
Abstract
Background: Substance use disorders (SUDs) are at a national high, with significant morbidity and mortality. Harm reduction, a public-health strategy aimed at reducing the negative consequences of a risky behavior without necessarily eliminating the behavior, represents a useful approach to engage patients with SUDs in care. The objective of this article is to describe how 3 medical practices operationalized harm reduction as a framework toward patient care and identify the common practices undertaken across these settings to integrate harm reduction and medical care.
Methods: We conducted a qualitative study using in-depth, semistructured interviews with 20 staff and providers at 3 integrated harm reduction and medical care sites across New York State from March to June 2021. Interview questions focused on how harm reduction approaches were implemented, how harm reduction philosophies were demonstrated in practice, and barriers to adoption.
Results: The interviews resulted in 8 main themes of integrated harm reduction medical care: 1) role of provider as both learner and informer; 2) pragmatic measures of success; 3) collaborative and interdisciplinary care teams; 4) developing a stigma-free culture; 5) creating a comfortable and welcoming physical space; 6) low-threshold care with flexible scheduling; and; 7) reaching beyond the clinic to disseminate harm reduction orientation; and 8) creating robust referral networks to enhance transitions of care. These themes existed at the patient-provider level (#1 to 3), the organizational level (#4 to 6), and the level extending beyond the clinic (#7 to 8).
Conclusions: All 3 sites followed 8 common themes in delivering harm reduction–informed care, most of which are consistent with the broader movement toward patient-centered care. These practices demonstrate how medical providers may overcome some of the barriers imposed by the medical model and successfully integrate harm reduction as an orienting framework toward care delivery.
- Access to Primary Care
- Harm Reduction
- New York
- Opiate Substitution Treatment
- Opioid-Related Disorders
- Primary Health Care
- Qualitative Research
Introduction
Substance use disorders (SUDs) are at a national high, with significant associated morbidity and mortality. More than 100,000 overdose related deaths were reported in the year ending April 2021,1 marking a growth of more than 30% over the prior year. Amid worsening rates of overdose deaths, the Biden administration released a new Overdose Prevention Strategy that explicitly identified harm reduction (HR) as a priority, signaling an ideological shift in the national response to the opioid crisis.2
HR is a public-health strategy aimed at reducing the negative consequences of a risky health behavior without necessarily eliminating the target behavior.3 In the context of drug use, HR prioritizes the prevention or minimization of drug-related harms such as HIV transmission and overdose without requiring the elimination or reduction of drug use itself.4 Although HR strategies have been supported by grassroots efforts for decades, they remained controversial in the United States, where the “War on Drugs” model predominated since the 1970s. Although states such as New York have already instituted guidelines that encourage an “HR approach in the care of all individuals who use substances,” the Biden administration’s new strategy is the first endorsement of HR as a policy at the federal level.5
This recent shift comes amid growing consensus on the importance of integrating HR concepts and services into the traditional substance use treatment milieu.6 A 2020 Consensus Report by the National Academies of Sciences, Engineering, and Medicine noted that “harm reduction strategies are essential to decrease the risk of infectious disease” and recommended that “individual clinics, health care programs, and providers should incorporate harm reduction strategies into both infectious disease and opioid use disorder care.”7 Similarly, in a 2022 National Academies of Medicine consensus report, experts called for an “integration of harm reduction into broader health systems.”8 These actions point toward a broader momentum to integrate HR principles and practices in the routine provision of care for patients who use drugs.9
Yet, despite growing support, little is known around what HR looks like in medical settings. Although HR includes pragmatic activities such as distributing naloxone and educating patients about safe drug use practices, it also necessitates a shift in the philosophy toward patient care.10 HR involves the adoption of a treatment perspective that meet patients “where they are at” in terms of their drug use, even if it entails continued drug use.11,12,13,14,15 In allowing the person who uses drugs to set their own goals, HR shifts the locus of control from the physician and his/her medical knowledge to the patient. These philosophical clashes may act as an invisible barrier to integrating HR into broader medical models.10
HR has been widely practiced as an orienting philosophy in syringe service programs and other community-based settings, and several studies have examined the incorporation of specific HR activities such as syringe exchange and supervised injection sites into medical treatment models.16,17,18,19,20,21 Other studies have examined the adoption of certain practices such as the delivery of low-threshold and patient-centered HIV and SUD treatment.22,23,24 However, very few detailed examples exist on how HR and medical practices can be integrated, and how successful providers operationalize this integration.25
This qualitative study uses semistructured interviews of providers and staff at integrated HR-medical care sites to synthesize the common themes and characteristics across sites and to introduce a useful overarching model of HR-informed medical care.26 Given the high prevalence of SUDs among patients in primary care practices,27 it is important to understand how HR can be implemented in This study specifically interviewed providers and staff at 3 treatment sites that have adopted a harm reduction medical model, and their approaches could give insight and direction to more traditional practices in the process of moving from a treatment focused-model to a harm reduction orientation.
Methods
Study Design, Setting, and Participants
This qualitative study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) reporting guidelines.28 The research team conducted in-depth interviews with 20 staff and providers at 3 sites across NYS. The research team consisted of 3 university researchers (JC, ZL, HH) who study health disparities and health care delivery for people who use drugs (PWUD). The researchers’ prior beliefs included supporting medication treatment and harm reduction services as evidence-based practices that promote health equity.
Sites were selected based on our understanding of their explicit adoption of HR in its mission; specifically, 2 sites were identified by the National Academies of Medicine as exemplar sites that have adopted harm reduction, and the third site was recommended by the other 2 practices. The sites are described in Table 1.
Description of Sites
The research team created a semistructured interview guide that focused on how HR approaches were implemented at each site, how HR philosophies were demonstrated in practice, and barriers to adoption. The interview guide can be found in Appendix Table 1. Participants were recruited based on discussions with leadership from each site; specifically, participants were selected to represent the spectrum of roles that exist within each site, including those that exist in direct patient care (primary care providers, psychologists, patient navigators, care coordinators, social workers, community health workers, nurses, nurse managers, registered nurses, and nurse practitioners) and those that are involved in establishing clinic policies and in practice administration (medical directors, directors of operations, directors of finance, project directors, and operations coordinators). All interview participants identified by the leadership from each site agreed to participate in the study. Participants were given $50 gift cards for the interviews. Each interview was conducted by 2 interviewers using video or audio calls and were professionally transcribed. Interviews were conducted from March- June 2021, and approval for this study was obtained from the New York University Institutional Review Board.
We took a 3-step approach to analyzing the data. After verbatim transcription of the interviews, we first organized responses based on interview question category (ie, defining harm reduction philosophies, barriers, facilitators to adoption). In the second step, the primary analyst (Z.L.) openly coded each segment of the text following a constructive grounded theory methodology. Grounded theory is a widely used inductive approach to qualitative data analysis aimed at the discovery of theory from systematically obtained data.29,30 A grounded theory approach is particularly well suited for conceptual framework building due to its emphasis on generalizing theorization.26 Constructive grounded theory is a relativist and pragmatic version of grounded theory, which does not assume that theories are discovered as in classic grounded theory, but are constructed by the researcher within a particular cultural and personal context.31 In the final step, all authors (Z.L., H.H., J.C.) reviewed coding notes across regular meetings to develop theoretical codes or “themes” based on the patterns and relationships found between the codes.
The main analyst (Z.L.) outlined the main points for each theme within the matrix along with illustrative quotes from interviews for each theme.
Results
The 8 themes of integrated HR medical care were: 1) role of provider as both learner and informer; 2) pragmatic measures of success; 3) collaborative and interdisciplinary care teams; 4) developing a stigma-free culture; 5) creating a comfortable and welcoming physical space; 6) low-threshold policies; 7) reaching beyond the clinic to disseminate harm reduction orientation; and 8) creating robust referral networks to enhance transitions of care. (See Table 2 for examples and illustrative quotes and Appendix Table 2 for the themes of harm reduction-informed care by site.)
Common Themes of Harm Reduction-Informed Care
These 8 themes were categorized into 3 groups, based on the organizational level (micro, meso, macro) in which the themes operated: 1) the patient-provider relationship (themes #1 to 3); 2) organizational (themes #4 to 6); and 3) beyond the clinic (themes #7 to 8). See Figure 1 for the full model displaying the 8 themes of HR oriented care organized by organizational level.
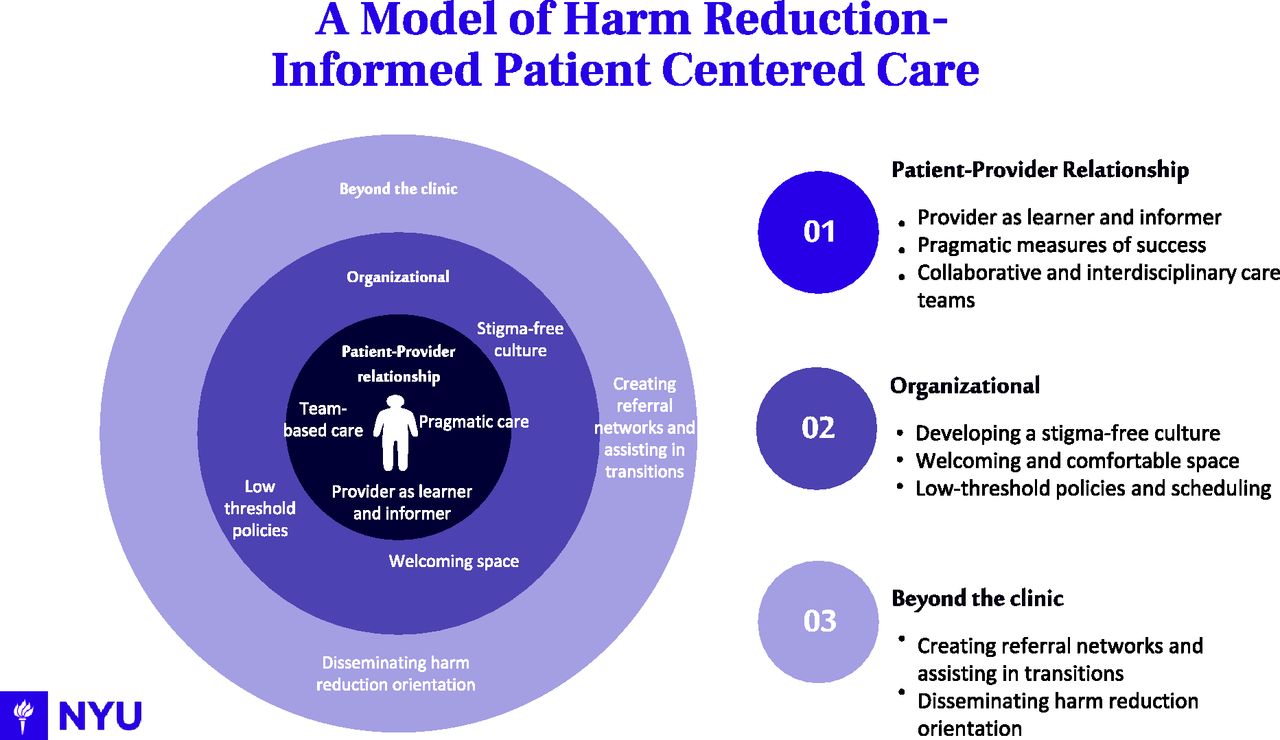
Themes of harm reduction-informed medical care by organizational level.
HR within the Patient-Provider Relationship
Role of Provider as Both Learner and Informer
Respondents discussed the unique role of providers within the HR context, which is to both learn from patients and inform them of potential options to improve their health and well-being. Rather than viewing providers as the authority on health, participants were clear that the patient is the expert in their own drug use. Therefore, the patient, not the provider, drives the conversation and identifies their own health priorities, which need not include addressing substance use.
In developing a treatment plan for the patient’s self-identified priorities, providers are not directive or forceful, but function as sources of information and guidance, and provide a realistic range of support options aimed at improving patients’ lives. Providers have a responsibility to provide patients with medical advice but must respect and acknowledge a patient’s autonomy to make their own decisions with the resources provided. The expectation is not that the patient must be compliant to the treatment, but for the provider to be compliant to the patient’s needs, and help patients practice safer behaviors.
Pragmatic Measures of Success
Respondents noted the importance of having a pragmatic understanding of what constitutes success in the context of a patient’s treatment. Providers recognized that substance use may continue, and that complete abstinence was not a realistic goal for many patients. Instead, the focus is on the process of treatment, rather than the outcome. Process-related successes included patient engagement in visits, patient retention, and having an open and honest relationship with patients.
Providers were also firm in their belief that the definition of patient success varies according to the person. For many providers, addressing a patient’s self-identified goals is considered an achievement, with 1 provider noting that in some cases simply identifying the patient’s priority is an accomplishment. Providers also agreed that any positive change or risk reduction should be acknowledged and considered a success, and that providing holistic support to patients, and addressing social determinants of health such as homelessness were important elements of a successful visit.
Collaborative and Interdisciplinary Care Teams
Respondent sites discussed the importance of employing interdisciplinary care teams to meet patient needs. At each clinic, the day-to-day operations are collaborative, and it is not uncommon for a small team of staff members to meet with an individual patient. In addition, should one clinician be overburdened or have a full schedule, other team members will step in and adapt their schedules to incorporate more patients. Staff at all 3 sites are in constant communication with each other about patient care and feel comfortable calling on other team members for support in difficult situations. Each site also holds weekly meetings to discuss any issues or questions related to patient care.
Care at each site is also interdisciplinary, with a wide range of providers and specialists working to meet the varied needs of patients with co-occurring mental and physical health issues. For example, staff at 1 clinic included primary care providers, a community health worker, social workers, peer navigators, a psychologist, and a psychiatric nurse practitioner, thus providing more specialized services to address patients’ unique needs.
HR at the Organizational Level
Developing a Stigma-Free Culture
To practice HR-informed care, respondents stressed the importance of developing a stigma-free culture that is respectful, trusting, and understanding of patients. Key to this culture was having a strong leadership team dedicated to the mission of providing HR -informed care and hiring clinical providers and staff who are willing to learn about and apply HR to their work.
Providers and staff also stressed the importance of having initial and ongoing training and education on HR principles and using stigma-free language rooted in trauma-informed care. This entailed having constant communication and check-ins with other staff members to ensure fidelity to HR principles during day-to-day interactions with clients. These practices helped create a culture in which providers and staff are comfortable assessing each other, and where team members are encouraged to ask for help and support.
Creating a Welcoming and Comfortable Physical Space
Respondents also emphasized the need to create a physical space that was comfortable and welcoming to patients, and in which patients did not feel stigmatized, judged, or perceived as ‘less than.’ This could be achieved by remembering patient’s names as they walked in the door, ensuring signage around the clinic was not stigmatizing toward drug users, handing out snacks and warm drinks to help make wait times less onerous, and allowing patients to bring belonging such as large bags, carts, or even pets into the clinic. One clinic provided spaces for showers and laundry facilities on site.
Low-Threshold Care with Flexible Scheduling
Low-threshold and flexible policies is another core component of HR-informed care at all 3 sites, with the goal of removing barriers put in place by the health care system, and meeting patient needs. Staff and providers from each site discussed the importance of having a walk-in model for appointments rather than scheduled appointment times, and not disciplining patients for missing appointments. Although 2 sites accepted appointments, they did not penalize patients who were late. Common to all sites were nonpunitive, nonjudgmental policies regarding urine toxicology screenings; when performed, the results of these screenings were used as a starting point to begin conversations with patients surrounding safer drug use such as to counsel about the risks of polydrug use. In addition, patients are not punished nor are their medications discontinued for disclosing medication misuse while on buprenorphine. Finally, staff emphasized their strict policy of not releasing information to courts or the criminal justice system without express permission from patients.
HR as an Approach Extending beyond the Clinic
Reaching beyond the Clinic to Dissemination Harm Reduction Orientation
Respondents discussed the importance of reaching beyond the clinic to disseminate practices and elements of a harm reduction orientation to other clinics and providers, as well as to shift perceptions of people who use drugs (PWUD). Providers from 2 sites taught at medical schools and in residency training programs and used these roles as opportunities to infuse HR philosophy into the next generation of providers. This includes both the principle that care does not end in the clinic, and the importance of recognizing patients with SUDs as autonomous in the treatment process.
Creating Robust Referral Networks to Enhance Transitions of Care
Respondents across all 3 sites also made active effort to create referral networks to ensure patients are sent to practices where they will be treated with respect and to coordinate care with other providers. At times, this entailed sending patients to a provider outside of a particular health system or network. In addition, staff at each site strive to make the transition as smooth as possible, by making external appointments for patients, reminding patients of appointments, and in the case of 1 site, hiring peer navigators to escort patients to external appointments and providing them with MetroCards.
Discussion
In this study, we describe a model of integrated HR and medical care based on 8 common themes across 3 medical treatment sites that adopted HR as an orienting philosophy toward patient care. This model operates at 3 levels. At the patient-provider relationship level, HR entails shifting the provider’s role to that of a learner and informer, setting pragmatic goals, and delivering team-based care. At the organizational level, this model emphasizes the importance of a stigma-free culture with welcoming physical space and low-threshold policies. Beyond the clinic, the model emphasizes disseminating a harm reduction orientation to other clinics, the creation of referral networks, and other activities to assist in care transitions (see Figure 1).
The Institute of Medicine (IOM) defines patient care as “providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions,”32 and endorses 6 dimensions of patient care33: 1) respect for patients’ values, preferences, and expressed needs; 2) coordinated and integrated care; 3) provision of information, communication, and education; 4) ensuring physical comfort; 5) provision of emotional support; and 6) involvement of family and friends. The model of HR-informed care that emerged from our study aligns directly with these dimensions of patient-centered care. For example, low-threshold, pragmatic care in which patients drive their care goals directly address the IOM’s emphasis on being respectful to patient’s values, preferences, and needs. Similarly, in providing interdisciplinary and collaborative care, and reaching beyond the clinic to develop referral networks of like-minded providers, the sites in our study delivered coordinated and integrated care. Providers interviewed in our study also viewed their roles as sources of information for patients in providing a realistic range of support options, which aligns with the IOM’s third principle of patient centered care. Creating a comfortable and welcoming physical space helps ensure physical comfort for their patients. Finally, in developing a stigma-free-culture and training providers in using stigma-free language rooted in trauma-informed care, HR-informed care can relieve fear and anxiety among a highly stigmatized population.
Mistrust between PWUD and medical providers have persisted amid a growing overdose crisis. Prior research suggests many providers fear being deceived by PWUD and express discomfort and uncertainty in their approach to these patients.34 Meanwhile, PWUD experience stigma and often interpret clinician interactions as signs of intentional mistreatment.28,35 The overlapping experience of fear, stigma, and mutual mistrust creates conditions that make it challenging to deliver patient-centered care.29,36 Although some aspects of the HR-informed patient-centered care model, such as open-access scheduling may be challenging to implement in many office-based settings,37 strategies such as working with the patient to set pragmatic treatment goals and creating a culture of acceptance and respect could serve as a starting point to help dismantle pervasive mistrust between PWUD and the medical and nursing community.
There are several limitations to our study. First, sites were selected to participate in this study based on their known experience practicing a HR-approach to care and their experiences may not translate to providers who practice in more traditional medical settings. As noted earlier, some aspects of HR model, such as open and flexible scheduling, may not be feasible in many contexts and may require an unconventional approach to organizing the workload. Second, this study only captured the perspectives of providers and staff and did not include the perspective of patients. Third, this study focused solely on primary care sites, and did not include specialty care or hospital-based settings. Future studies should explore ways to design HR-informed patient-centered care from the client’s perspective, as well as adapt elements of this approach, including low-threshold buprenorphine prescribing, having a stigma-free culture, and a referral network that includes HR-oriented providers and warm handoffs, to a wider variety of care settings, beyond primary care.
Yet, despite these limitations, our study adds to the growing literature on the integration of HR practices and philosophies into medical settings. According to the National Survey on Drug Use and Health only 10.3% of individuals with a SUD received treatment in 2019.38 Many people who need substance use treatment do not receive it because they are not ready to stop using drugs.13 Moreover, mutual mistrust between PWUD and medical providers pose a significant barrier to access.28,39 For these individuals, HR may serve as an important entry point to engagement in treatment. A large body of evidence has accrued over decades demonstrating the programs like SSPs that were built on HR principles have had wide reaching positive impacts, including reducing overdoses and overdose deaths, transmission of communicable diseases, and substance-using behavior overall.40,41,42 However, very few examples of an integrated HR-medical models exist in the literature.13 Other articles have proposed HR frameworks specifically for the delivery of buprenorphine in primary care settings,25 offered guidelines for the integration of specific harm reduction services, such as syringe exchange services or supervised injection, into health care settings such as hospitals,43,44,45 and proposed principles to define harm reduction as a conceptual approach to health care delivery.3 However, these articles fall short of offering a model that operationalizes HR-orientation for medical settings at different organizational levels.
To our knowledge, ours is the first multi-site study examining how HR and medical care can be integrated. The 3 sites in our study illustrated the ways in HR can serve as an orienting framework toward delivering patient-centered medical care. Future studies should focus on developing measures of “HR-orientation” to further build the evidence base on the impact of HR as an approach toward patient care, and to assess the effectiveness of HR programs by comparing patient outcomes in sites with a strong HR orientation, compared with those lacking or with limited HR orientation. Further research is also needed to evaluate the adoption of the practices identified in a wider range of medical settings, examine which aspects of HR-informed care can be integrated more widely, and to assess whether this model is responsive to patient concerns, improves patient outcomes, and addresses the concerns of community stakeholders.
Conclusions
This study describes 3 unique sites which use HR as a framework for patient-centered care in medical settings and identifies 8 core themes underlying this approach. This innovative treatment model addresses common barriers within the health care system for PWUD related to stigma, lack of alignment with patient needs and goals, and provider misconceptions surrounding substance use. As the health care system attempts to grapple with the increased severity of the opioid epidemic, the integrated HR model presented in this study may be a useful as a guiding framework to delivering patient-centered-care for patients with SUDs.
Appendix
Standard Interview Guide
Themes of Harm Reduction-Informed Care by Clinic
Notes
This article was externally peer reviewed.
Funding: This study was funded by a grant from the Center for Drug Use and HIV/HCV Research.
Conflicts of interest: None.
To see this article online, please go to: http://jabfm.org/content/36/3/449.full.
- Received for publication September 5, 2022.
- Revision received November 4, 2022.
- Revision received November 29, 2022.
- Revision received January 23, 2023.
- Accepted for publication February 6, 2023.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.