
Article Figures & Data
Figures
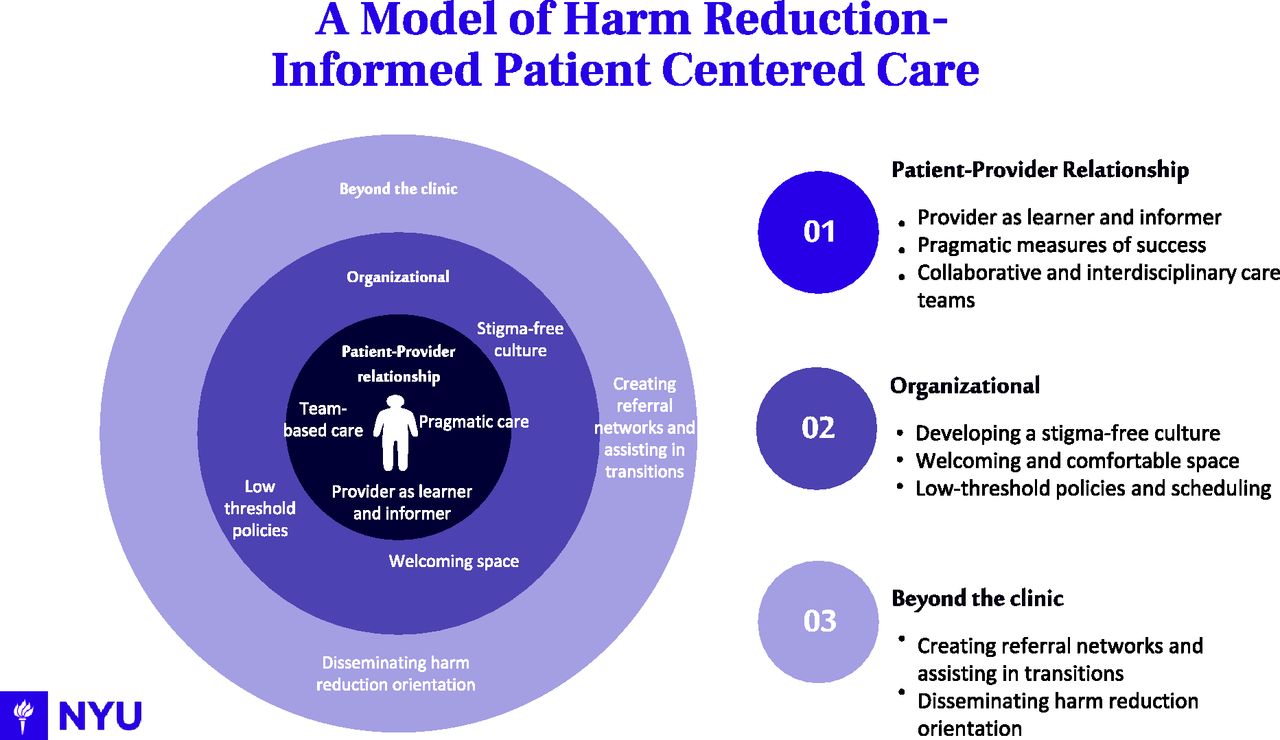
- Figure 1.
Themes of harm reduction-informed medical care by organizational level.
Tables
Site 1 Site 2 Site 3 Model Free-standing clinic model Co-located model in Hospital System Co-located model in Syringe exchange program Setting Non-Urban, Ithaca NY Urban, East Harlem NY Urban, Bronx NY Services Primary care, medication for opioid use disorder (MOUD), Human Immunodeficiency Virus (HIV) and Hepatitis C (HCV) testing, pre-exposure prophylaxis (PrEP), Mental health, social services Primary care, MOUD, risk reduction counseling, HCV treatment, overdose response training, and behavioral services Primary care, MOUD, HIV and HCV treatment, PrEP, referrals to specialty care Number of Interview Participants 7 (Director of operations, clinical supervisor/primary care provider, director of financing strategy, psychologist, physician, community health worker) 7 (Patient navigator, nurse care manager, nurse practitioner, physician, social worker, research physician (2), operations coordinator) 6 (Nurse, care coordinator, physician (2), registered nurse, project director) Themes Examples Illustrative Quote(s) Provider as both learner and informer Provider views patients as experts in their own drug use and strives to learn what patients’ goals in treatment are
“Letting the patient feel like they're autonomous in their treatment decisions is really important. I actually will tell patients, consider me a tool for your health and I will take on the doctor role and I will tell you what my advice is and my recommendations, but I don't ever want you to feel like I'm trying to tell you what to do.” Providers are not directive or forceful but function as sources of information for patients, providing a realistic range of support options to develop a treatment plan consistent with? patient’s goals.
Provider aims to be compliant to patient’s needs (not vice versa) and to help patients adopt safer behaviors.
“Harm reduction means you're giving somebody all the tools, you're informing the person, the participant. You're giving them all the tools they have to make the safest decisions, but ultimately, their decisions are their decisions” Pragmatic measures of success Providers recognize that complete abstinence may not be a realistic goal for many patients.
“I would qualify that success is that they're engaging with us, having an honest relationship with us, and are able to come to us when there are new problems coming up for them.” Focus is placed on the process of treatment rather than outcomes
Measures of success based on care processes (ie, patient engagement and retention), having an open, honest relationship with patients, and reaching patients’ self-identified goals.
“We're not expecting that people are going to be completely abstinent, that might not even be their goal and that's totally okay. But just seeing progress and being happy with that. Like, patients like coming in time to get a refill, that's great” Collaborative and interdisciplinary care teams Ensuring a wide range of providers and specialists are available to address varied patient needs
“We’re constantly talking to each other. We have weekly team meetings. We’re constantly emailing each other about the various needs of our patient. We know each other, we’re a small team and I think that makes it very easy for me to pick up the phone and call.” Routine staff meetings to collaboratively discuss issues and questions related to patient care
Relying on other team members for support during difficult situations
Developing a stigma-free culture Having strong leadership team dedicated to harm-reduction
“We create an environment where people are free to discuss their drug use without fear of being stigmatized or judged, so that we can give people the tools to reduce their harms around the health issues that arise for people who inject drugs”
“We do interview all of our clinic-facing providers, like nurses and front desk and everything. They do an interview with the team huddle. And this guy came on last week and he was like, I just really want to treat addicts and everyone’s eyes rolled. And that was the end, the guy didn’t get the job”Intentional hiring and screening practices for culture-fit
Ongoing training and education on using stigma-free language versed in trauma-informed care (ie, in charting) and treating all patients with respect
Constant communication and check-ins between staff to ensure fidelity to harm-reduction principles
Creating a comfortable and welcoming physical space Providing showers, bathroom, and laundry facilities on site
“Patients have a comfortable relationship with the clinic. Some of them, they come in, and often we're not even registering them with the doctor. They're just sitting and talking to us in the nurse’s office. We're not busy, and they can come in and talk to us.”
“Our staff works really hard at making sure that patients don't feel stigmatized, that they don't feel judged or looked upon as less than. I think physically the fact that patients can come in and grab a cup of coffee, which if you're injection drug users, the fact that you have the space to do that safely in, I think is really quite critical.”Allowing patients to bring belongings such as large bags, carts, pets in the clinic
Handing out snacks to patients to make wait times less onerous
Remembering patients’ names
Reducing paperwork burden for patients
Low-threshold care with flexible scheduling Adopting a walk-in model for appointments with no penalties for no-shows or late arrivals
“In our clinic, we have basically a policy that patients certainly need appointment times, but often they're late for their appointment times or early for their appointment times, and we'll basically see them whenever. So that just allows a lot more flexibility for them to be able to be seen.”
“We do urine toxicology tests. We try to say that very much upfront, this is not punitive, this is it just to have an open conversation. We're not trying to stop your prescription. Even if you're using opioids”No penalties or discontinued services for disclosing medication misuse
Using urine toxicology to start conversations rather than for punitive purposes
Enacting policies to protect patient privacy (i.e. to courts)
Reaching beyond the clinic to disseminate harm reduction orientation Carving out time to teach harm reduction principles in medical schools and residency training programs
“Very few current internal medicine residency programs even teach what harm reduction is, or how to provide low threshold MAT. We are involved in a training program locally to do just that.” Holding training sessions with other local community organizations
Creating robust referral networks to enhance transitions of care Developing referral networks to ensure patients are treated with respect when receiving services outside of the clinic
Supporting patients during external transitions (ie, scheduling external appointments, providing MetroCards)
“We don't send people to places where they're going to be treated poorly or abused by providers, we're not going to send them because that reflects back on us. So, we're careful about our referrals naturally.” Interview Questions Section I: Program Descriptive Information 1. Briefly describe the type of practice and the services provided
2. Briefly describe the history of the program’s integrated services
3. Briefly describe the interactions between patients and staff members
4. Briefly describe the organization of the care team
Section II: Harm Reduction Approaches and Services What do you consider to be critical elements of harm-reduction-informed care? 5. What does a harm reduction-oriented model of treatment look like in your practice?
6. How would you describe your organization’s philosophy toward patient care?
7. Could you provide me with an example of applying these philosophies to delivering care to patients?
8. How do you assess whether you are being true to these concepts?
9. What mechanisms does the practice have in place to build a culture of harm reduction?
10. Describe the decision-making process that takes place in your clinic around patient care.
11. Describe how you enact and integrate the following harm reduction concepts in your clinic:
Humanism: Providers have respect for patients and the decisions they make, providing care without moral judgments.
Pragmatism: Providers have realistic expectations and support a range of options for reducing harm.
Individualism: Support is tailored to individual patients’ needs.
Autonomy: Patients and providers negotiate the best plan of care.
Incrementalism: Any positive change acknowledged and reinforced.
Accountability: Patients are responsible for (and experience) the consequences of their behavior but are given additional chances to improve.
Section III: Facilitators and Barriers 12. What factors help facilitate the provision of harm-reduction oriented care in your practice?
13. What factors prevent the provision of harm-reduction oriented care in your practice?
14. What advice do you have for providers that want to adopt a harm-reduction-oriented approach to care integration?
Theme Free-Standing Clinic Model Co-Located Model in Syringe exchange program Co-Located Model in Hospital System Provider as both learner and informer - Providers provider a realistic range of support options
- Patient guides the provider to understanding what will be the safest course of action for them
- Patients are not required to be compliant to providers, providers are expected to be compliant to patient needs
- Providers take cues from the patient
- Providers give patients all the tools and resources to make their decisions, but accept that decisions are theirs to make
- Providers let patients know they are autonomous in their treatment decisions
- Providers create treatment plans in conjunction with the patient and in which the patient has decision-making power
- Providers understand that patients know more about drug use than the providers
Pragmatic measures of success - Providers are responsive to patient goals and do not push their own agenda
- Providers goals are to cultivate a trusting relationship with patient
- Definition of success dependent on individual patient
- Any positive change is acknowledged
- Celebrate small successes
- Patients identify needs to address, not required to be SUD-related
- Success can be patient engaging for a follow-up visit, getting stable housing, getting a job, refilling medication
- Having a relationship with the patient is a success
- Patient decides treatment goals and are not required to have abstinence as a goal
- Patient success is based on their own goals and needs
- Reality-based care focused on the process, rather than the outcome
- Communication and engagement with patient is success
Interdisciplinary and collaborative care teams - Morning meetings with clinic staff to review schedules
- Day-to-day operations are collaborative
- Every voice is valued
- Interdisciplinary care
- Weekly clinic meetings
- Interdisciplinary approach
- If needed, two providers will meet with an individual patient
- Interdisciplinary care
- Constant communication between staff
- Weekly check-ins with entire team
- Providers call each other for support in patient interactions
Developing a stigma-free culture - Careful about hiring and screening applicants
- Recognizing that the medical system is patriarchal
- Servant leadership
- Mandatory, ongoing training
- Providers do not impose the medical system on patients and uphold patients ownership and belonging in the space
- Hiring the correct people
- Ongoing and supporting training
- Provider recognition of biases and privileges
- Hiring the right providers
Creating a comfortable and welcoming physical space - Avoid use of stigmatizing language
- Do not release information to courts or criminal justice system without patient consent
- Staff remember patient names and other personal details
- Friendly signage
- Radical welcome; ‘we take you as you are’
- Patients welcome to come in and chat without seeing a provider
- Patients can bring dogs or belongings into the clinic
- Patients are not burdened with paperwork
- Give out snacks to patients
- Allow patients to use bathrooms and showers
- Avoiding use of stigmatizing language
- Social justice and racial justice initiatives
- Avoid use of labels in medical charting
- Give patients snacks
- Hand out metro cards
Low-threshold care with flexible scheduling - Patients not penalized for missed appointments
- On-demand services
- Do not withhold treatment because patient discloses drug use
- Walk-in model
- Are not punitive with positive urine toxicologies
- Do not require abstinence
- Do not refuse treatment or kick someone out because of a positive urine toxicology
- Patients not penalizing for late or missed appointments
- Same-day access to services
Reaching beyond the clinic to disseminate harm reduction orientation - Staff train local providers and community organizations on harm reduction
- Providers teach at medical schools
Creating robust referral networks to enhance transitions of care - Careful with referrals and creates ties with external providers
- Careful with referrals and creates ties with external providers
- Careful with referrals and creates ties with external providers
- When external care is necessary, staff make appointments for patients and remind them of visits
Abbreviation: SUD, Substance use disorders.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.