
Abstract
Purpose: Functional status is a major contributor to overall health and reflects both daily activity level (performance) and maximum attainable activity level (capacity). Existing assessment tools evaluate only 1 domain of function and do not provide insight into contributors to functional decline. We addressed these deficiencies by developing the Tennessee Functional Status Questionnaire (TFSQ), which reports activity levels in metabolic equivalents (METs) and evaluates 5 key areas: performance, capacity, activity, pain, and acute care. We validated the activity levels reported by the TFSQ against the Duke Activity Status Index (DASI).
Methods: In this prospective, observational study, 120 patients completed both the TFSQ and the DASI. TFSQ-reported functional performance and capacity was correlated with DASI-calculated METs.
Results: Pearson correlation between TFSQ-reported capacity and DASI-calculated METs was r = 0.69, P < .001. TFSQ capacity was significantly lower in patients who reported recently decreased activity, pain affecting function, or recent acute care exposure.
Conclusions: The TFSQ is a brief and efficient assessment of patient function, standardized to METs and validated against the DASI. Our study suggests that many patients may have the functional reserve to increase daily physical activity and that factors such as changes in activity, pain, and recent acute care interaction may lower functional capacity.
- Chronic Disease
- Exercise
- Functional Performance
- Functional Status
- Geriatrics
- Health Promotion
- Metabolic Equivalent
- Surveys and Questionnaires
- Tennessee
Introduction
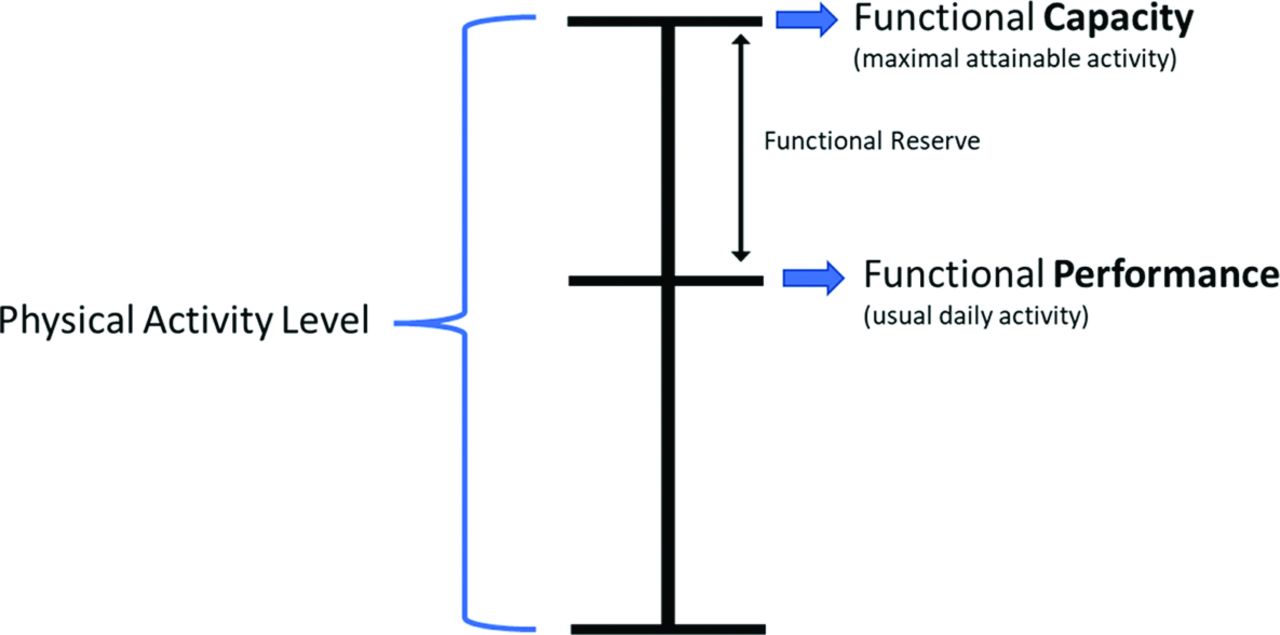
In today’s fast-paced, outcomes-focused health care environment, it is important to have brief and efficient tools that enhance holistic clinical assessment. Patient physical activity and function is one area that is often inconsistently assessed. Patient physical activity level is a major predictor of overall health and mortality1 and is dependent on a patient’s functional status. A patient’s functional status reflects the person’s “ability to perform daily activities required to meet basic self-care needs and maintain health and wellbeing”2 and is composed of both the patient’s functional performance (usual daily physical activity) and the person’s functional capacity (maximal attainable physical activity). Functional capacity may or may not exceed functional performance, depending on the amount of functional reserve a patient possesses (Figure 1). Functional status can be affected by the presence of pain3 or by recent acute care episodes (emergency department [ED] visit, hospitalization, or surgery).4 Proactively identifying a patient’s functional status can guide a clinician to facilitate and evaluate treatment, set treatment goals, and help prevent a patient’s further functional decline.5⇓–7

Graphical depiction of the components of functional status. Functional status is composed of both functional performance and functional capacity. Functional performance reflects usual physical activity level. Functional capacity is the maximal attainable physical activity level. Functional reserve is the difference between functional performance and functional capacity.
Objective reporting of physical activity can be challenging due to the variability of physical activity intensity. One method of standardizing function is to convert reported physical activity levels into corresponding metabolic equivalents (METs), with 1 MET being the patient’s energy expenditure at rest, or the amount of oxygen consumed while at rest.8 Functional capacity is therefore often reported in METs.9 Functional capacity in METs can be objectively assessed by using direct measurement (exercise stress testing)9 or validated activity questionnaires such as the 12-question Duke Activity Status Index (DASI).10 These existing methods are limited in that they require complex equipment or only assess maximal attainable physical activity, which is just 1 component of functional status. In addition, none of these assessment methods directly report on functional performance, functional trajectory, or factors known to affect functional capacity. There currently is no time-efficient tool that can be used by clinicians at point-of-care to establish a patient’s functional status at baseline, reassess following a health event, and establish a trajectory of functional recovery.
We sought to address these deficiencies in functional status assessment by developing and validating a patient-reported survey instrument that would be brief, be easy to score, and indicate specific areas for attention and potential intervention. These efforts led to the development of the novel 5-question survey instrument the Tennessee Functional Status Questionnaire (TFSQ), which allows patients to report both their functional performance and functional capacity in METs along with identifying any activity changes, pain affecting function, or recent acute care interactions.
In this prospective observational study, we present the development of the TFSQ and the initial validation data comparing the TFSQ-reported functional capacity in METs to the functional capacity calculated from the 12-question DASI. We hypothesized that there would be at least a moderate correlation between both MET values. Further, we used the TFSQ to better understand the relationship between the 2 components of functional status and compared those responses to recent changes in physical activity and factors known to be associated with functional decline. We hypothesized that recently decreased activity level, pain affecting activity, and acute care exposure (ED visit, hospitalization, or surgery) are each independently associated with reduced functional capacity and functional performance.
Methods
TFSQ Design and Development
The TFSQ (Appendix) was developed to address the aforementioned deficiencies in functional status assessment. We identified 2 components that would be necessary to accomplish this goal. The first was a simple table of activities from which patients could select their respective activity levels (functional performance or functional capacity) and identify their level of energy expenditure in METs (Table 1). The activities were chosen to represent a broad range of familiar self-care, caregiver, indoor, outdoor, and sporting activities. The associated energy expenditure in METs for each activity was determined from the Compendium of Physical Activities,8 a listing of more than 800 specific activities with associated measured or calculated MET values. The activities were then grouped according to similar levels of energy expenditure into 5 ordinal columns of activities (A–E) representing MET values of <3METs to >6METs (Table 1).
Columns of Activities, Grouped by Metabolic Equivalents (METs), for Tennessee Functional Status Questionnaire (TFSQ) Questions 1 and 2
Tennessee Functional Status Questionnaire (TFSQ): TFSQ Questions 1–5 Ask Details about Functional Performance, Capacity, Activity, and Acute Care. Questions 1 and 2 Refer to Columns A–E Listed in Table 1. (See Appendix for the Complete Instrument)
The second component of the TFSQ was the specific questions that were asked to generate a more robust functional assessment picture (Table 2). Each question (TSFSQ 1 to 5) was chosen and carefully worded to assess a separate component of function. Performance (TFSQ 1) assesses functional performance, asking patients to rate their usual level of activity by selecting the appropriate column (A–E) from the activity table. Capacity (TFSQ 2) assesses functional capacity by asking patients to rate their best level of activity using the same columns of activities (A–E). Activity (TFSQ 3) assesses for recent (within the past 60 days) changes in physical activity level. Pain (TFSQ 4) assesses if the respondent has pain that limits physical activity. Acute care (TFSQ 5) evaluates if the respondent had acute care exposure through an ED visit, hospitalization, or surgery in the past 60 days. The entire TFSQ was then assessed for readability using SMOG11 and Flesch-Reading Ease12 to ensure it was between 3rd-grade and 6th-grade reading level.
Participants and Setting
This internal review board–approved prospective observational study compared patient responses on the TFSQ with responses to the DASI across 2 sites: the Family Medicine Clinic (UFP) and the Chronic Pain Clinic (Pain Clinic). Our inclusion criteria consisted of patients over age 18 presenting for well visits (UFP) or new patient consults (Pain Clinic) who were willing and able to independently complete both questionnaires. Exclusion criteria consisted of patients under age 18 or those who were unwilling or unable to independently complete both questionnaires. All participants completed both the DASI and the TFSQ during the same visit. To account for potential respondent biases, the order of the DASI and TFSQ were counterbalanced randomly as to which survey instrument was completed first. The data were collated using Research Electronic Data Capture (REDCap) software (Vanderbilt University, Nashville, TN).
TFSQ Validation and Analysis
Our primary objective was to validate the functional capacity (TFSQ 2) MET values reported by the TFSQ to the MET values calculated from the DASI. The DASI is a validated 12-question patient-reported measure of functional capacity10 that asks participants what they “can” do, with the sum of each weighted answer calculating an index value. A published and validated formula is then used to convert this to METs.10 The American College of Cardiology/American Heart Association recommends using the DASI in preoperative risk assessment to determine functional capacity.9 Our secondary analysis evaluated the relationship between functional performance and functional capacity as they related to each other and then further associated each component with recent change in physical activity level, presence of pain affecting activity, and recent acute care exposure (ER/hospitalization/surgery).
Statistical Power
An a priori sample size calculation was performed with the following parameters: 2-tailed hypothesis, α value of 0.05, β value of 0.20, null hypothesis of r = 0.00, moderate correlation of 0.40 between the TFSQ and DASI, and an attrition rate of 30%. The sample size calculation yielded a needed sample size of n = 66 based on the stated parameters.
Statistical Methods
Frequency and descriptive statistics were used to describe the demographic characteristics of the sample. The MET values from the DASI instrument were calculated using the associated scoring rubric.10 The METs reported from TFSQ 2 (functional capacity) were validated against the METs calculated from the DASI. Frequency statistics were used to calculate the number of missing observations. Missing data were assessed for randomness using MCAR (missing completely at random) analysis. Pearson’s r correlation was employed to test for significant associations between the MET values from TFSQ question 2 and the MET values derived from the DASI to generate convergent validity evidence. The statistical assumption of homogeneity of variance for the ordinal columns of responses (A–E) to TFSQ questions 1 and 2 and the categorical responses to questions 3, 4, and 5 was assessed using Levene’s test of equality of variances.
Cross-tabulation tables were used to assess the level of concordance between functional performance (TFSQ 1) and capacity (TFSQ 2). An independent samples t-test was performed to compare the respondents’ answers to performance and capacity (TFSQ questions 1 and 2) across activity (TFSQ 3) responses. Independent sample t-tests were also used to compare the respondents that responded yes or no on pain (TFSQ 4) on their respective average answers to performance and capacity (TFSQ 1 and 2). The same analysis was used to compare those who responded yes or no to recent exposure to acute care (TFSQ 5). Means and SDs for the TFSQ question comparisons were reported and interpreted using numeric values 1 to 5 to associate with the TFSQ ordinal columns A through E.
The statistical analyses were performed using SPSS Version 28 (IBM, Armonk, NY), and statistical significance was assumed at an α value of 0.05.
Results
A total of n = 120 patients participated in this study. The sample was primarily female (n = 77, 65.3%), white (n = 106, 92.2%), and non-Hispanic (n = 102, 97.1%). The frequency and descriptive statistics of the patient sample and their responses to the TFSQ questions are presented in Table 3. Missing data for each of the TFSQ questions are also reported in Table 3. MCAR analysis showed that the missingness in the data set was random, therefore we continued with the statistical analysis. We decided not to impute any values at this juncture as we sought to generate validity evidence for the TFSQ.
Characteristics of Sample and Responses to Tennessee Functional Status Questionnaire (TFSQ) Questions (Study Participants, Demographics, and Descriptive Statistics)
Correlation of TFSQ with DASI
Pearson’s r correlations yielded evidence of convergent validity with statistically significant positive correlations between the TFSQ-reported functional capacity in METs (TFSQ 2) and the DASI-calculated METs, r = 0.690, P < .001 (Figure 2). There was also a positive correlation between TFSQ-reported performance (TFSQ 1) and the MET values generated by the DASI, r = 0.565, P < 001. Both correlations are considered strong effects as defined by Cohen.13
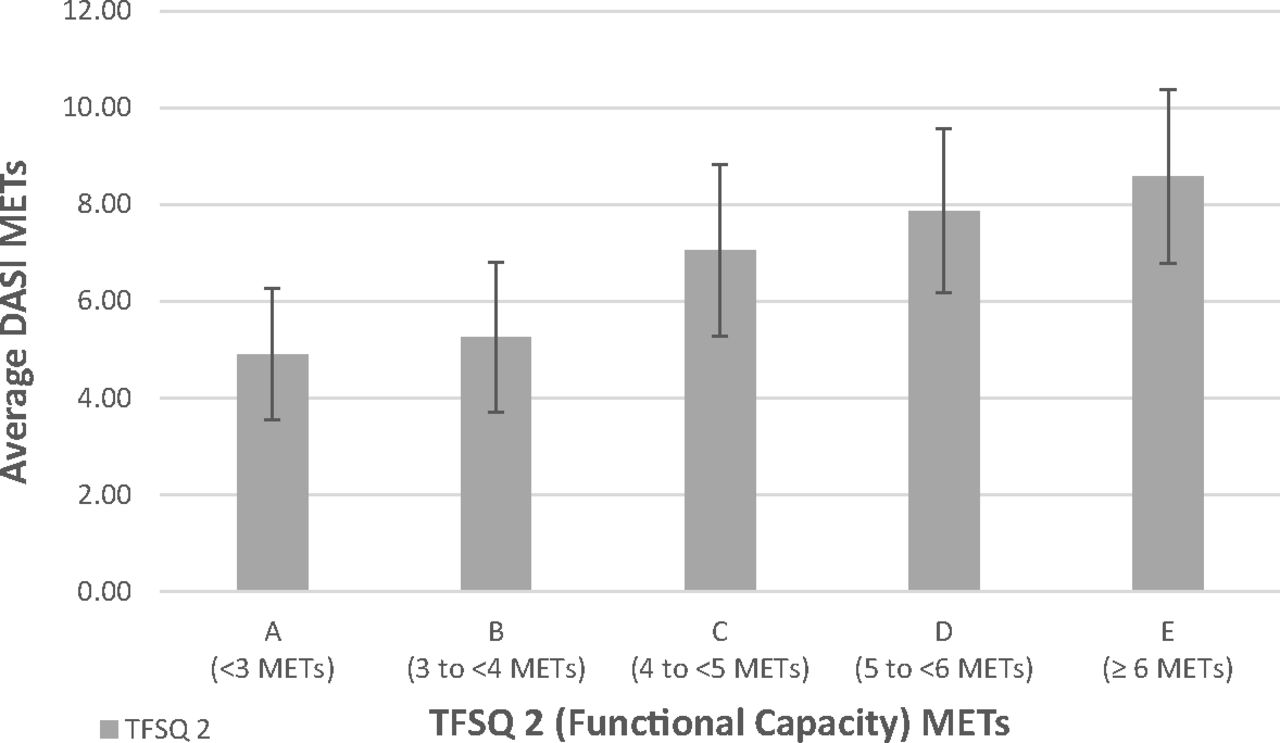
Distribution of mean Duke Activity Status Index (DASI) metabolic equivalents (METs) per corresponding Tennessee Functional Status Questionnaire (TFSQ) response. TFSQ 2 assesses functional capacity; that is, a patient's maximal attainable level of physical activity. Standard deviation (SD) represented by error bars. Statistically significant positive correlations between the TFSQ 2-reported METs (functional capacity) and DASI-calculated METs. Pearson's r correlation r = 0.690, P < .001.
Functional Performance (TFSQ 1) and Capacity (TFSQ 2)
The difference in frequency distribution between functional performance (TFSQ 1) and functional capacity (TFSQ 2) is shown in Figures 3a and 3b. The cross-tabulation analysis showed that there was concordance between the responses to TFSQ 1 and TFSQ 2 46.1% of the time (n = 47 respondents out of a total of 102). The cross-tabulation tables also showed that the discordance between the responses to TFSQ question 1 and TFSQ question 2 was greater than 2 (2) column deviations 20.6% of the time (21/102 respondents).
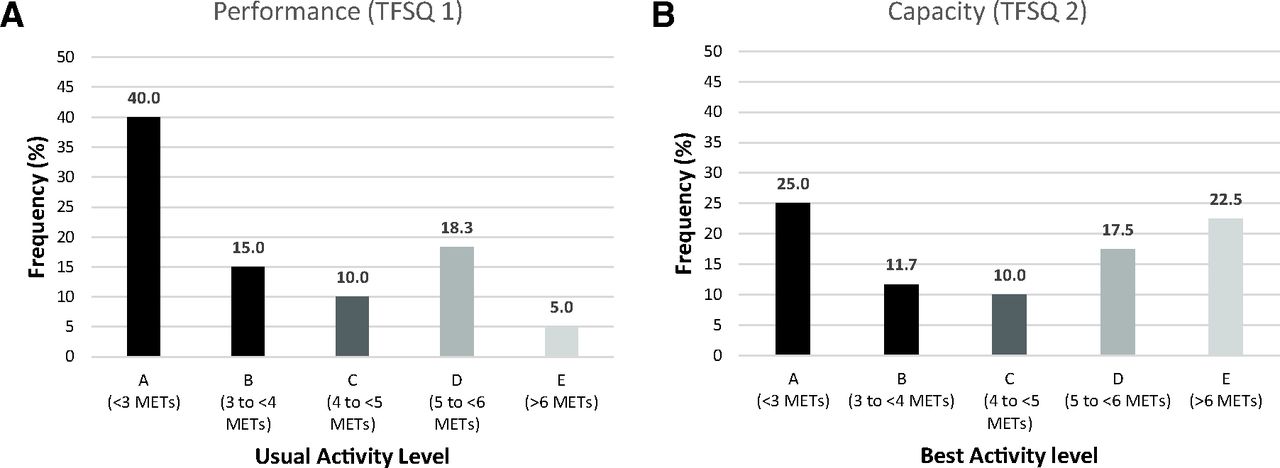
A: Frequency distributions for Tennessee Functional Status Questionnaire (TFSQ) 1—functional performance. Patients selected their usual activity level from 1 of 5 columns of activities (A–E) grouped according to Metabolic Equivalents (METs) (<3 METs to >6 METs). B: Frequency distributions for TFSQ 2—functional capacity. Patients selected their best activity level from 1 of 5 columns of activities (A–E) grouped according to METs (<3 METs to >6 METs).
Activity (TFSQ 3)
There was a statistically significant difference in both performance (TFSQ 1) and capacity (TFSQ 2) for persons reporting less activity (TFSQ 3) in the past 60 days, compared with those who reported no change or being more active. Those reporting being less active in the past 60 days had significantly lower reported performance, P = .048, and functional capacity (TFSQ 2), P = .047. This also held true for the calculated DASI MET values, with patients reporting that they were less active reporting significantly fewer METs than more active (P = .002) and no change (P < .001). See Table 4 for the relevant means and SDs.
Tennessee Functional Status Questionnaire (TFSQ) Internal Consistency: Functional Performance (TFSQ 1) and Capacity (TFSQ 2), Associations with Activity (TFSQ 3), Pain (TFSQ 4), and Acute Care (TFSQ 5) (and Corresponding Duke Activity Status Index [DASI] Metabolic Equivalents [METs] for Pain and Acute Care)
Pain (TFSQ 4)
Patients reporting yes to pain (TFSQ 4) had significantly lower functional performance (TFSQ 1), P = .009 (n = 70), and functional capacity (TFSQ 2), P < .001 (n = 66) than those who reported no pain. See Table 4 for the relevant means and SDs. The mean DASI-reported MET value was also significantly lower for those respondents reporting pain versus no pain, P < .001 (Table 4).
Acute Care (TFSQ 5)
Patients reporting yes to acute care (TFSQ 5, ED/hospitalization or surgery in the past 60 days) had significantly lower functional capacity (TFSQ 2) than those who reported no, P = .017 (n = 20; see Table 4). The mean DASI-reported METs were also significantly lower for patients answering yes to acute care (TFSQ 5) versus those who answered no (P = .003) (Table 4).
Discussion
We developed the TFSQ to enhance functional status assessment by evaluating both functional performance and functional capacity in METs and provide actionable information on activity, pain, and acute care effects on function. We validated the METs reported by the TFSQ by correlating them with the MET values calculated from the DASI. We further used the TFSQ to assess how both components of functional status relate to change in activity, presence of pain affecting activity, and recent ED visits, hospitalization, or surgery. In doing so we were able to capture a quantifiable functional status snapshot of the participating subjects while also gaining insight into factors that may affect their functional status.
Our data showed a strong correlation between functional capacity (TFSQ 2) and DASI METs (r = 0.69, P < .001). This provides robust psychometric evidence that the self-selection of best activity level from 1 of the 5 TFSQ activity columns (Table 1) provides an adequate estimation of patient functional status compared with the 12-question DASI. There was also a statistically significant correlation between functional performance (TFSQ 1) and DASI METs (r = 0.565, P < .001), although this correlation was expected not to be as strong as the correlation between functional capacity (TFSQ 2) and DASI because functional performance is often not as intense as functional capacity.
Indeed, one key finding in our study was the difference in distribution between functional performance (TFSQ 1) and functional capacity (TFSQ 2) in the sample (Figure 3). We found that TFSQ-reported functional performance was skewed to lower MET values, with 40% of respondents selecting column A (<3 METs), and only 5% of patients selecting column E (>6 METs). However, when the same patients were asked to report their functional capacity, only 25% of patients selected column A, with 22.5% of patients indicating they could perform activities of > 6 METs. These findings suggest there is an opportunity to encourage additional physical activity in our patients, as many patients have the capacity and functional reserve (Figure 1) to be more active in their daily lives. Another finding of interest was the discordance between TFSQ 1 and 2 (53.9%), with there being a minimum of 2-column difference in functional performance and functional capacity 20.6% of the time. Although some of the discordances may be explained by the physiologic barriers to function assessed in this tool (pain, acute care, and so forth), behavioral science suggests that there are also psychological barriers to physical activity that may need to be addressed.14
We also investigated the link between recent changes in activity (TFSQ 3) and functional capacity (TFSQ 2). We found that those participants who reported being less active in the previous 60 days had significantly lower functional capacity and functional performance than those who reported no change or increased activity. This reported decrease in physical activity may serve as an early warning sign of a negative functional trajectory. Awareness of this trajectory may in turn lead to opportunities for the clinician to intervene to prevent further functional decline.
Analysis of responses to pain (TFSQ 4), showed that patients who had pain that affected their daily physical activity reported significantly lower functional performance (TFSQ 1) and functional capacity (TFSQ 2) than those who did not report pain (P < .001). TFSQ 4 prompts the clinician to assess whether the decreased physical activity is due to an inability to perform at a higher level because of limitations from pain versus being due to a possible lack of effort (see the difference between MET frequencies in TFSQ 1 and 2 [Figure 2]). Studies show that pain frequency and intensity are negatively associated with disability, and early intervention of pain is known to result in better functional outcomes.15
Acute care (TFSQ 5) asks about recent ED visits, hospitalization, or surgery. Affirmative answers to this question were also associated with lower functional capacity than those who answered no (P = .017). This is consistent with the findings of Brown et al,4 who noted that participants more than 75 years old with either ED visits or hospitalization had a decrease in function that did not return to baseline even after 1 year. This finding highlights the importance of clinicians proactively identifying such patients and initiating functional restoration measures such as posthospitalization rehabilitation and active physical therapy to prevent further functional decline.
This study has important limitations. One limitation of this study is the relatively homogeneous patient sample in which it was initially validated (Table 3). Further validation efforts would ideally include more diverse patient samples, along with translation to other languages. Additional versions of the table of activities (Table 1) could also be created to reflect appropriate activities for different populations or geographical regions. In addition, 47.1% of respondents were patients at a chronic pain clinic (Table 3), which may have magnified the effect of chronic pain on function, as these patients were seeking specialist treatment for their chronic pain. Another limitation of this study is the effect that recall bias and subjectivity play on patient-reported outcomes.9 Other studies have shown that patient-reported outcomes often slightly underestimate the actual functional capacity.16 Conversely, using that same rationale, if a patient reports a functional capacity of >4 METs on the TFSQ (column C or higher), we can more readily conclude that they are at lower risk of perioperative complications.6 In the same vein, a TFSQ functional capacity of >5 METs (column D or E) aligns with a lower risk of all-cause and cardiovascular-related death.5 A third limitation is that this study only assessed patients’ functional status at 1 point in time. Repeated assessments in the same patients may provide more robust and reliable data. This is 1 reason why trending TFSQ results over time may provide more valuable insight into the patient’s functional status, such as in situations where aberrances in life circumstances may have an undue effect on overall activity.
In summary, the 5-question TFSQ is a novel tool that enhances functional status assessment by establishing a robust yet efficient functional snapshot that is relevant across multiple settings in health care. With this tool, clinicians can quickly assess whether patients has have potential to increase their usual physical activity, and potentially their overall health and well-being,2 by addressing any difference observed between functional performance (TFSQ 1) and capacity (TFSQ 2). In addition, by assessing both components of functional status regularly in preventive care, chronic care, and acute visits, clinicians can monitor for subtle signs of decline and establish the urgency of a referral for rehabilitation, intervention, or specialty referral to avoid permanent disability. The TFSQ may be used with various patient populations across different medical settings. For example, a family medicine physician could use the questionnaire as a tool to track patient functional status longitudinally, and an anesthesiologist might use it as a snapshot of functional status in evaluating a patient’s risk level for surgery.
The TFSQ provides insight into potential reasons for functional decline, such as pain affecting activity (TFSQ 4) or recent acute care (TFSQ 5). It also allows for functional reassessment after an acute event such as hospitalization, trauma, or surgery. It is important to note that the TFSQ is not a substitute for a detailed history and physical examination. However, it may facilitate focusing those efforts on factors that may be limiting a patient’s function and quality of life. To date, we know of no other validated instrument that succinctly measures all of the components assessed on the TFSQ.
Future research and clinical applications for the TFSQ may include preoperative assessment, cardiac rehab, pain management outcomes, and palliative care interventions, where objective documentation of functional status can be beneficial for both care planning and tracking outcomes. It could also be used as a measure of the effectiveness of pain management treatments or other therapies designed to improve overall function. This tool could be used to follow patients throughout their lives, helping to establish goals of care, assess the efficacy of treatments, and engage patients in their care. It may also provide patients with insight into how change in activity, pain, or recent acute care exposure can impact their functional status and prompt educational interventions and motivation for patients to restore their function appropriately. Together, these insights can help patients and clinicians “Focus on Function” when addressing the health needs and goals of individual patients.
Acknowledgments
The authors would like to acknowledge Paul D. Allen, MD, PhD for his contributions to the study design and crafting of the manuscript.
Appendix. Tennessee Functional Status Questionnaire Instrument
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: The authors have no conflicting or competing interests to disclose.
To see this article online, please go to: http://jabfm.org/content/36/1/4.full.
- Received for publication July 29, 2022.
- Revision received October 7, 2022.
- Accepted for publication October 11, 2022.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Response: Re: Developing and Validating a Novel Tool to Enhance Functional Status Assessment: The Tennessee Functional Status Questionnaire (TFSQ)
- Re: Developing and Validating a Novel Tool to Enhance Functional Status Assessment: The Tennessee Functional Status Questionnaire (TFSQ)
- Family Physicians Can/Should Do: What? Where? And How?