
Article Figures & Data
Figures
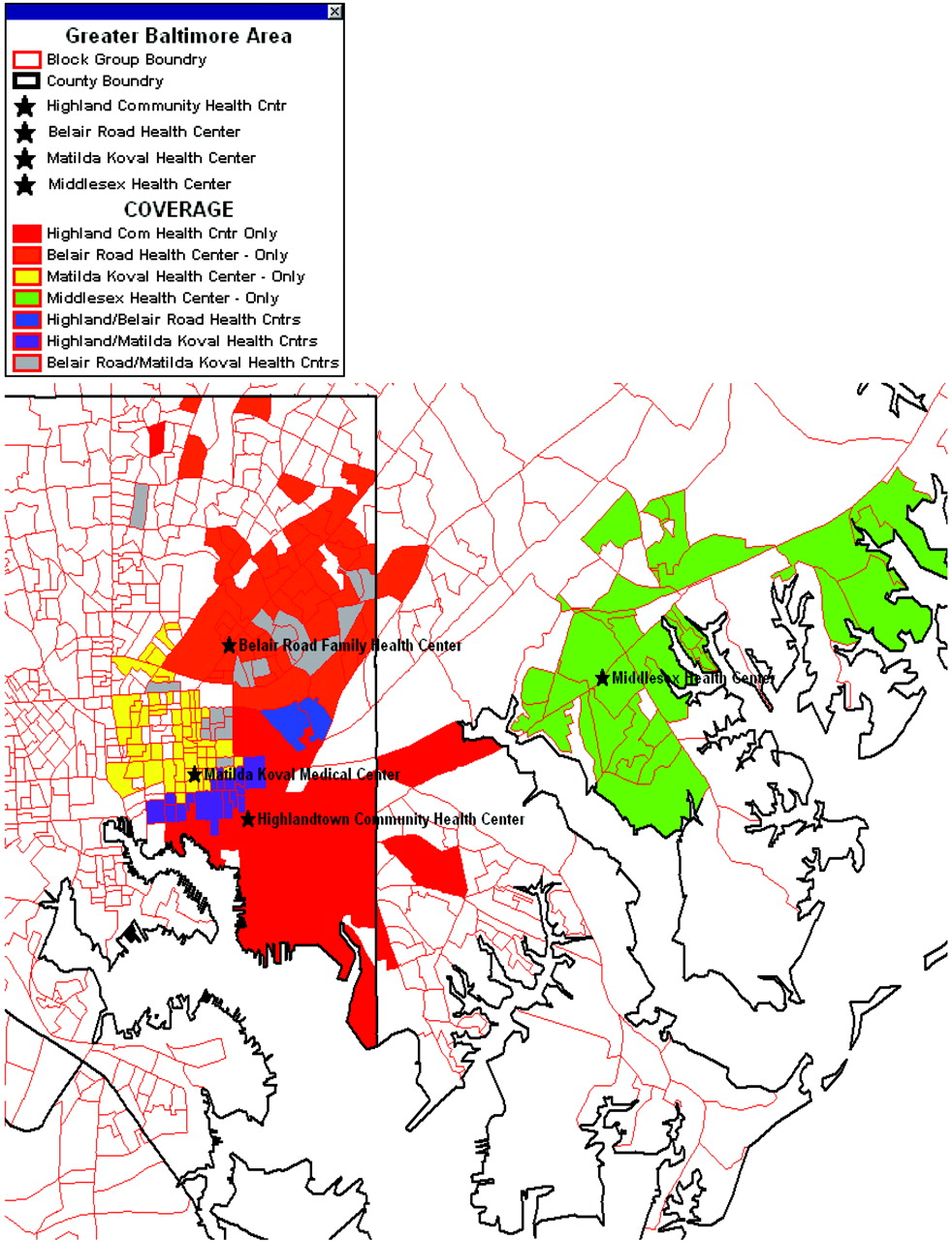
- Figure 1.
Baltimore Medical Systems, Inc.'s’ aggregate service area. Using billing and administrative data assigned to clinic, this map shows the service area (census tract) of 4 BMSI clinics and their overlap.
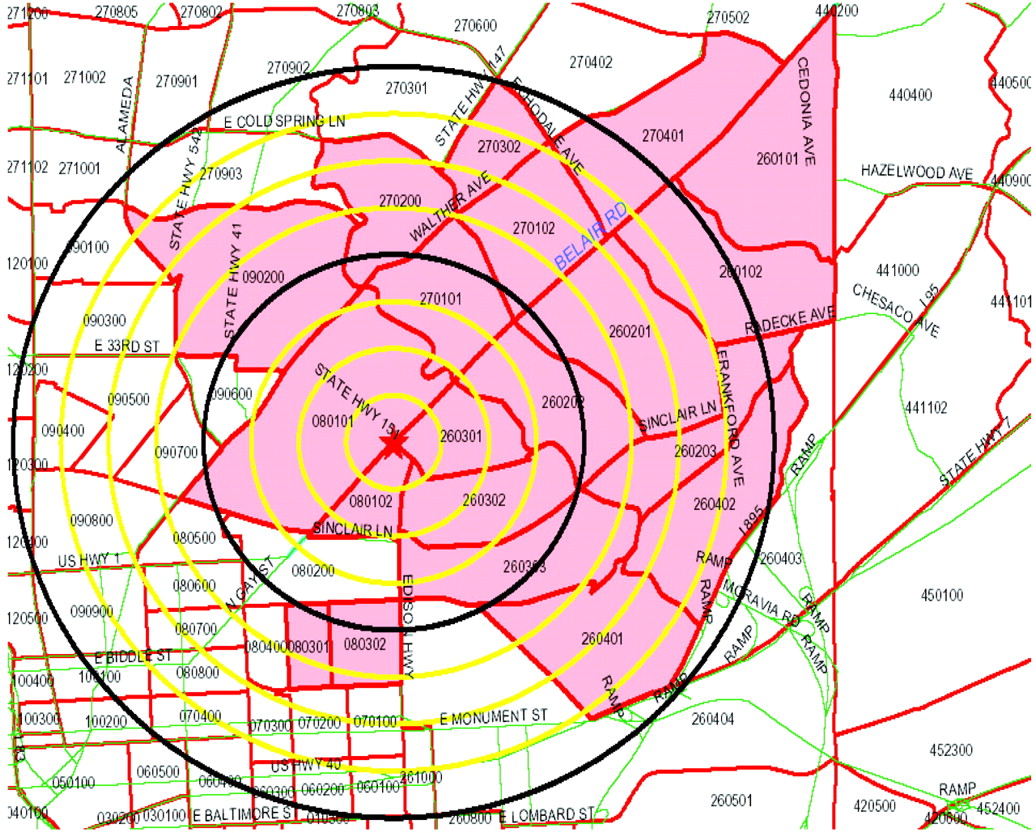
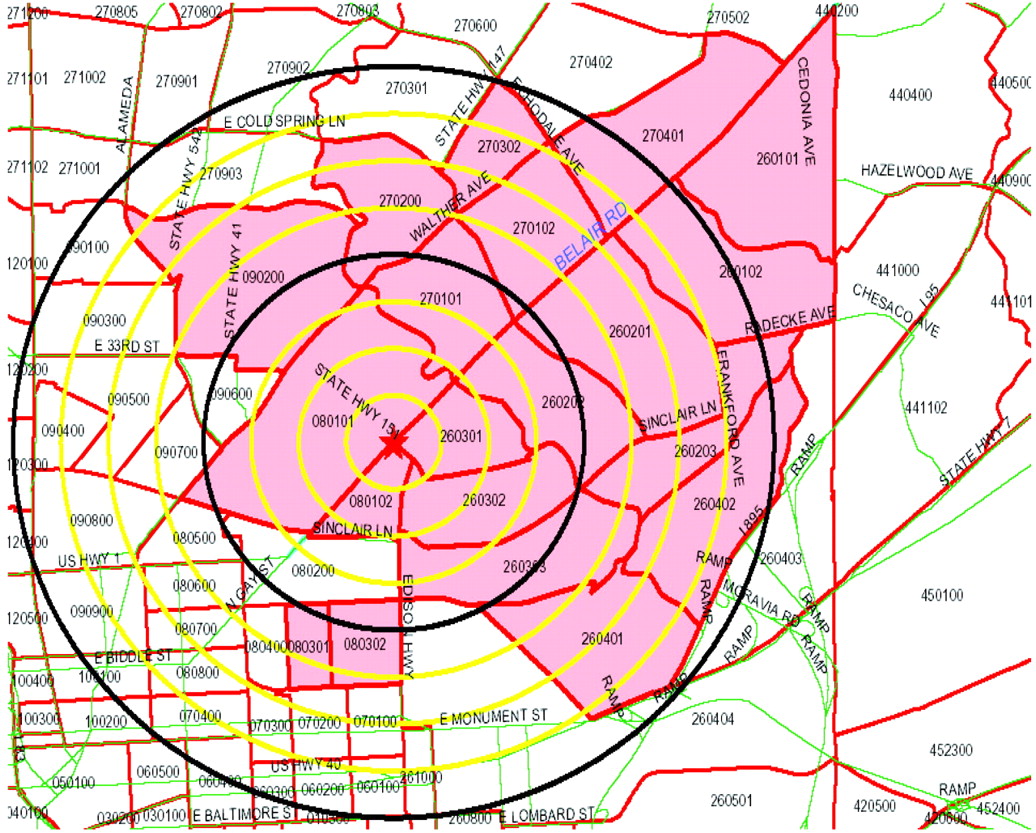
- Figure 2.
This map demonstrates the federally designated medically underserved area that a single Baltimore Medical Systems, Inc., clinic receives federal funding to serve, with quarter-mile radii from clinic marked out to 2 miles. Discrepancies between maps of these “ideal” service areas and the actual service areas (such as that in Figure 1) were cited by BMSI executives as informative and surprising; they later used the actual service area information to change a relocation decision based previously on medically underserved area alone.
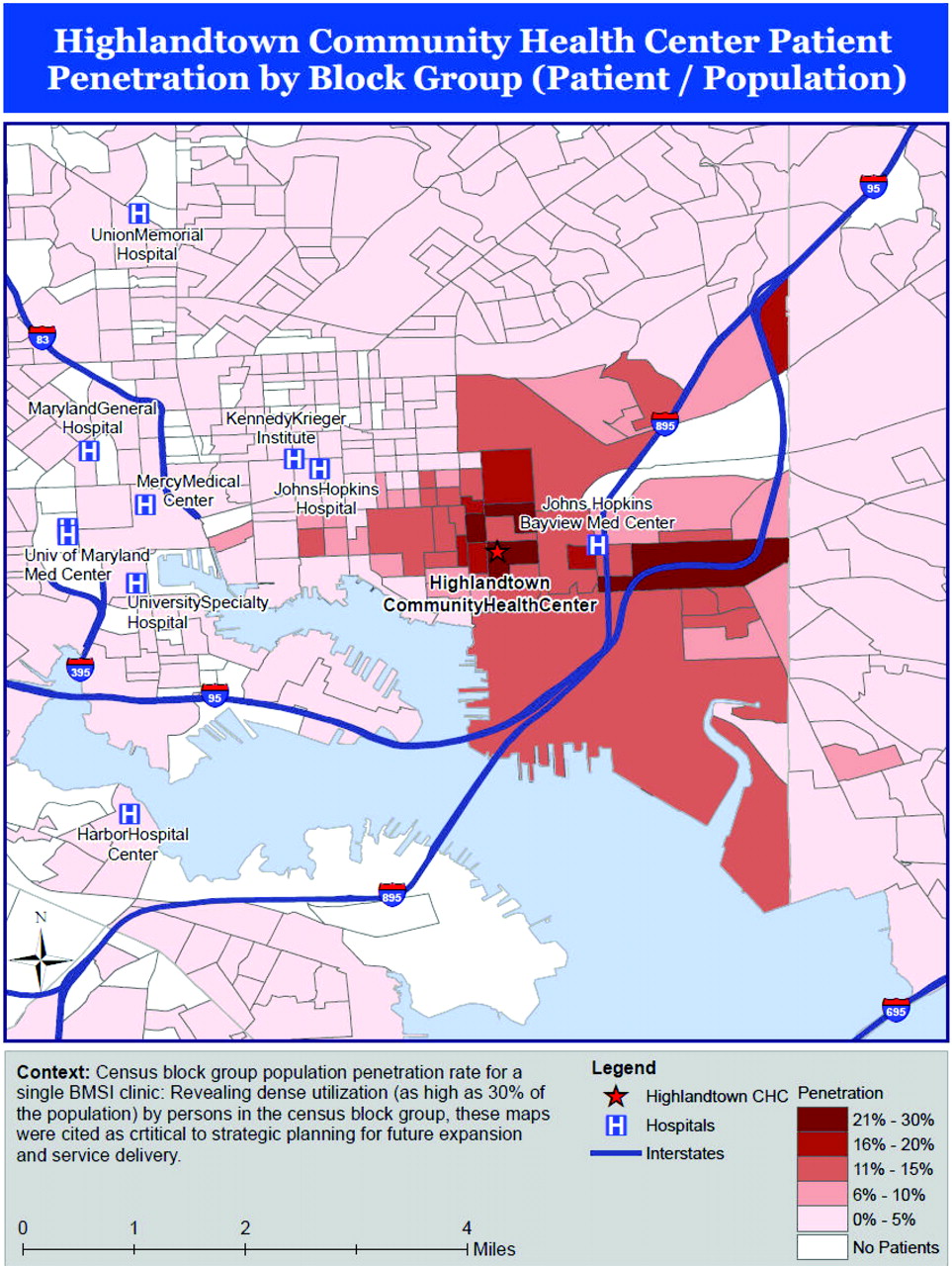
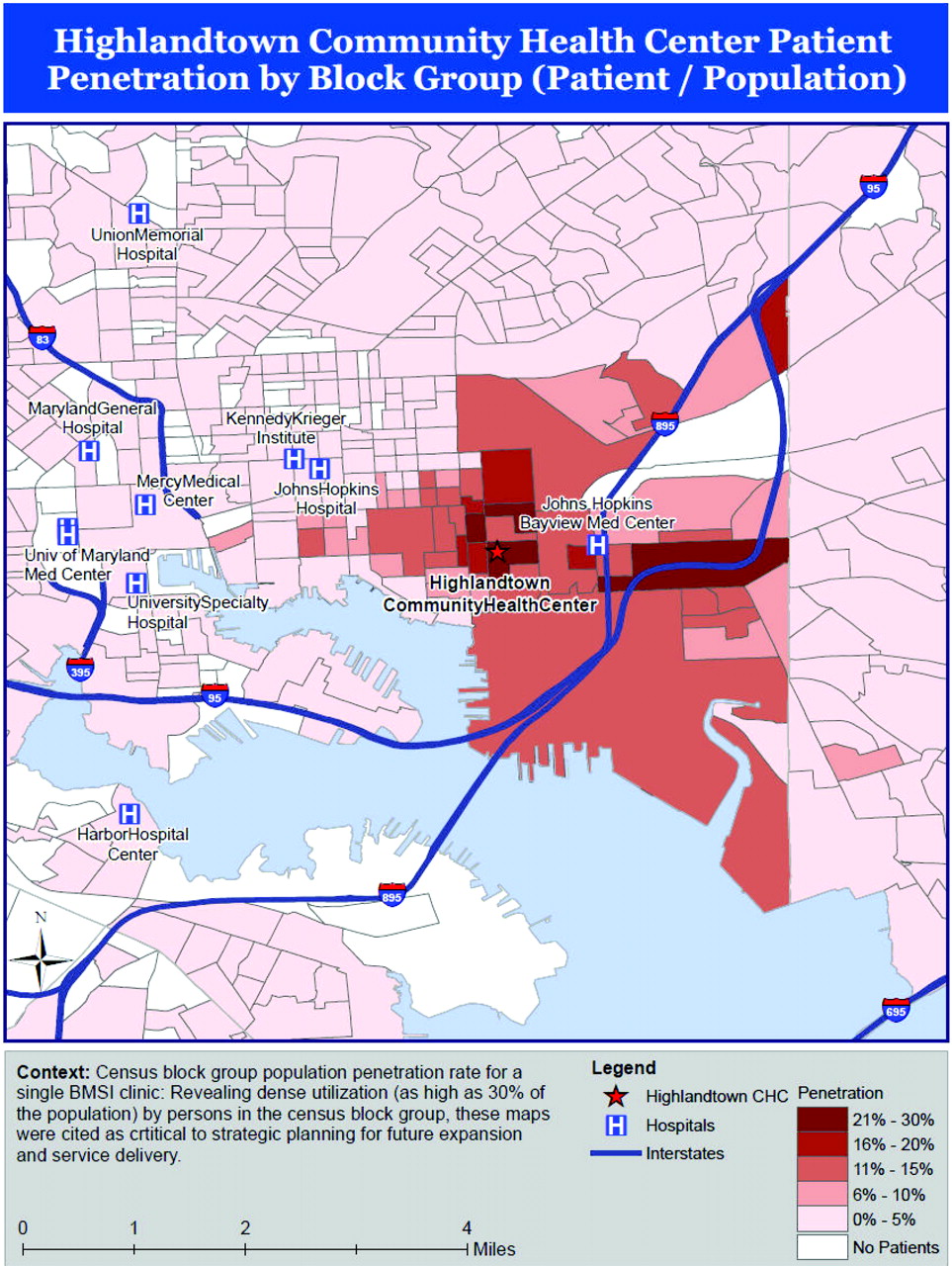
- Figure 3.
Census tract population penetration rate for a single Baltimore Medical Systems, Inc., clinic. Revealing dense utilization (as high as 30% of the population) by persons in the census tracts most proximal to this clinic, these maps were cited as critical to strategic planning for future expansion and service delivery. GIS, geographic information systems.
- Figure 4.
Perceptions, barriers, and possible solutions to increase primary care geographic information systems adoption. BMSI, Baltimore Medical System, Inc.; CHC, community health center.


Tables
- Table 1.
Key Domains Related to Primary Care Adoption of Geographic Information Systems from Community Health Center Key Informants
Key Domains Perceptions of Primary Care Clinical Applications of GIS Key Informant Comments, Responses, and Results Positive perceptions The process resulted in enthusiastic engagement “I’m just excited… We’re doing this expansion grant for [clinic A] and there [are] two key questions in the grant being asked: ‘Why do you guys think you need to expand?’ and ‘Tell us who is not being served in your MUA that you need to expand [for].’ Now I’ve got these maps. Look at all of these people in my clinic area that are not being served and we need to expand. And now I have to get some outreach persons [to explain this].” Maps enhanced community comprehension Operations committee members and one administrator were “stunned” by the fact that they were serving more than 1-in-4 people in some blocks around a clinic that was “so close to [other primary care safety net service providers].” After seeing the overlapping service areas of 3 of their clinics, 3 participants stated (verbatims intertwined): “We thought [clinic A] was losing business to [a nearby provider network]. . .not filling their pediatrics appointments. . .but it looks like their kids are going to [sister clinics B and C, also within BMSI].” Mapping galvanized new ideas about data use Gauging the impact of a proposed site move on access for vulnerable patient populations, in follow-up to the focus groups leadership of the network elected not to move a clinic because maps revealed that clusters of 2 vulnerable populations served would have their access threatened. Improving the efficiency and effectiveness of existing community health outreach and marketing activities, such as breast cancer awareness among African-American women older than 40. In follow up, this proposal led to a research project to explore this question. Merging clinic data with regional Medicaid managed-care data to guide unassigned Medicaid recipients to appropriate safety net facilities for primary care. Supporting expansion grant funding for new clinical services, both as new sites and through expansion of high utilization clinics. Assessing the success of 2 new clinics in reaching local vulnerable populations targeted in their federal grant applications. Leaders pointed out how GIS applications could improve clinical revenue. Penetration maps for one clinic generated enthusiastic discussion among clinic leaders. The maps showed that, despite a wealth of nearby safety-net options, as many as 20% to 25% of individuals from the 4 census-block groups adjacent to their clinic were using their services (see Figure 3). These maps confirmed leaders’ suspicions that they were the principal provider in a particular neighborhood and served as the impetus for pursuing grant funding to expand that clinic. Negative perceptions Participatory interpretation required Understanding any single static map was best done through discussion, and exploration of the data in a desktop GIS “on the fly.” In one focus group, a single participant's insight helped the group understand why 2 census-block groups distant from BMSI clinics had unexpectedly high user penetration: “There is a deaf community there that takes advantage of [our hearing impaired services] at [clinic A].” Barriers to further implementation Financial and technical Desktop GIS software use was seen as too expensive and technically challenging to overcome for primary care implementation, even in a large, multisite practice with substantial information technology support. Security and workflow Multiple informants noted the importance of HIPAA-compliance and data security and the need for access across multiple settings. Possible solutions Demonstrate financial impact Demonstrating usefulness in grant writing, defending contracts, and reimbursements with payors, hospitals, and community stakeholders is key to driving adoption. Achieve economies of scale through web-based platform Internet-based solutions that would allow accessibility of data able to be mapped for multiple locations—such as at the point of care—during advocacy efforts or in administrative meetings were cited as the best way to “increase the likelihood of using [clinical data mapping] regularly.” Ensure a dynamic or interactive mapping process Focus groups and individuals preferred dynamic mapping that allowed them to turn layers on and off, zoom in and out, filter data, and change data attributes to static maps. GIS, geographic information systems; MUA, medically underserved area; BMSI, Baltimore Medical System, Inc.; HIPAA, Health Insurance Portability and Accountability Act.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Examining How Social Risk Factors Are Integrated Into Clinical Settings Using Existing Data: A Scoping Review
- Novel Models to Identify Census Tracts for Hepatitis C Screening Interventions
- Clinicians Overestimation of Their Geographic Service Area
- Progress towards using community context with clinical data in primary care
- How Other Countries Use Deprivation Indices--And Why The United States Desperately Needs One
- Using Geographic Information Systems (GIS) to Identify Communities in Need of Health Insurance Outreach: An OCHIN Practice-based Research Network (PBRN) Report
- Mapping Primary Care: Putting Our Patients in Context