
Abstract
Introduction: The COVID-19 pandemic caused potentially disruptive shocks to chronic condition care. We examined how diabetes medication adherence, related hospitalizations, and primary care use changed in high-risk veterans prepandemic and postpandemic.
Methods: We conducted longitudinal analyses on a cohort of high-risk diabetes patients in the Veterans Affairs (VA) health care system. Primary care visits by modality, medication adherence, and VA acute hospitalizations and emergency department (ED) visits were measured. We also estimated differences for subgroups of patients by race/ethnicity, age, and rural/urban location.
Results: Patients were 95% male with mean age 68 years. Prepandemic patients received a mean per quarter of 1.5 in-person primary care visits and 1.3 virtual visits, 0.10 hospitalizations, and 0.22 ED visits, with mean adherence of 0.82. The early pandemic was associated with fewer in-person primary care visits, more virtual visits, fewer hospitalizations and ED visits per patient, and no change in adherence; there were no midpandemic versus prepandemic differences in hospitalizations or adherence. Black and nonelderly patients had lower adherence during the pandemic.
Conclusion: Adherence to diabetes medications and primary care use remained high for most patients even though virtual care replaced in-person care. Black and nonelderly patients may require additional intervention to address lower adherence.
Introduction
More than half of US adults have a chronic condition such as diabetes, hypertension, or hyperlipidemia1 that is mainly managed in a primary care setting. Regular care including taking medications and monitoring clinical measures is critical to managing these conditions. The COVID-19 pandemic led to pauses in many in-person services that could be particularly disruptive to health care and medication access for patients with chronic conditions. Challenges to accessing health care may have been compounded by issues directly caused by the pandemic such as unemployment and the loss of income; avoidance of in-person care due to fear of COVID-19 exposure; and deteriorating mental health due to the health, economic, and social toll of the pandemic.
Most (64%) patients in the Veterans Affairs (VA) health care system have chronic conditions2 and thus were at risk for health impacts from COVID-19 disruptions to their care. The VA issued a national directive to convert most in-person services to virtual (telephone or video) care effective March 15, 2020, representing an abrupt transformation in care delivery.3⇓–5 In addition, some primary care providers and staff were diverted to other departments such as inpatient care, emergency care, or community living centers as part of VA medical centers’ emergency response to handling COVID-19 cases, potentially reducing availability of routine primary care visits. This provides the opportunity to examine whether patients with chronic conditions continued to engage with their primary care providers virtually and whether receipt of key chronic condition care was disrupted by these changes. The VA’s policy to quickly shift to virtual care mirrors that of many other US health care systems during the COVID pandemic.6,7 In addition, the Centers for Medicare and Medicaid Services began postpandemic waivers to allow US providers to be reimbursed similarly for virtual and in-person visits. Therefore, lessons learned from the VA experience with virtual care rollout can directly inform interpretation of overall US quality trends observed postpandemic and future planning to mitigate negative impacts of increased virtual care use for all patients with chronic health conditions.
We estimated changes in use of primary care and adherence to diabetes medications in our primary analysis, and hospitalizations and emergency department (ED) visits in secondary analysis, to examine disruptions in care for high-risk VA patients with diabetes over a 3-year period before and after the pandemic began. We focused on patients at high risk for hospitalization or death since we expect delayed or disrupted care to have a disproportionately larger impact on these patients. We also examined care for subpopulations of racial/ethnic minority groups, older adults, and rural residents who may have experienced greater barriers to engaging in virtual care during the pandemic.
Methods
Study Design and Cohort
We conducted a longitudinal study following a cohort of high-risk patients with diabetes over a 3-year period: fiscal year (FY) 2019 to 2021 (October 1, 2018–September 30, 2021). Patients were identified as high risk using the VA Care Assessment Needs (CAN) predictive score. Patients with a score in the 85th percentile and above for 90-day hospitalization or death in the last quarter of the baseline year (FY2019) were included.8 Patients with CAN scores in the 85th percentile have approximately 4 times the rate of hospitalizations and 7 times the rate of death as patients at the median CAN score. We limited the cohort to those with at least 1 VA primary care visit, a diagnosis of diabetes recorded in encounter records, and 1 filled prescription for an oral diabetes medication in the baseline year (FY2019).
We obtained patients’ VA health care use data, outpatient prescription fill records for diabetes medications, and mortality data from national VA administrative data in the Corporate Data Warehouse (CDW). For veterans who died during the study period, date of death was obtained from the VA Vital Status file and the CDW Patient file. This work was conducted for quality improvement purposes under the VA Office of Primary Care, so no institutional review board approval was obtained. Funding for this work was provided by the VA Office of Primary Care, and the funder had no role in the study design, analysis of data, interpretation of findings, writing of this work, or decision to submit this work for publication.
Patient Outcome Measures
Our primary outcomes of disrupted, routine care were primary care use and medication adherence. Primary care use was categorized by care modality as in-person care or virtual care including telephone, video telehealth (both home- and clinic-based services), and secure messaging based on prior work.5,9 We measured the number of visits by modality per patient.
Medication adherence for diabetes medications was measured using the proportion of days covered10 from the CDW Outpatient Prescription files.11 Drug classes included α-glucosidase, biguanides, dipeptidyl-peptidase-4 inhibitors, glucagon-like peptide-1 agonist, meglitinides, sodium-glucose cotransporter-2 inhibitors, sulfonylureas, and thiazolidinediones. We did not include insulin due to inaccuracies in measuring adherence of injectable medications via fill data. For prescription fills that crossed quarters, the number of days filled was prorated between quarters. The first quarter of FY2019 was the index quarter to identify patients’ first prescription fill, so it was excluded from the quarterly adherence measure. We identified patients who discontinued their medications with no refills recorded for 2 consecutive quarters for a drug class.
Our secondary outcomes included measures of acute medical/surgical hospitalizations, hospitalizations for an ambulatory care-sensitive condition (ACSC), and diabetes-related hospitalizations (including diabetes short-term complications, diabetes long-term complications, or uncontrolled diabetes) based on diagnosis codes from the Agency for Healthcare Research and Quality’s Clinical Classifications Software.12 We also measured all-cause ED visits.
Other Study Measures
Patient characteristics including age, gender, race/ethnicity, marital status, VA enrollment priority, Elixhauser comorbidity,13 rurality, and distance to VA primary care were measured, as in prior work, in the baseline year.11 Age, gender, race/ethnicity, marital status, and enrollment priority were obtained from the VA Observational Medical Outcomes Partnership data, which aggregates data from several VA data sources and reports standard values. Patients’ race and ethnicity was primarily patient reported but could also be reported by proxy or by VA enrollment staff. Patients’ distance to their nearest VA primary care provider and rural/urban location were obtained from VA Planning and Support Services Group data. We measured several clinic characteristics in the baseline year that could affect primary care use including mean waiting times for appointments for established patients, overall proportion of visits provided by telephone, and proportion of patients using telehealth services from clinic data in the Veterans’ Support Services Center. We measured patients’ county rate of COVID-19 infections by quarter based on the case rate reported by the Centers for Disease Control.14
Statistical Methods
We categorized FY quarters into the prepandemic (10/1/2019–3/30/2020), early pandemic (4/1/2020–12/31/2020), and midpandemic (1/1/2021–9/30/2021) phases based on the initial pause of in-person VA services (beginning mid-March 2020) for the initiation of the early pandemic phase and the widespread administration of the COVID-19 vaccine to high-risk veterans in early 2021 for the midpandemic phase. We compared patients’ unadjusted primary care use, hospitalizations and ED visits, and medication adherence in each quarter and pandemic phase over the 3-year period using descriptive analyses.
In time-series analyses, we compared outcomes in each phase relative to the prepandemic phase using an unbalanced cohort since some patients died during the study period. In estimating adherence, we excluded observations of patients once they discontinued their medications. We conducted separate regressions to estimate primary care visits by modality and medication adherence for all diabetes medications in linear models; all-cause hospitalizations, ACSC hospitalizations, and ED visits in Poisson models; and hospitalization for diabetes complications in logistic models. Models adjusted for a continuous quarterly time trend, patients’ sociodemographic characteristics (age, race/ethnicity, gender, marital status, VA enrollment priority group), Elixhauser comorbidity, comorbid depression, distance to nearest VA primary care site, rurality, all clinic characteristics standardized to the mean, community rate of COVID-19 infections, and a patient random effect, whereas standard errors were adjusted for clustering by clinic. We estimated the marginal difference in outcomes with 95% CIs in the early and midpandemic phase relative to the prepandemic phase.
We also conducted subgroup analyses to examine changes in outcomes between pandemic phases by patients’ race/ethnicity, age group, and rurality in regression models with the same covariates as above in addition to interaction terms between the subgroup characteristic with pandemic phase. We estimated the marginal means of outcomes and 95% CIs by subgroup characteristic and pandemic phase. Regression models estimating hospitalizations for subgroup analyses used linear models because marginal means could not be estimated in Poisson/logistic models. All analyses were conducted in Stata 14.
Results
A total of 188,569 patients were identified as high risk for hospitalization and death and filled medications for diabetes in the prepandemic, baseline year. Over the 3-year period, 18% of patients died. Most of the cohort (68%) was older than 65 years of age in the baseline year, the vast majority (95%) were male, and 65% were White (Table 1). Only half were currently married, most had a service-connected disability, and a majority lived in urban areas with a mean 21-minute drive time to a VA primary care site. Cohort patients had a mean of 6.4 Elixhauser comorbid conditions, with most patients having hypertension (94%) and hyperlipidemia (83%), and 38% had depression. The most common oral medications filled were biguanides (45%) and sulfonylureas (32%). Across the 930 primary care clinics treating cohort patients, the waiting time for next available appointments was a mean of 4.3 days, and 27% of clinic visits, on average, were provided by telephone and 17% of patients in a clinic, on average, had telehealth use in the baseline year before the pandemic.
Patient and Clinic Characteristics for High-Risk VA Patients with Diabetes, Fiscal Year 2019
Unadjusted Outcomes
Mean in-person primary care visits/quarter dropped from 1.5 (±2.1) in the prepandemic period to 0.7 (±1.8) in the early pandemic phase, then increased to 1.2 (±2.0) in the midpandemic phase (Table 2). Mean virtual primary care visits/quarter increased from 1.3 (±2.0) in the prepandemic period to 2.0 (±2.7) and 1.6 (±2.3) in the early and midpandemic phases, respectively. Mean medication adherence was relatively unchanged before the pandemic (0.82 ± 0.25) and during the pandemic phases (0.81 ± 0.27 and 0.82 ± 0.26, respectively). Mean ED visits, all-cause hospitalizations, hospitalizations for an ACSC, and hospitalizations for diabetes complications all dropped from the prepandemic to early pandemic phase. Mean use rose in the midpandemic phase for all acute care measures.
Mean Unadjusted VA Use by Pandemic Phase in High-Risk VA Patients with Diabetes, FY2019-2021, n = 188,569
Adjusted Outcomes
In adjusted models for our primary outcomes, we found a mean decrease of 0.68 (–0.70, –0.66) in in-person primary care visits, a mean increase of 0.88 (0.84, 0.92) in virtual primary care visits per patient/quarter, and no change in mean adherence to diabetes medications in the early pandemic phase relative to the prepandemic period (Table 3). For our secondary outcomes, we found mean decreases of 0.23 (–0.28, –0.19) in all-cause hospitalizations, 0.26 (–0.32, –0.20) in ACSC hospitalizations, 0.002 (–0.002, –0.001) in diabetes-related hospitalizations, and 0.22 (–0.24, –0.21) in ED visits per patient/quarter in the early pandemic phase compared with the prepandemic phase.
Adjusted Differences in Use During Early and Midpandemic Phases Compared to Prepandemic Phase Among High-Risk VA Patients with Diabetes, n = 188,569
In the midpandemic phase, there were increased mean in-person primary care visits and virtual primary care visits per patient/quarter relative to the prepandemic phase. There was no difference in any of the acute care measures or medication adherence in the midpandemic phase relative to the prepandemic phase. Full regression results are reported in Appendix 1.
Subgroup Summary
In models with interaction terms between race/ethnicity subgroups and pandemic phase, Black (–0.04 [–0.07, –0.02]) and Hispanic (–0.19 [–0.28, –0.10]) patients had larger decreases in in-person primary care and larger increases in virtual primary care than White patients (0.09 [0.04, 0.13] and 0.37 [0.18, 0.55], respectively) in the early pandemic phase (Figure 1A). Black patients had lower mean diabetes medication adherence throughout the 3-year period (–0.051 [–0.054, –0.048]) and also had a significant drop in adherence after the pandemic began compared with White patients (–0.005 [–0.008, –0.002], Figure 1B). Black patients had a higher rate of hospitalizations for ACSCs and diabetes complications compared with White patients in the prepandemic phase and a larger decrease in the pandemic phases (Appendix 2). Black and Hispanic patients had higher mean ED visits than White patients prepandemic and larger decreases in ED visits in the early pandemic phase.
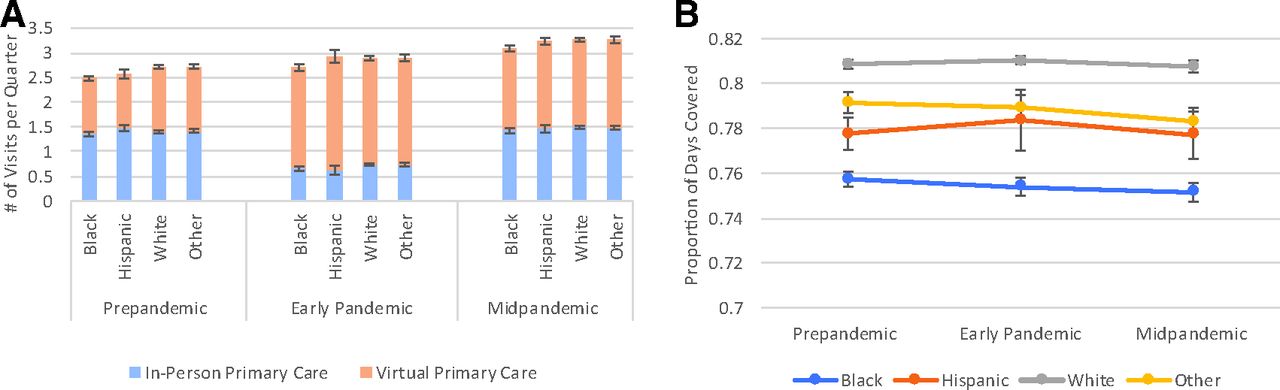
Mean adjusted primary care visits (A) and medication adherence (B) in high-risk patients by race/ethnicity. In A, blue/orange bars show mean number of primary care visits per patient per quarter estimated from regression models. In B, adherence was measured by proportion of days covered, ranging from 0 to 1.0, per patient per quarter and estimated from regression models. Mean visits and adherence per quarter were estimated from linear regression models adjusting for age-group and pandemic phase and their interaction terms, quarter, patients’ sociodemographic characteristics, Elixhauser comorbidity, comorbid depression, distance to primary care site, rurality, clinic factors, and community rate of COVID infections.
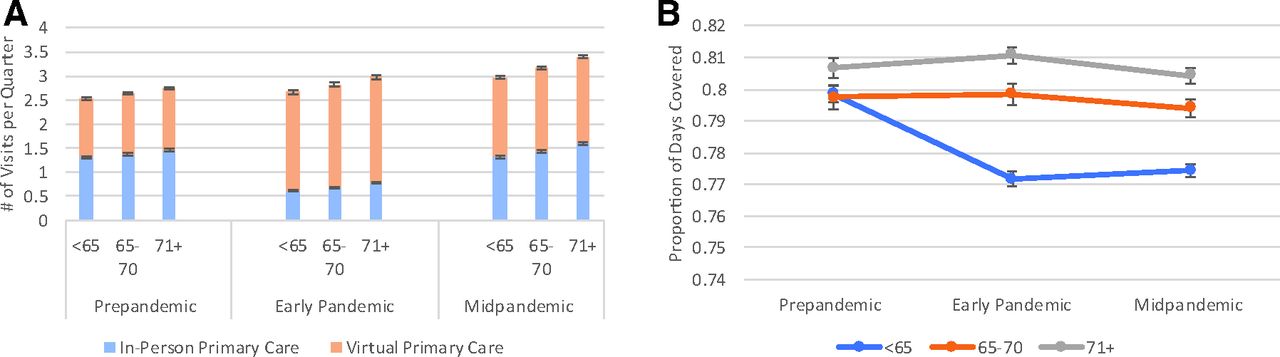
Patients in older age groups, both 65 to 70 years (0.06 [0.04, 0.08]) and 71 years and older (0.13 [0.10, 0.15]), had a larger increase in in-person primary care compared with those less than 65 years of age in the midpandemic period (Figure 2A). Older age groups also had a larger increase in virtual primary care in both pandemic periods compared with younger patients. There was an increase in adherence rate in the early pandemic period for patients ages 65 to 70 and 71 years and older (0.005 [0.002, 0.008] and 0.008 [0.005, 0.10], respectively) compared with age less than 65 (Figure 2B). The older age groups had lower rates of all types of acute care use and smaller decreases for some acute care measures compared with patients less than 65 after the pandemic began.
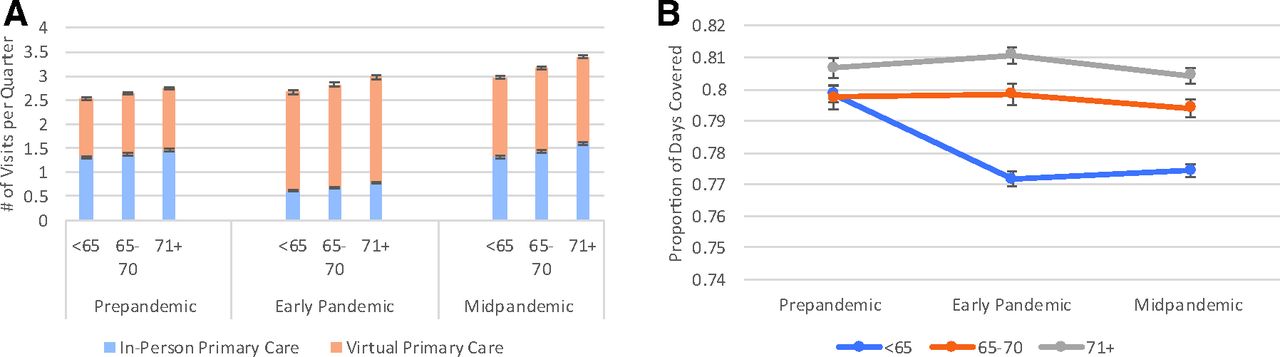
Mean adjusted primary care visits (A) and medication adherence (B) in high-risk patients by age group. In A, blue/orange bars show mean number of primary care visits per patient per quarter estimated from regression models. In B, adherence was measured by proportion of days covered, ranging from 0 to 1.0, per patient per quarter and estimated from regression models. Mean visits and adherence per quarter were estimated from linear regression models adjusting for age-group and pandemic phase and their interaction terms, quarter, patients’ sociodemographic characteristics, Elixhauser comorbidity, comorbid depression, distance to primary care site, rurality, clinic factors, and community rate of COVID infections.
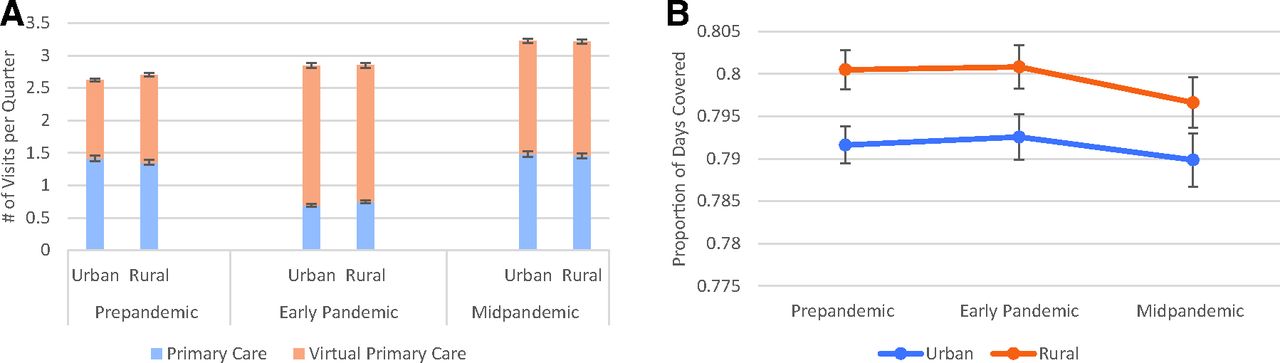
Comparing rural and urban patients, rural patients had greater in-person care (0.11 [0.09, 0.14]) and less virtual primary care (–0.19 [–0.24, −0.14]) than urban patients during the early pandemic phase (Appendix 3). There were no changes in adherence between the prepandemic and postpandemic periods for rural versus urban patients. Rural patients had less acute care use compared with urban patients, and their rate of ED visits decreased less in the early pandemic period compared with urban patients.
Discussion
In a cohort of patients with diabetes at high risk for hospitalization and death, we found temporary reductions in patients’ use of in-person primary care, ED, and hospitalizations in the early pandemic period, but most of these differences disappeared later in the pandemic. Patients’ in-person primary care use was largely replaced by virtual visits, which remained higher later in the pandemic even as in-person visits returned to prepandemic levels. Despite changes in primary care modality, adherence to diabetes medications remained high throughout the 3-year period. These findings suggest that primary care clinics were largely successful in maintaining delivery of care to diabetic patients during the pandemic. The implementation of the VA patient-centered medical home promoting team-based care, access, and continuity may have facilitated the high levels of diabetes care continuity that we found. The VA’s organizational structure, including experience with continuous quality improvement and earlier use of virtual technologies, may have also enabled the VA to adapt quickly to providing care during the pandemic.15⇓⇓–18
We found that Black and Hispanic veterans maintained access to primary care via virtual visits, but rural patients relied more on in-person care than urban patients. It is unclear whether these differences are due to clinic capabilities and staffing where these patients receive care or patients’ access to and comfort with technologies (devices, high-bandwidth Internet) to use virtual care. In the midpandemic period once COVID-19 vaccines began to be administered, VA primary care clinics prioritized high-risk patients for in-person care, which may be reflected in trends for higher in-person care for older patients during this period. The concurrent maintenance of high levels of virtual care in this midpandemic period suggests that many patients continued to choose virtual care once in-person care became more available, indicating the pandemic may have hastened the adoption of virtual care by both providers and patients for routine primary care.
Multiple VA primary care strategies may have contributed to these high levels of adherence. VA primary care teams include clinical pharmacists who help patients manage prescription fills, team-based proactive panel management dashboards for patients with diabetes and other conditions, and processes for patients to request prescription fills electronically without appointments. The VA has also long had a mail-prescription refill system. While many people experienced financial challenges and higher unemployment from pandemic-related industry shutdowns, the VA helped mitigate cost-related barriers to care by halting collection of copayments for outpatient, inpatient, and prescription medications March 2020–September 2021 through the American Rescue Plan Act.
A prior study of high-risk VA patients documented high adherence rates,11 so poor medication adherence does not seem to be a problem for most multimorbid VA patients. However, Black patients had lower rates of diabetes medication fills than White patients throughout the study period, and this difference widened during the pandemic. This may indicate that strategies or systems that mitigated gaps in medication adherence for veterans overall were not made as accessible, or were used at lower rates, by minority veterans. Proactive and effective interventions such as clinical pharmacist monitoring, automated refills, and combination pills to reduce pill burden19 could be prioritized for Black patients and clinics that serve a higher percentage of minority patients. Examining the role that structural racism plays in medication-taking behaviors for Black patients is also needed to identify potentially appropriate and innovative solutions.20,21
While there was a temporary reduction in hospitalizations, including those for diabetes complications, and ED visits during the early pandemic phase, these rates increased later. Due to widespread decreases in acute care, especially among Black, Hispanic, and nonelderly patients, the temporary reduction may have been due to patients’ avoidance of hospitals or hospitals’ inability to admit less acute cases, and the consequences of these reduced hospitalizations is not yet fully known. We did not find differences in acute care in the midpandemic period relative to the prepandemic period, so acute care use appeared to largely recover. However, a longer follow-up period is needed to assess long-term consequences.
The changes in care modality that we found for high-risk patients are consistent with a prior VA study with a broader population of veterans with diabetes that reported reductions in in-person outpatient care, increases in virtual care, and an initial decrease, then rebound, in hospitalizations.22 This study also found no effect of the pandemic on hemoglobin A1c concentrations. Other VA studies found reductions in overall VA hospitalizations after March 2020.23 Our results add a focus on high-risk patients and medication adherence and extend earlier findings by examining patterns in care for a later period of the pandemic.
Other health care systems also transitioned to providing predominantly virtual services in the early stages of the pandemic including both video telehealth and telephone.7,24 Unlike our findings, in the US, virtual primary care visits during the pandemic did not reach the level of in-person visits because total primary care use decreased compared with prepandemic levels.25 One study of private health plan data found that among patients with diabetes, there was no adverse impact of the pandemic on patients’ outpatient use, prescription fills, or hemoglobin A1c concentrations after a brief disruption in outpatient care.6 Therefore, some organizations maintained care for diabetic patients during the pandemic without immediately obvious adverse consequences. In contrast to our findings, one study of private claims data documented a higher rate of inpatient admissions for diabetes complications in the postpandemic period through 2021.26 Several studies found lower rates of hemoglobin A1c tests,27,28 lower adherence to asthma medications for Medicare patients,29 and a higher rate of discontinuation of chronic medications for patients in Massachusetts during the pandemic,30 so some health systems and populations may have experienced greater disruptions to chronic condition care than our population of high-risk VA patients.
Limitations
VA patients are older, more male, and sicker than the general population,31,32 so some results may not be generalizable to the general US population. These findings may also not be generalizable to patients who were not high risk or newly diagnosed with chronic conditions because study patients had higher levels of use and engagement with the health care system before the pandemic. Patients were identified through risk scores in the baseline year, and some patients were no longer high risk in subsequent periods. We did not assess patients’ risk scores over time because they were based on use and lab measures that were less accurate after the pandemic began, potentially affecting the interpretability of risk scores over time. We did not include Medicare use because a study of high-risk patients using VA care found low use of Medicare services33; however, we may have underestimated health care use. We did not have data on patients’ incomes, so we could not assess whether differences in use existed by income level. We measured adherence based on prescription fills and not through more direct assessment methods, so adherence may have been overestimated. Finally, we did not have measures of hemoglobin A1c or other clinical measures to assess impacts of the pandemic on health status.
Conclusion
Overall, the VA’s salaried staffing model, established primary care practices around panel management, prior experience with virtual modalities, low cost-sharing for care, and providing medications through the mail may have mitigated adverse impacts on patients’ access to primary care and crucial medications during shutdown of in-person services. Although some organizational features that enabled the VA to respond nimbly to a public health disaster are unique to the VA system, other features can be used by other health care organizations, including team-based models of care, mail delivery for medication refills, and reduced cost-sharing for the sickest patients, potentially leading to improved care during both regular times and disasters.
We identified a key area of concern because diabetes medication adherence decreased disproportionately for Black and nonelderly patients during the pandemic; these groups may need more proactive and personalized outreach during disruptions to in-person care to maintain access to and encourage adherence to medications.
Acknowledgments
We greatly appreciate the contributions of Hao Jiang for assistance with data analysis.
Appendix 1.
Regression Results for All Outcomes in Full Cohort, FY2019-2021
Appendix 2.
Mean Adjusted Number of Emergency Department Visits/Hospitalizations per Quarter in High-Risk Patients by Race/Ethnicity, Age Group, and Rurality
Appendix 3.
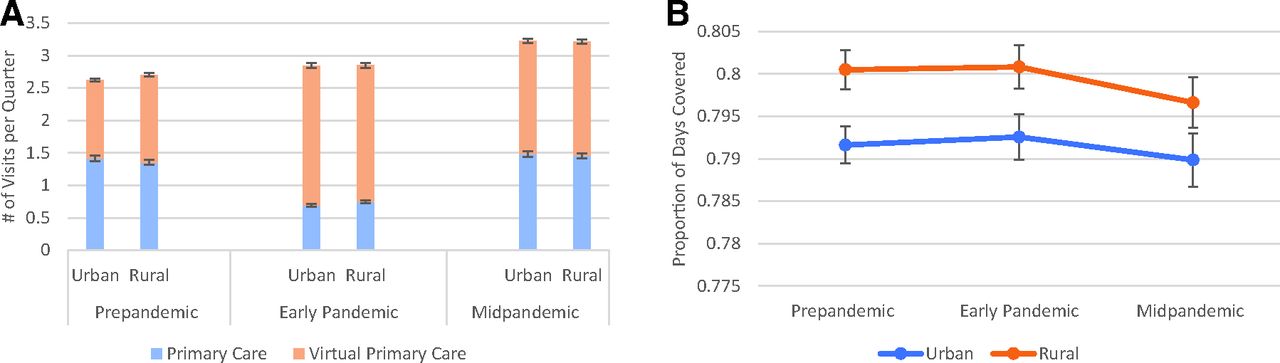
Mean Adjusted Primary Care Visits (A) and Medication Adherence (B) in High-Risk Patients by Rurality. Mean visits and adherence per quarter were estimated from linear regression models adjusting for rurality and pandemic phase and their interaction terms, quarter, patients’ sociodemographic characteristics, Elixhauser comorbidity, comorbid depression, distance to primary care site, rurality, clinic factors, and community rate of COVID infections.
Notes
This article was externally peer reviewed.
Funding: This project was supported by VA’s Primary Care Analytic Team.
Conflict of interest: The authors report no conflicts of interest.
To see this article online, please go to: http://jabfm.org/content/36/2/289.full.
- Received for publication September 16, 2022.
- Revision received October 28, 2022.
- Accepted for publication November 2, 2022.




{kind=link}
{kind=link}
{kind=link}