lack of housing.12 While this process is still in development, consolidating this information and simplifying it into 3 prompt questionnaires allowed our teams to quickly identify and develop a workflow for referrals following positive screenings.
In the absence of a concrete referral workflow, simply collecting SDoH data does not necessarily yield social service referrals.1,14 This study has made progress in overcoming some of these challenges by iteratively collecting and refining referral workflow data in phases. For instance, the FindHelp.org website link serves as a resource repository and is being developed to capture patient-specific access to these resources, making it a potent and effective tool for connecting SDoH data.9 Furthermore, in the third phase of the study, we modified the workflow such that patients with positive SDoH screenings were automatically referred to social work. Although the 2023 data collection is not complete, referrals to social work increased from 375 to 2,226 in 2023—nearly a fivefold increase. Future information will be available regarding resources used by patients working with ambulatory social workers.
Limitations of this study include patients without internet access, thereby being unable to use the FindHelp.org website. These individuals are not represented in the data tracking, potentially excluding critical cases. Moreover, a portion of the homeless population lacks working phones, hindering communication for social work staff postreferral—though we try to have care management meet with the patient during the time of visit with this select population. These patients miss out on connecting with intended services. Future studies should longitudinally follow patients to assess overall health and determine if FindHelp.org and social work referrals adequately address critical needs. There is ongoing study to identify the rate at which patients use or connect to the resources once the referrals are processed and to capture and sort the demographics.
Conclusion
SDoH significantly impacts patient outcomes and plays a crucial role in patient care alongside clinical interventions. Therefore, giving clinicians access to patient-centered SDoH information in real-time, embedded in existing clinical workflows, is critical.6,15 Star Community Health's targeted approach, streamlining the process and screening questions in the EHR workspace, has effectively increased the number of patients screened in the community care centers. The links to resources on the FindHelp.org website and referrals to social work have proven to intuitively connect patients to essential resources for their well-being. Leveraging technology will continue to be a key factor in bridging gaps in patient care and improving access.
Acknowledgments
The authors thank Dr. Robert Langan for his editorial assistance.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/38/1/9.full.
- Received for publication April 22, 2024.
- Revision received August 17, 2024.
- Accepted for publication August 26, 2024.




{kind=link}
{kind=link}