
Abstract
Background: We examined the impact of various comorbid conditions on diabetes and condition-specific cost-related nonadherence (CRN), and HbA1c in adults with diabetes.
Methods: This was a cross-sectional analysis of participants with diabetes and poor glycemic control in an ongoing trial (n = 600). We computed prevalence of condition-specific CRN, prevalence of specific types of diabetes-related CRN by comorbid condition, prevalence of specific types of condition-specific CRN within each comorbidity, and the association between condition-specific and diabetes-related CRN and HbA1c for each comorbid condition.
Results: Fifty-eight percent (n = 350) of participants reported diabetes-related CRN. Diabetes-related CRN rates were highest in those with liver problems (63%), anemia (61%), respiratory diseases (60%), and hyperlipidemia (60%). Condition-specific CRN rates were high in those with respiratory diseases (44%), back pain (41%), and depression (40%). Participants with cancer and kidney diseases reported the lowest rates of diabetes-related and condition-specific CRN. Delaying getting diabetes prescriptions filled was the most commonly reported form of diabetes-related CRN across all comorbid conditions and was the highest in those with liver problems (47%), anemia (46%), and respiratory diseases (45%). In adjusted models, those with back pain (beta-coefficient, 0.45; 95%CI 0.02–0.88; P = .04) and hyperlipidemia (beta-coefficient, 0.50; 95%CI 0.11–0.88; P = .01) who reported both diabetes-related and condition-specific CRN had higher HbA1c.
Conclusions: CRN in patients with diabetes is higher than in other comorbid conditions and is associated with poor diabetes control. These findings may be driven by higher out-of-pocket costs for medications to manage diabetes, lack of symptoms associated with poor diabetes control, or other factors, with implications for both clinicians and health insurance programs.
Introduction
Social determinants of health persist as key reasons why greater than 30% of people with diabetes do not meet target goals for glycemic control.1 Reducing nonadherence to treatment and management of diabetes can prevent avoidable complications, which are a substantial burden on the US Health care system.2 Nonadherence to treatment and management recommendations results from various factors, including social determinants like high out-of-pocket costs associated with treatment and regimen complexity of diabetic medications.3–4
Cost-related nonadherence (CRN) is defined as individuals taking smaller doses or skipping doses of medications, delaying or deciding not to fill a prescription or engage in routine care, and spending less money medications to pay for other necessities.5–6 Several studies have documented that CRN ranges from 14% to 30% in individuals with diabetes in the United States.6⇓⇓⇓⇓⇓⇓–12
There has been an increasing recognition of the challenges of CRN in impeding diabetes management, especially given the high prevalence of comorbid conditions evident among individuals with diabetes.13 Individuals with diabetes who took additional medications for comorbid conditions such as asthma, COPD, depression, arthritis, and other disabilities, are at higher risk of engaging in CRN.4,14,15 Cost of medications have a significant impact on the degree of medication underuse, that is, taking less medication than the prescription intended.16 There is limited data comparing the prevalence of the different types of CRN behaviors (ie, skipping/taking less medication doses, delayed/decided not to fill prescription, and delayed/decided not to see health care provider) exhibited by individuals with diabetes based on their respective comorbid conditions. In addition, the effect of CRN resulting from various comorbid conditions on hemoglobin A1c (HbA1c) has not been studied. A better understanding of the effect of CRN resulting from comorbid conditions on the management of diabetes can support more tailored interventions to improve treatment adherence that accommodates the cost-related challenges of managing multiple conditions.
The purpose of this study was to compare the prevalence of various forms of CRN behaviors in individuals with diabetes, and also for their respective comorbid conditions such as anemia, asthma, chronic obstructive pulmonary disease (COPD), arthritis, back pain, cancer, depression, gastrointestinal problems, clinical atherosclerotic cardiovascular disease (ASCVD), hypertension, hyperlipidemia, HIV/AIDS, kidney disease, and liver problems. We also examined the association between CRN within specific comorbid conditions, and HbA1c. We hypothesize that there will be differential prevalence of types of CRN behavior among individuals with diabetes and within certain comorbid conditions, and differential impact of CRN resulting from comorbid conditions on clinical outcomes, such as HbA1c.
Methods
Data Sources
This study is a secondary data analysis of baseline assessments of participants in a randomized controlled trial evaluating approaches to addressing unmet social risk factors among people with diabetes.17 All study procedures were approved by the University Institutional Review Board.
Study Sample
Potential participants meeting the following criteria were identified via the University Diabetes Research Registry18, and the health system’s electronic health record: 1) 18 to 75 years of age, 2) diagnosis of type 1 or type 2 diabetes with prescribed oral or injectable antihyperglycemic medication, 3) most recent (within the past 6 months) recorded HbA1c level of ≥7.5% for individuals ≤70 years and >8.0% for individuals between 70 to 75 years in age, 4) positive report of financial burden or cost-related nonadherence using screening questions developed and validated from prior work5–6, and 5) access to a mobile phone. Exclusion criteria included significant cognitive impairment or active participation in another diabetes-related research study.
Eligible and interested patients gave informed consent before their baseline assessments. A total of 6055 potential participants were initially contacted, of which 997 were confirmed to be eligible. Of those, 666 (66%) consented to participate, and 600 provided completed surveys. This analysis is based on the completed 600 surveys.
Data Collection and Measures
In-person interviewer-assisted surveys were conducted by trained staff before March 11, 2020, the same day the World Health Organization (WHO) declared the COVID-19 pandemic. Since then, surveys were administered over the telephone. Standard demographic characteristics and clinical data were collected via self-report. Hemoglobin A1c was measured via a fingerstick blood test.
Cost-Related Nonadherence (CRN) Behaviors
To measure CRN behaviors for diabetes and other comorbid conditions, participants were asked if they engaged in any of the following behaviors in the past 12 months due to financial burden for diabetes and each of their other comorbid conditions: took less medications, skipped medication doses, delayed or decided not to fill a prescription, and delayed or decided not seeing a health care provider (4-point Likert scale: never to often). These behaviors were analyzed as dichotomous variables, with ‘never’ and ‘rarely’ indicating ‘no’ CRN, and ‘sometimes’ and ‘often’ indicating ‘yes’ to CRN. The percentage of participants with a positive response were reported for each of the 6 items.
Comorbid Chronic Conditions
In addition to diabetes, participants were asked if their provider has ever diagnosed them with any of the following chronic conditions: anemia, asthma/COPD, arthritis, back pain, cancer in the past 3 years, depression, digestive problems, clinical ASCVD, hypertension, hyperlipidemia, kidney disease, and liver problems (y/n). These conditions were chosen to align with chronic conditions queried in national surveys.19
Statistical Analysis
All analyses were completed using R statistical package. Descriptive statistics, chi-square, and t test were computed to describe differences in diabetes-related CRN by demographic and clinical characteristics. Descriptive statistics were computed to describe the prevalence of condition-specific CRN, prevalence of specific types of diabetes-related CRN by comorbid condition, and prevalence of specific types of condition-specific CRN within each comorbidity. Multiple variable regression models were computed to examine the association between condition-specific CRN and HbA1c for each condition of interest, and the association between occurrence of CRN for both diabetes and comorbid condition, and HbA1c for each condition of interest. Models were adjusted for age, sex, number of comorbid conditions, health insurance type, and type of diabetes (type 1 or type 2).
Results
Sample Characteristics
A total of 600 participants were included in the analytic sample (Table 1). On average, participants were 53 years of age. Fifty-eight percent of participants reported at least 1 diabetes-related CRN behavior, and 32% of participants reported 4 or more types of diabetes-related CRN behaviors. Compared with those who did not report diabetes-related CRN, those who reported diabetes-related CRN were more likely to identify as non-White (P < .05), have private insurance (P < .05), and higher HbA1c (P < .05) (Table 1).
Sample Characteristics
Prevalence of Diabetes-Related and Condition-Specific Cost-Related Non-Adherence
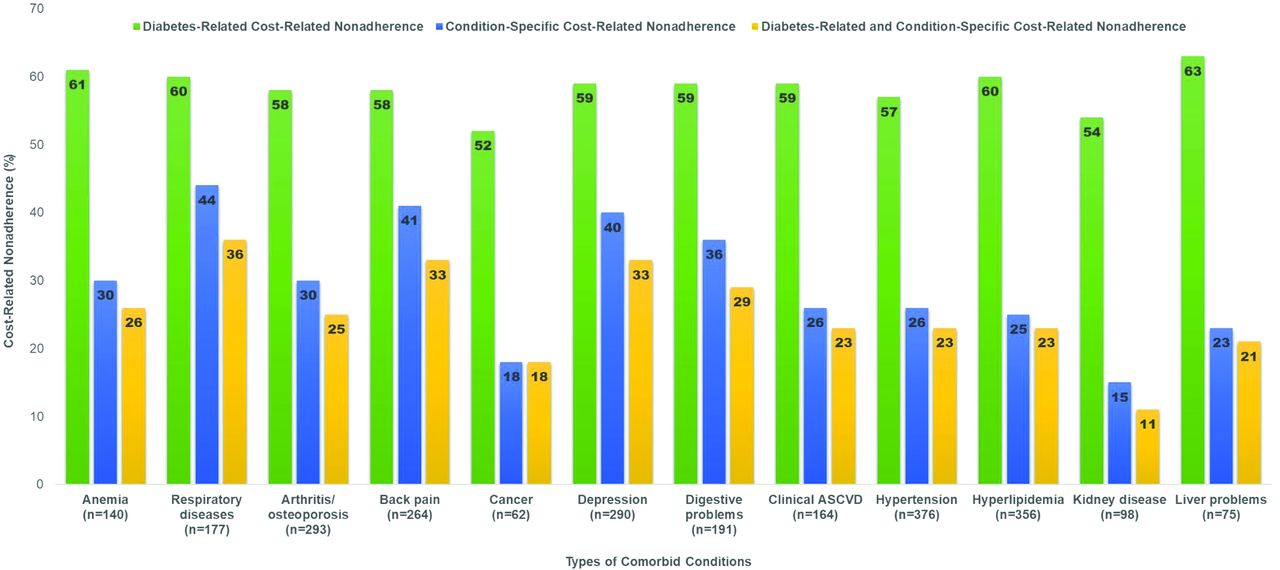
The prevalence of CRN related to diabetes, specific conditions, and both are represented in Figure 1 Prevalence of diabetes-related CRN among all comorbid conditions were comparable, ranging from 52 to 63%. Diabetes-related CRN was highest in those with liver problems and anemia at 63% and 61%, respectively. Participants with cancer and kidney disease reported lowest rates of CRN related to their diabetes (52% and 54%, respectively), their specific conditions (18% and 15%, respectively), and both (18% and 11%, respectively). Participants with respiratory diseases, back pain, and depression reported the highest prevalence of condition-specific CRN (44%, 41%, and 40%, respectively) and both diabetes-related and condition-specific CRN (36%, 33%, and 33%, respectively). Among all comorbid conditions, diabetes-related CRN was higher than condition-specific CRN (Figure 1).

Prevalence of diabetes-related and condition-specific cost-related nonadherence.
Behaviors of Diabetes-Related and Condition Specific Cost-Related Non-Adherence by Comorbid Conditions
Types of diabetes-related CRN by comorbid conditions are represented in Figure 2a. Among those who engaged in diabetes-related CRN, more people who reported taking smaller doses of their medications for diabetes had concurrent anemia (32%) or liver problems (35%). Prevalence of participants who skipped doses of diabetes medicine were comparable among all comorbid conditions with highest rates reported in those with clinical ASCVD (32%) and liver problems (31%). Delayed getting prescriptions filled for diabetes was the most common diabetes-related CRN behavior among all comorbid conditions and it was frequently reported in those with liver problem (47%), anemia (46%), digestive problems (46%), clinical ASCVD (46%), and respiratory diseases (45%). More people who reported that they decided not fill their medication for diabetes had concurrent anemia (36%), clinical ASCVD (34%), and liver problems (33%). Participants with anemia and liver problems were more prone to delay (36% and 35%, respectively) or decide not (29% and 32%, respectively) seeing their health care provider for diabetes due to cost (Figure 2a).

Behaviors of diabetes-related and condition specific cost-related nonadherence by comorbid conditions.
Types of condition-specific CRN by comorbid conditions are represented in Figure 2b. Taking smaller doses of their medication to manage their condition was highest among those with respiratory disease (25%) or back pain (24%). Those with respiratory diseases (27%) or back pain (23%) also had a higher prevalence of skipping doses of their medication to manage their conditions. Participants with respiratory diseases (34%), digestive problems (22%), depression (21%), and back pain (21%) were more likely to delay filling their medications for these conditions. Twenty-nine percent of participants with respiratory diseases reported not getting their respiratory medications filled due to cost, which was significantly higher than all other comorbid conditions. Those with respiratory diseases, back pain, and depression were also more likely to delay (27%, 28%, and 26%, respectively) or decide not (20%, 24%, and 23%, respectively) seeing their health care providers due to cost (Figure 2b).
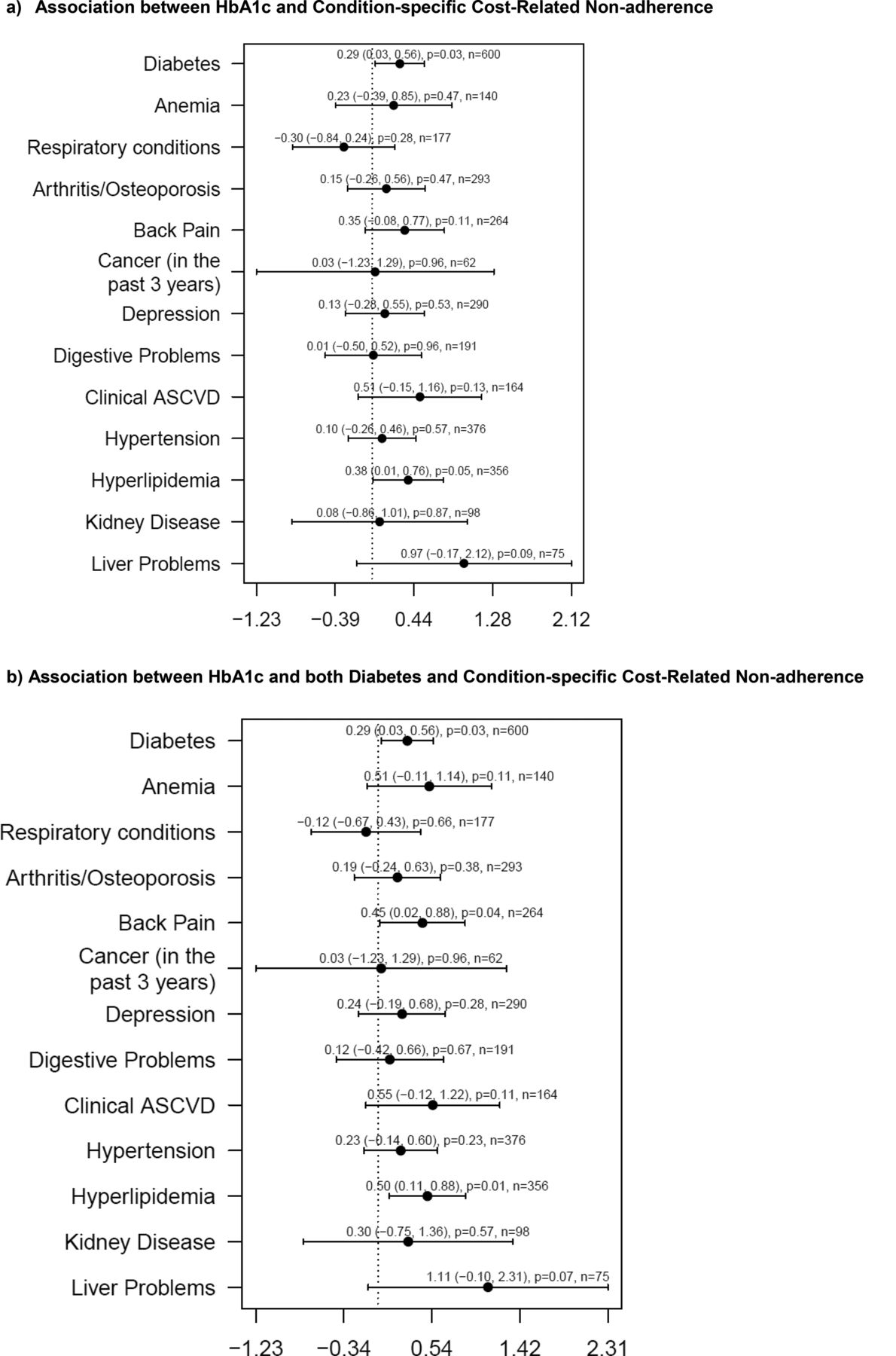
Association between hba1c and Both Diabetic and Condition-Specific Cost-Related Non-Adherence Comorbid Conditions
In multiple variable regression models, participants with diabetes-related CRN and hyperlipidemia-related CRN were more likely to have elevated HbA1c levels compared with those with other condition-specific CRN, when adjusted for age, sex, number of comorbid conditions, health insurance type, and type of diabetes (Figure 3a). Those with hyperlipidemia and diabetes, and back pain and diabetes (who reported both diabetes-related and condition-specific CRN also had higher HbA1c, when adjusted for age, sex, number of comorbid conditions, health insurance type, and type of diabetes (Figure 3b).

Associations between HbA1c and cost-related nonadherence by comorbid conditions. Abbreviation: ASCVD, clinical atherosclerotic cardiovascular disease.
Discussion
Economic Burden is an Important Social Determinant to Disease Management and Treatment Adherence
Cost-related nonadherence has become increasingly prevalent among individuals with diabetes in the US6⇓⇓–9 Our study builds on prior work examining CRN among people with diabetes and comorbid conditions,and is the first study to examine types of CRN behaviors that are associated with diabetes and concurrent comorbid conditions. We found that participants were more likely to engage in CRN for their diabetes compared with their other comorbid conditions. This suggests that when affordability is a concern, individuals are more likely to skip, take smaller doses, or not fill their medication for diabetes compared with medications that treat their comorbid conditions.
Our finding showed that participants with hypertension and hyperlipidemia report comparable rates of diabetes-related CRN to those with other comorbid conditions. About a fourth of these participants reported hypertension-related or hyperlipidemia-related CRN, which were lower than most of the other comorbid conditions evaluated in this study. These findings may be driven by the higher out-of-pocket costs for medications to manage diabetes compared with those for hypertension and hyperlipidemia. Blue Cross Blue Shield of Michigan (BCBSM), the largest health insurer in Michigan, placed common medications for hypertension and hyperlipidemia under Tier 1 with the lowest out-of-pocket cost.20 On the contrary, insulin and many noninsulin hypoglycemic agents are placed in higher tiers, resulting in greater financial burden for individuals with diabetes.20
We found that more than half of participants with respiratory diseases engaged in diabetes-related CRN and more than a third engaged in respiratory-disease-related CRN, which were both among the highest across all comorbid conditions. These participants reported high rates of taking smaller doses, skipping doses, delayed or decided not filling their prescriptions for both diabetes and respiratory diseases. Respiratory diseases and anemia were the 2 comorbid conditions with the highest rates of delayed getting diabetes medications filled due to cost. Other work has shown that intravenous iron replacement therapy to treat anemia, and inhaled corticosteroids used for respiratory diseases may lead to insulin resistance and elevated HbA1c.21–22 Due to insulin resistance and elevated HbA1c, it can be more challenging for providers to manage glycemic levels. Hence, the higher prevalence of CRN found in participants with anemia and respiratory diseases may be attributed to higher dose and frequency of insulin required to achieve adequate glycemic control. This would lead to more prescriptions or higher supply of insulin per pharmacy visit. In addition, individuals with type 2 diabetes with anemia or respiratory diseases may need additional and earlier initiation of medications with higher out-of-pocket costs, such as dipeptidyl peptidase 4 (DPP-4) inhibitors, sodium-glucose cotransporter-2 (SGLT-2) inhibitors or glucagon-like peptide-1 agonists (GLP-1).20
Our study found that participants with liver problems reported the highest rate of diabetes-related CRN. Few data describe the effect of liver problems on the prevalence of diabetes-related CRN. However, the presence of liver problems is a challenge for providers when it comes to choosing a medication for diabetes. Many cheaper oral medications for diabetes are metabolized by the liver; hence, these therapy options are contraindicated in individuals with severe liver problems.23 Furthermore, treatment algorithms for diabetes in individuals with severe forms of liver diseases suggest earlier initiation of insulin if glycemic control cannot be maintained on metformin.24 Since the out-of-pocket cost of insulin is significantly higher than most oral medications, individuals with liver problems may be more prone to engage in CRN, especially diabetes-related CRN.
Although it is well established that a cancer diagnosis creates significant financial toxicities for patient and their families25–27, we found that participants were 3 times more likely to engage in diabetes-related CRN compared with cancer-related CRN. Participants who reported cancer-related CRN reported higher rates of delaying or forgoing not seeing an oncologist due to cost compared with other cancer-related CRN behaviors. Our findings were slightly higher than previous studies that found CRN to be around 10% to 15% of individuals with cancer regardless of having diabetes.4,28 Potential determinants of these trends require further investigation. Many health care systems have adopted financial navigation programs into their oncology care model and have found these programs to be effective in reducing delays in cancer care for individuals with socioeconomic vulnerabilities.29–30 Despite their positive impact on cancer care, most financial navigation programs have mostly been implemented in cancer care settings. It is unclear the extent to which these programs address the financial toxicities associated with other comorbid conditions such as diabetes. Surprisingly, our study found that participants with diabetes and cancer did not report higher HbA1c compared with those with other comorbid conditions, which suggests that the magnitude of diabetes-related CRN in those with cancer was not significant enough to cause negative clinical outcomes related to diabetes.
Our study found that close to a third of participants engaged in CRN related to both diabetes and back pain, and these participants also reported higher HbA1c levels. In addition, participants with back pain reported relatively higher rates of all types of CRN behavior related to their medications for diabetes and back pain. Guidelines regarding the management of chronic back pain recommends initiating nonpharmacological options including superficial heat, massage, acupuncture, and spinal manipulation.31–33 Some of these services are either not covered or difficult to obtain payment approval from most health insurance companies.34–35 The expenses associated with these services coupled with the high out-of-pocket cost for insulin and noninsulin hypoglycemic agents can place substantial financial burden on individuals with diabetes and chronic back pain. This can lead to diabetes and chronic back pain to become uncontrolled, which can further the severity of both conditions.
There are limitations in this study that should be noted. In the absence of pharmacy claims or electronic health records, we are unable to verify the accuracy of self-reported data on CRN. Specific types of liver disease, cancer, respiratory problems, and cardiovascular diseases were not identified and studied. Participants were not asked to specify their chronic kidney disease stage, which may impact the choice of therapy for diabetes management. In addition, participants were not asked to state their HbA1c goal set by their provider. All these parameters can affect the number and type of medications required to manage to their diabetes as well as concurrent comorbid conditions, which can ultimately impact outcomes associated with CRN. Furthermore, nearly all the participants had some form of insurance coverage, so the generalizability of our results may not apply to individuals with no health insurance. Despite these limitations, the prevalence of CRN reported from our study are similar with those reported in the literature.6⇓⇓⇓⇓⇓–12
This study has important implications for health policy and clinical practice. Management of diabetes is especially complicated in individuals with concurrent comorbid conditions. Historically, providers have been focused on managing individuals’ health conditions without considering the financial implications that treatment and management regimens have on patients. More research is needed to provide adequate tools and support to screen for and mitigate the risk of CRN across comorbid conditions. With increasing technology use in clinical settings and greater emphasis on team-based care, there are opportunities to direct patients to care team members who can assist them with financial resources or enroll them into manufacturer or government sponsored programs. Given the noticeable, positive impact of financial navigation programs in reducing financial burden for cancer patients, expanding these health care services to other therapeutic areas beyond cancer may provide considerable improvement in CRN and health outcomes across multiple co-occurring conditions. To incentivize hospitals to expand financial navigation programs, there needs to be more evidence to prove that these programs can provide substantial cost-savings across clinical conditions.
Conclusion
Individuals with diabetes and additional comorbid conditions are at high risk of experiencing both diabetes-related and condition-specific CRN, especially in those with anemia, respiratory disease, and back pain. There is an increasing need for health care teams to screen patients for CRN, especially in those with multiple comorbid conditions, to better address economic burden that may have adverse consequences on health outcomes.
Acknowledgments
Authors would like to thank the study staff and participants.
Notes
This article was externally peer reviewed.
Funding: This work was supported by the University of Michigan Institute for Healthcare Policy and Innovation Student Fellowship program, National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (R01 DK116715-03) and (P30DK092926) (Michigan Center for Diabetes and Translational Research).
Conflict of interest: The authors have no conflicts of interest to disclose.
To see this article online, please go to: http://jabfm.org/content/36/1/15.full.
- Received for publication August 8, 2022.
- Revision received October 1, 2022.
- Revision received October 5, 2022.
- Accepted for publication October 11, 2022.




{kind=link}
{kind=link}
{kind=link}