
Abstract
Based on a 2023 survey of second year family medicine residents, 29% report that they plan to incorporate gender affirming care (GAC) into their future practice with those training in states with legal restrictions on GAC being less likely to do so. By identifying and supporting future health care professionals committed to providing these services, policy makers and workforce planners can ensure that there are enough trained professionals to meet growing demand and ensure equitable access.
Gender-affirming care (GAC), is a vital component of inclusive health care that encompasses “…an array of services that may include medical, surgical, mental health, and nonmedical services for transgender and nonbinary people”1, remains limited in access.2 Family physicians, given the breadth of their training and wide geographic distribution, are uniquely positioned to provide GAC. The American Academy of Family Physicians policy states that family physicians are well suited to provide GAC as part of comprehensive primary care.3 Despite increased utilization of GAC,4 there are social and legal barriers to providing GAC. Currently 23 states have some legal restrictions on providing GAC to children/adolescents with 7 states also have restrictions to access for adults which impacts 38% of transgender youth.5,6 A 2020 survey of family medicine program directors found that over half of residencies were incorporating GAC into their curriculum and that residents expressed a desire to provide GAC after graduation.7 Little is known about current residents’ future practice intentions to provide GAC and the impact of current practice restrictions.
We used data from PGY2 family medicine residents completing the American Board of Family Medicine (ABFM) National Resident Survey administered at the end of the October 2023 In-Training Examination. We determined the proportion of respondents who indicated that they intend to personally provide GAC after residency graduation. The question did not specify age groups or specific modality of intended GAC. The Kaiser Family Foundation provided a list of states that had laws banning GAC up to the age of 18, this data were used to determine the presence of GAC restrictions at the time of the survey.5 This list includes states with restrictions for adults as well. We calculated the mean percentage of residents in each state intending to provide GAC and categorized it as low (<20%), medium (20 to 50%), and high (>50%). The American Academy of Family Physicians Institutional Review Board approved this study.
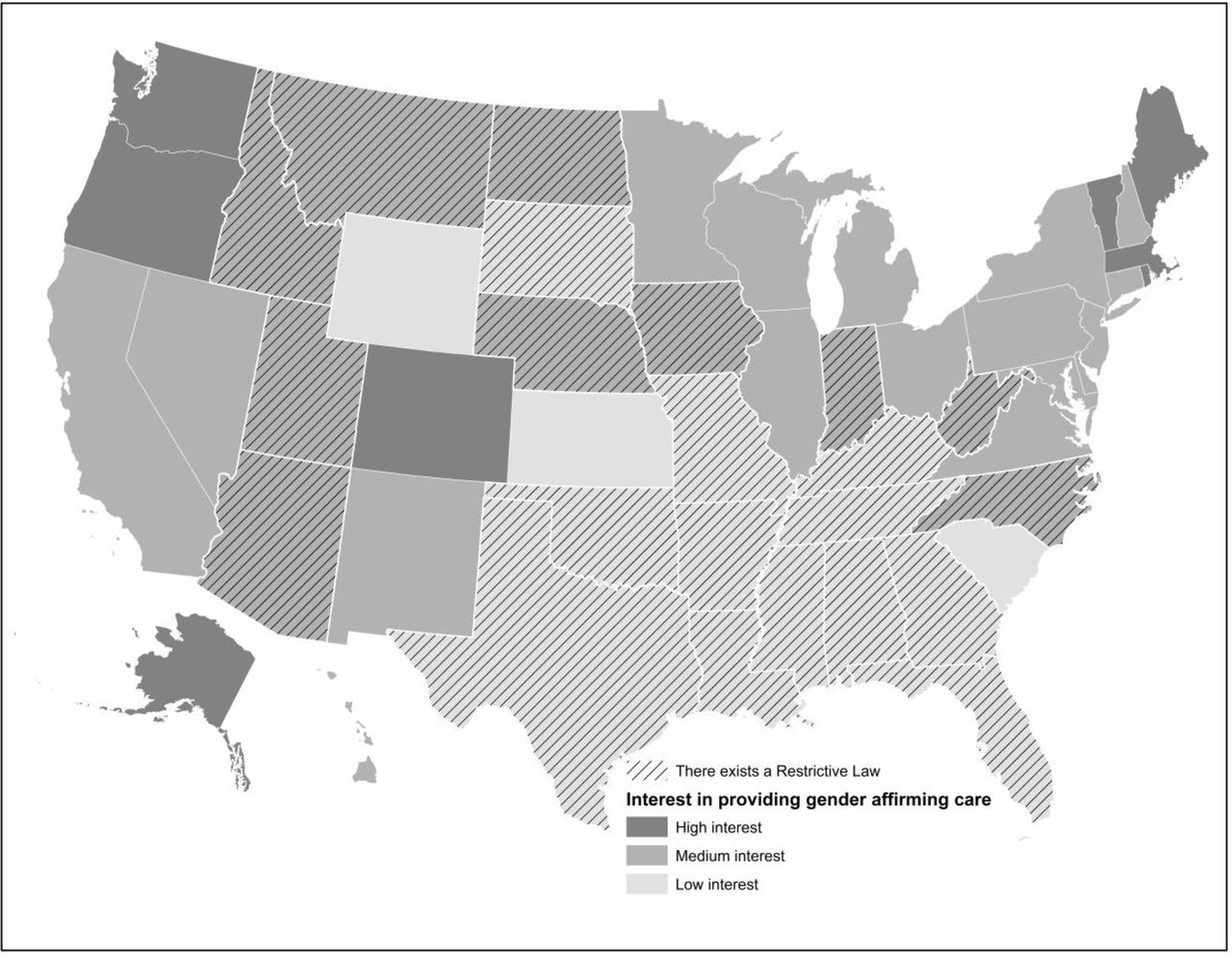
Our sample included 2584 PGY2 residents who completed questions on scope of practice (response rate: 53.5%). Overall 748 (28.9%) responding that they planned to include GAC in their future practice. Residents training in states with restrictions were significantly less likely to include GAC in their future practice (21.2% in states with restrictions vs 33.9% in states without restrictions, P-value = 0.0057). State level variation by restrictions is noted (Figure 1).
Slightly less than a third of family medicine residents plan to incorporate GAC into their future practice, despite the AAFP stating GAC is part of comprehensive primary care and a 2020 survey of program directors indicated that over half of residencies had incorporated GAC into their curricula. This indicates there is need for further training and other supports to overcome barriers so that GAC is more commonly incorporated into primary care practice. The political and legal environment of a training program – specifically legal restrictions on medical care such as GAC – is associated with fewer residents planning to include this care in their future practice. By identifying and supporting future health care professionals committed to providing these services, policy makers and workforce planners can ensure that there are enough trained professionals to meet growing demand and ensure equitable access.

Interest of second year family medicine residents in providing gender affirming care by state level restrictions.
Acknowledgments
Authors would like to thank Mark Carrozza, MS, who created the map.
Notes
See Related Commentary on Page 976.
This article was externally peer reviewed.
Conflict of interest: Ms. Fleishcer and Dr. Peterson are employees of the American Board of Family Medicine.
Funding: Dr. Barr received financial support from the American Board of Family Medicine Foundation.
To see this article online, please go to: http://jabfm.org/content/37/5/974.full.
- Received for publication February 20, 2024.
- Revision received May 1, 2024.
- Accepted for publication May 13, 2024.




{kind=link}