
Abstract
The Teaching Health Center Graduate Medical Education (THCGME) program is a decentralized residency training component of the Affordable Care Act, created to combat critical shortages and maldistribution of primary care physicians. The Accreditation Council of Graduate Medical Education and federal data reveal that the THCGME program accounted for 33% of the net increase in family medicine residency positions between 2011 and 2015. However, amid concerns about the program's stability, the contribution of the THCGME program to the net increase fell to 7% after 2015.
- Accreditation
- Graduate Medical Education
- Patient Protection and Affordable Care Act
- Primary Care Physicians
The Teaching Health Center Graduate Medical Education (THCGME) program began as a 5-year initiative under the Patient Protection and Affordable Care Act to increase the number of primary care residents and dentists trained in underserved, community, nonhospital settings such as rural health clinics and federally qualified health centers. Results to date include 11 new and 14 expanded teaching health center (THC) family medicine residency programs.1 In 2015, the Medicare Access and CHIP Reauthorization Act renewed funding for the THC program for an additional 2 years but reduced by 40% the amount of funding THCs received per resident ($150,000 to $95,000).
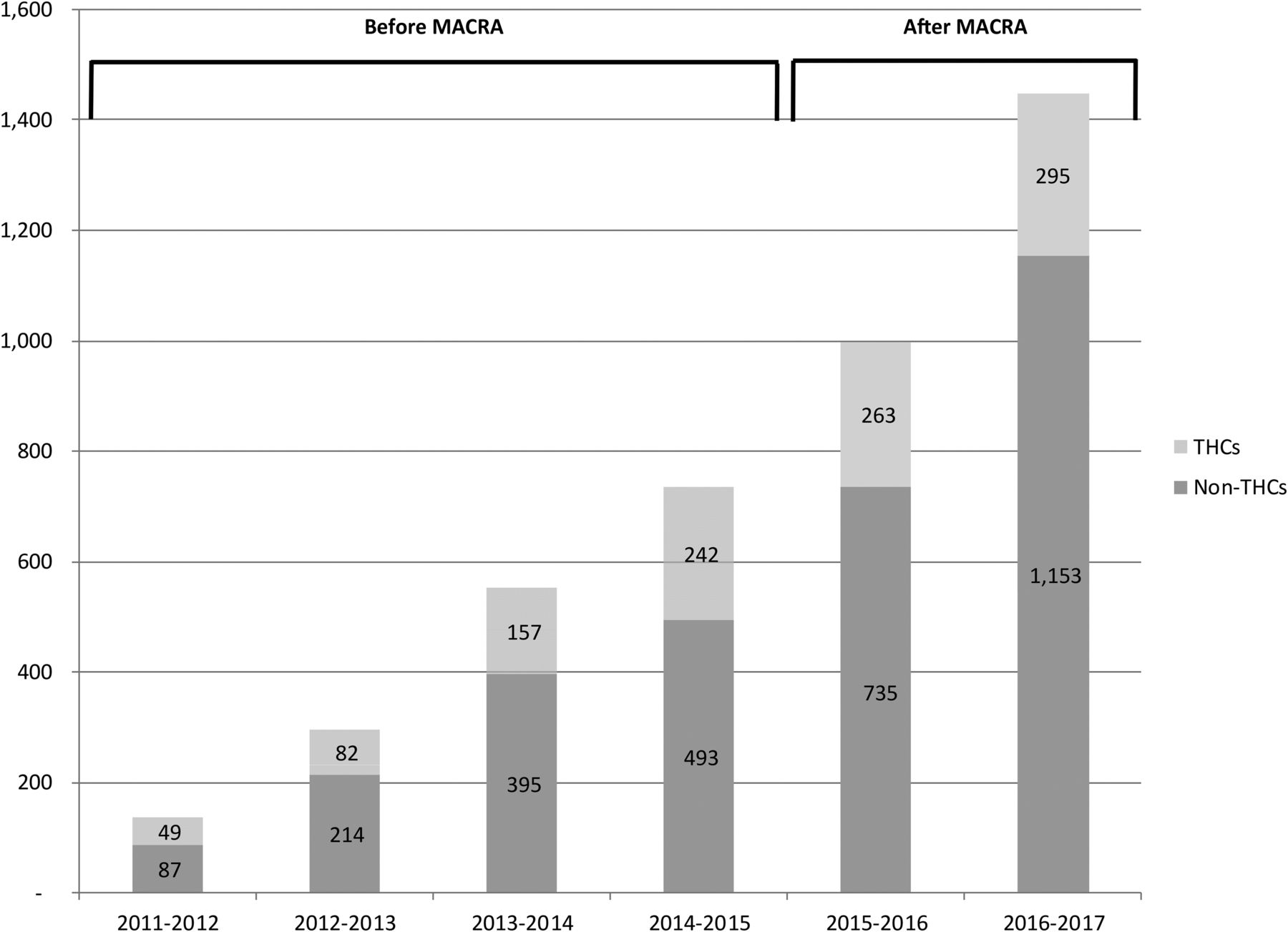
Combining Accreditation Council of Graduate Medical Education and Health Resources and Services Administration data, we found that family medicine residency training capacity increased by 735 positions (a 6% increase) between 2011 and 2015; 33% of this net increase was attributable to THCGME programs1 (Figure 1). Following the Medicare Access and CHIP Reauthorization Act and changes in funding, no new THCs were funded, and the net increase attributable to THCs fell to 7%.
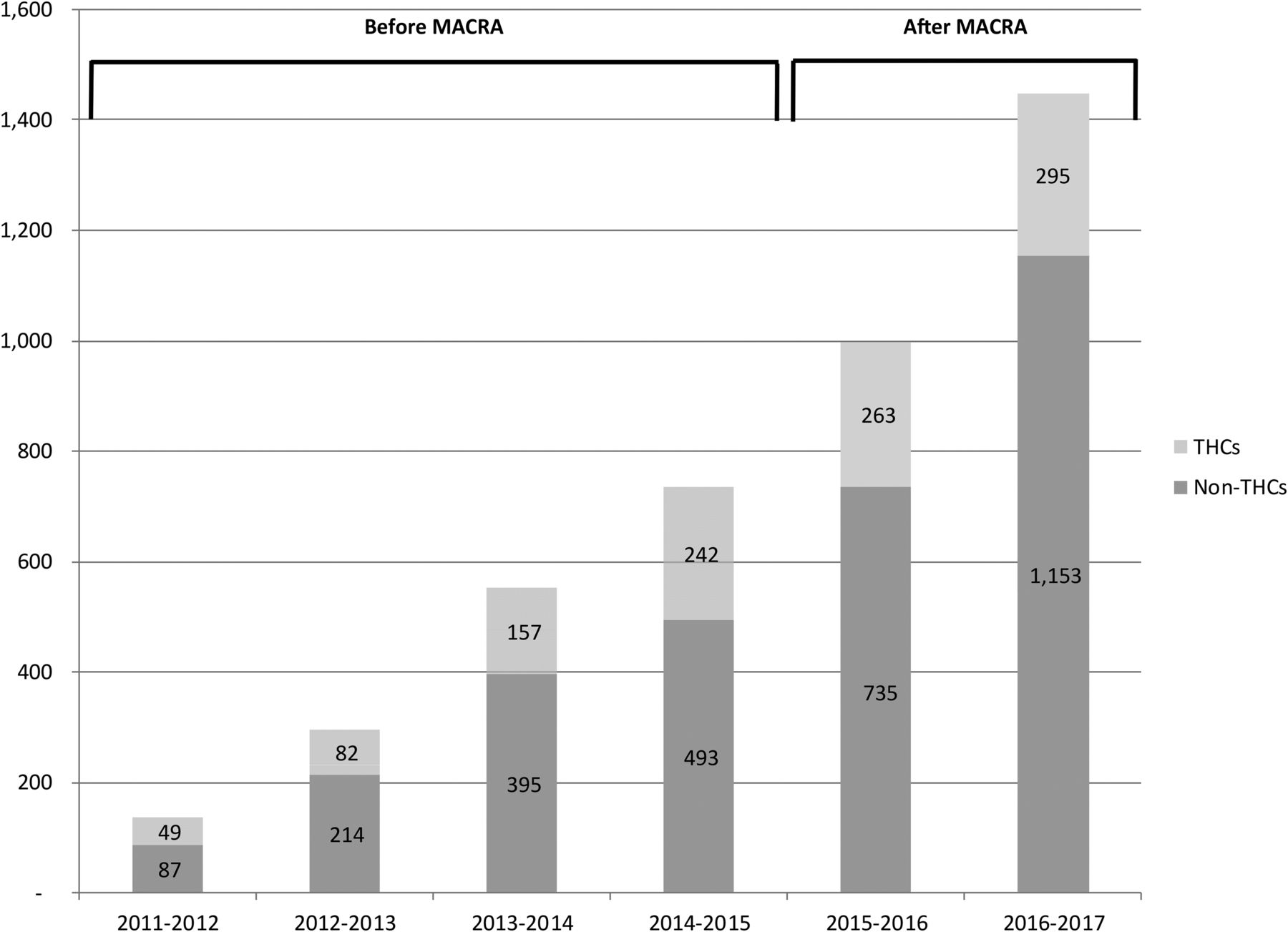
Cumulative increase in family medicine residency positions attributable to teaching health centers (THCs) versus non-THCs. MACRA, Medicare Access and CHIP Reauthorization Act.
Two factors potentially account for this decrease. First, THCGME's reduced funding and short extension were associated with very few additional THCs. Second, spurred by state and federal graduate medical education initiatives, non-THC, hospital-based positions expanded. The state of Georgia, for instance, launched an initiative to train by 2018 an additional 400 residents (nearly 80 of whom are projected to be in family medicine) through the creation of residencies at new teaching hospitals.2 While non-THC, hospital-based residencies can also address maldistribution, research suggests that training in nonhospital, underserved settings, such as at THCs, provide a greater return, with graduates more likely to treat underserved populations.3,4
With graduate medical education funding capped under the Balanced Budget Act of 1997, policymakers need new programs to address projected primary care physician shortages. THCGME provides an innovative vehicle for addressing primary care workforce needs and maldistribution. Given the instability and decline of funding, however, THCGME leaders have raised concerns about the program's viability, particularly since the amount received falls short of the THC per-resident net cost, estimated to be >$150,000.5,6 If policymakers wish to build on community-based training to address projected primary care shortages and maldistribution, THCGME funding needs to be renewed, stabilized, and expanded.7
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
See Related Commentary on Page 275.
To see this article online, please go to: http://jabfm.org/content/30/3/279.full.
- Received for publication October 28, 2016.
- Revision received February 6, 2017.
- Accepted for publication February 6, 2017.




{kind=link}