
Article Figures & Data
Figures
- Figure 1.
Flowchart of the process to identify eligible studies with reasons for inclusion or exclusion.
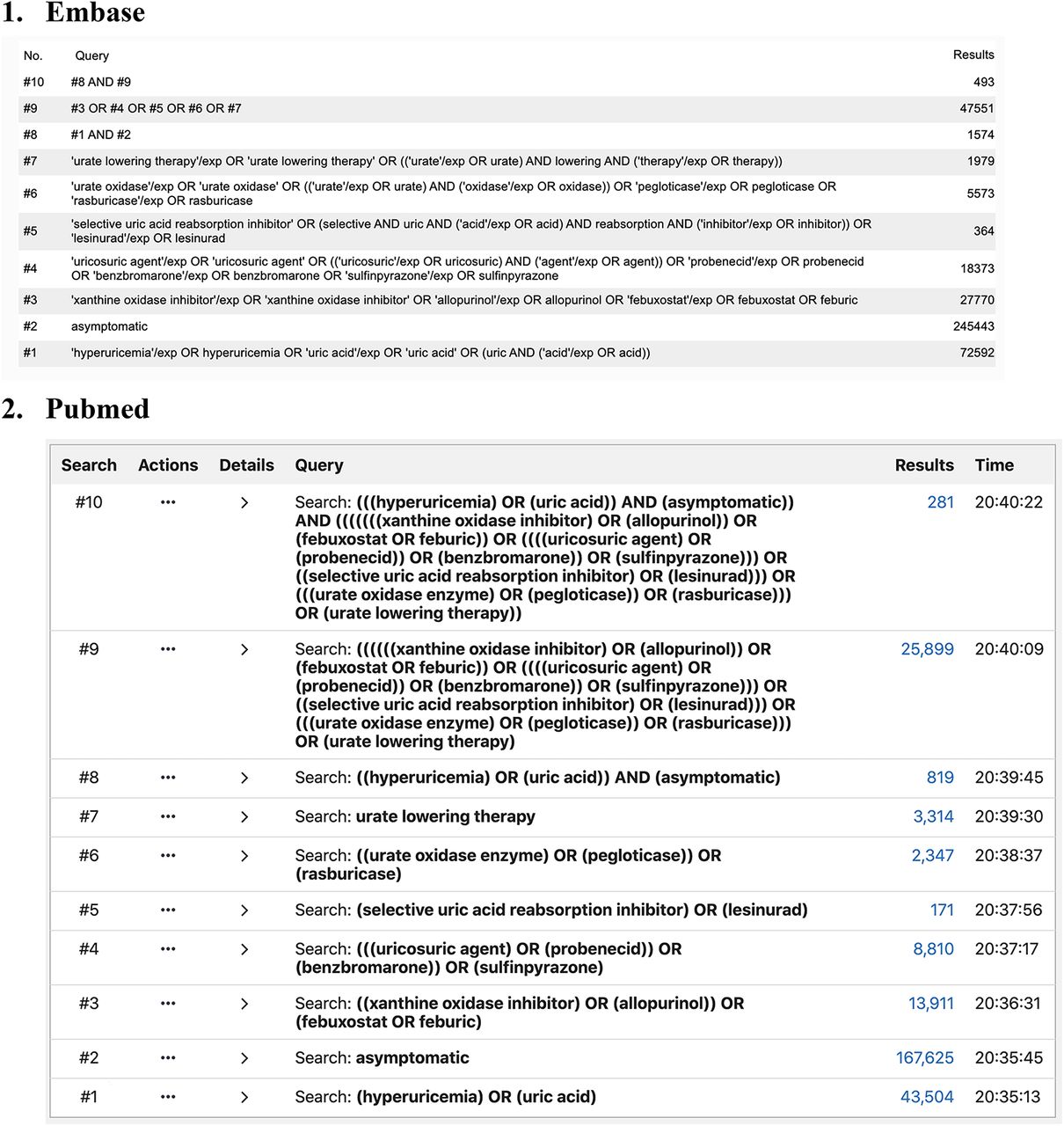
- Appendix 1.
Literature search strategy
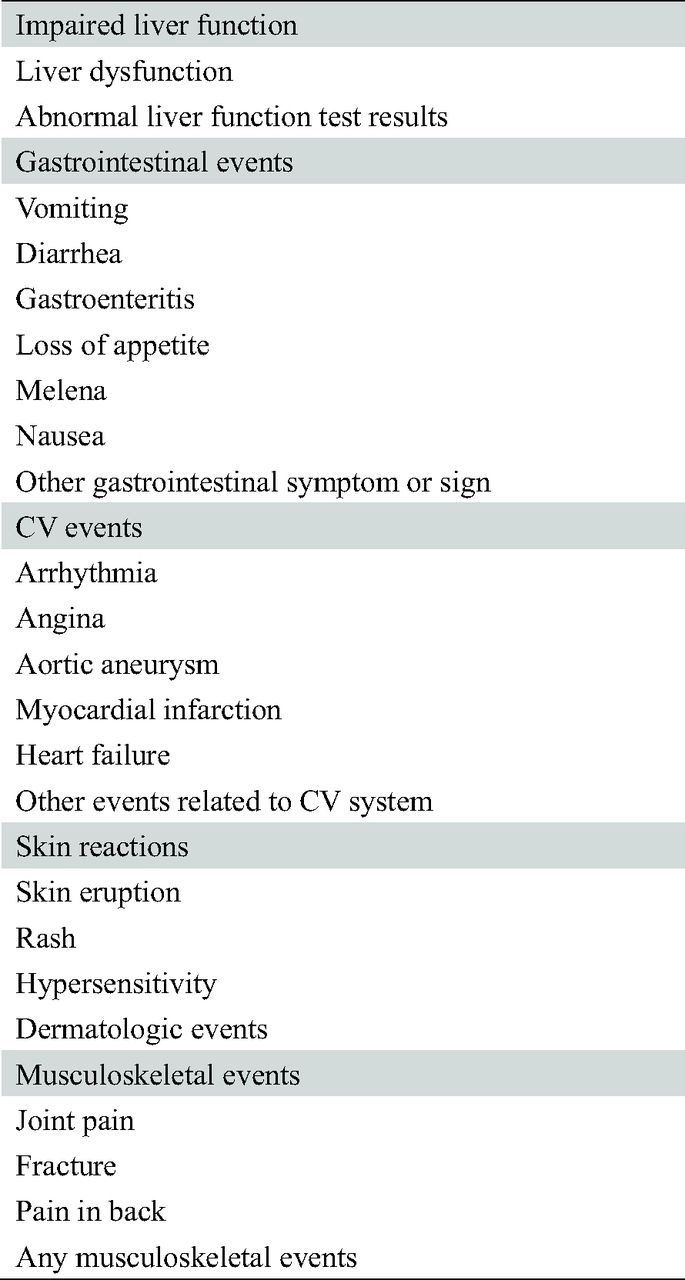
- Appendix 2.
Data extraction from included trials: Details of secondary outcomes
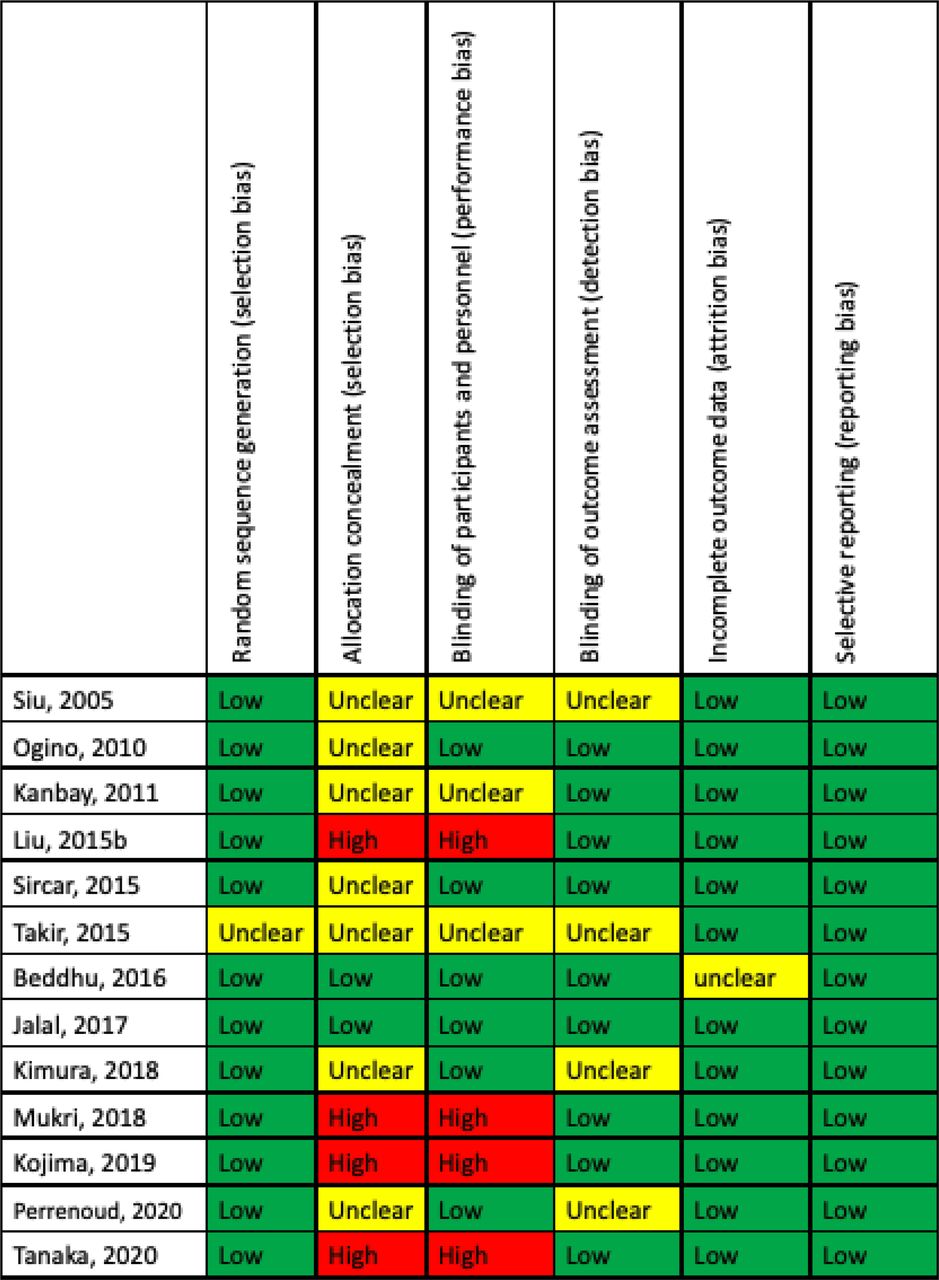
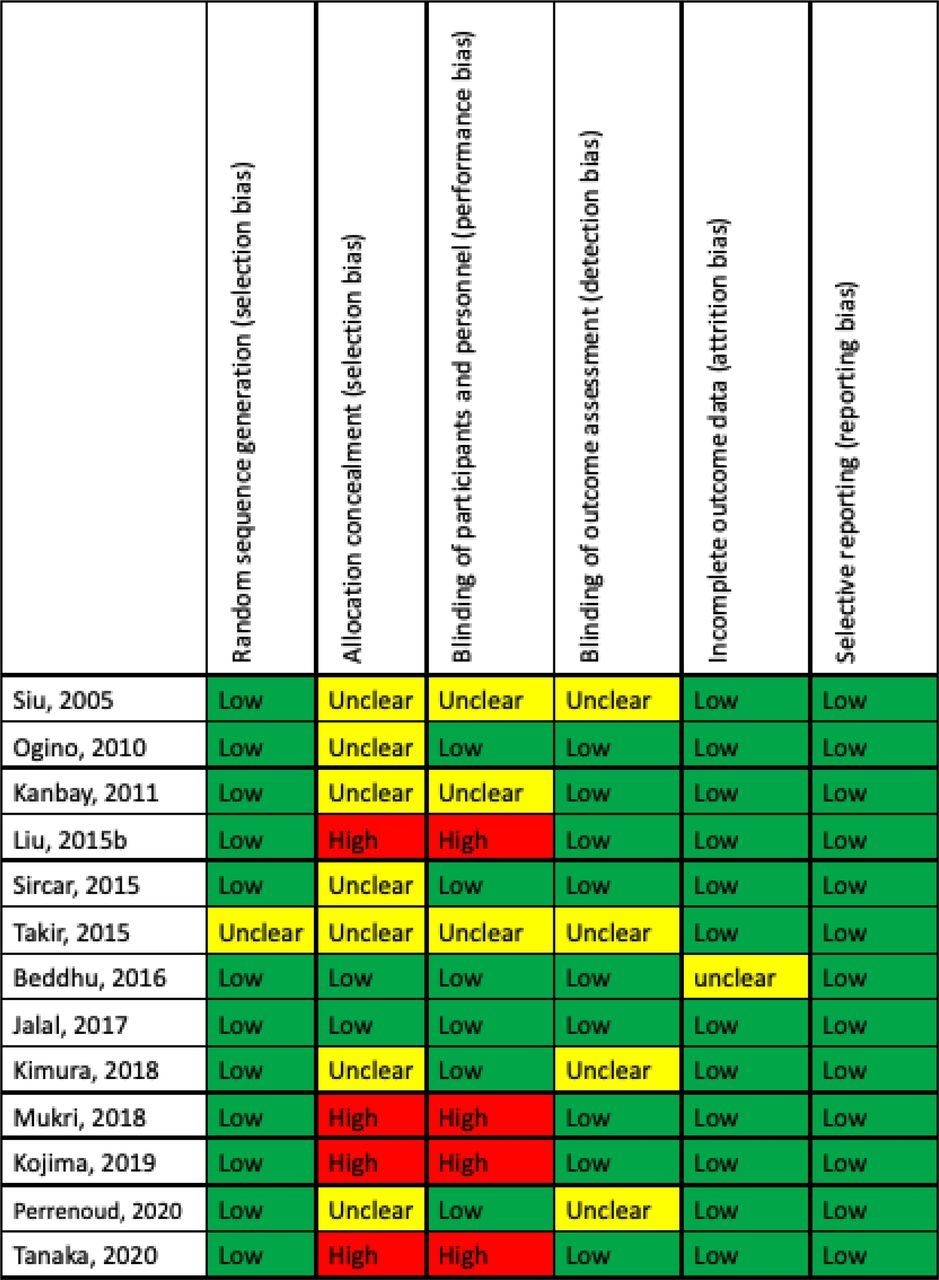
- Appendix 3.
Summary of the risks of bias in every included trial
- Appendix 4.
Network plot for effect of urate-lowering therapy. Each node represents a treatment group, and an edge indicates at least 1 trial comparing the 2 treatments on the ends of the edge. The node size in the network plot is proportional to the number of patients randomized to the treatment group, and the width of an edge is proportional to the number of studies making the pairwise comparison
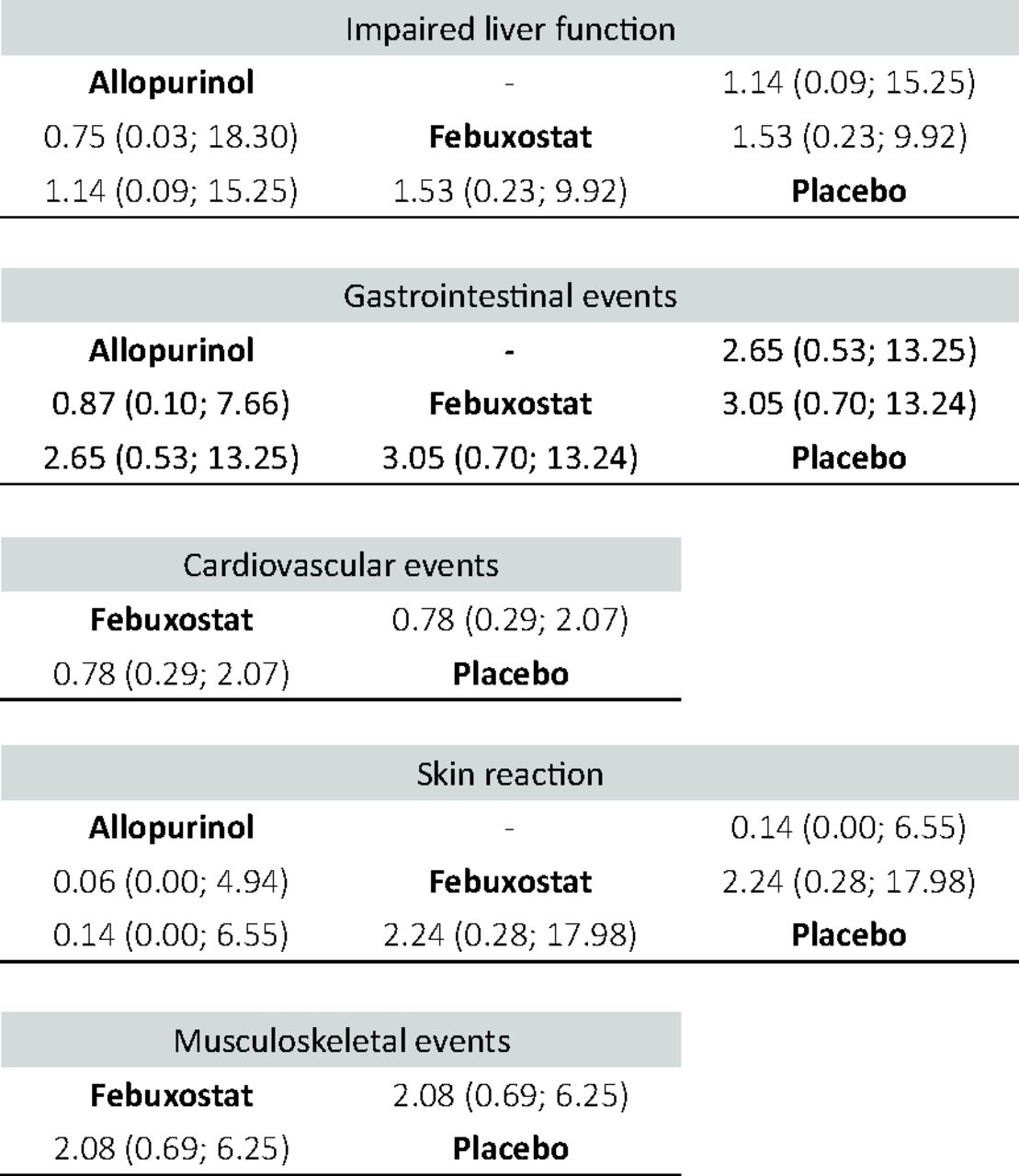
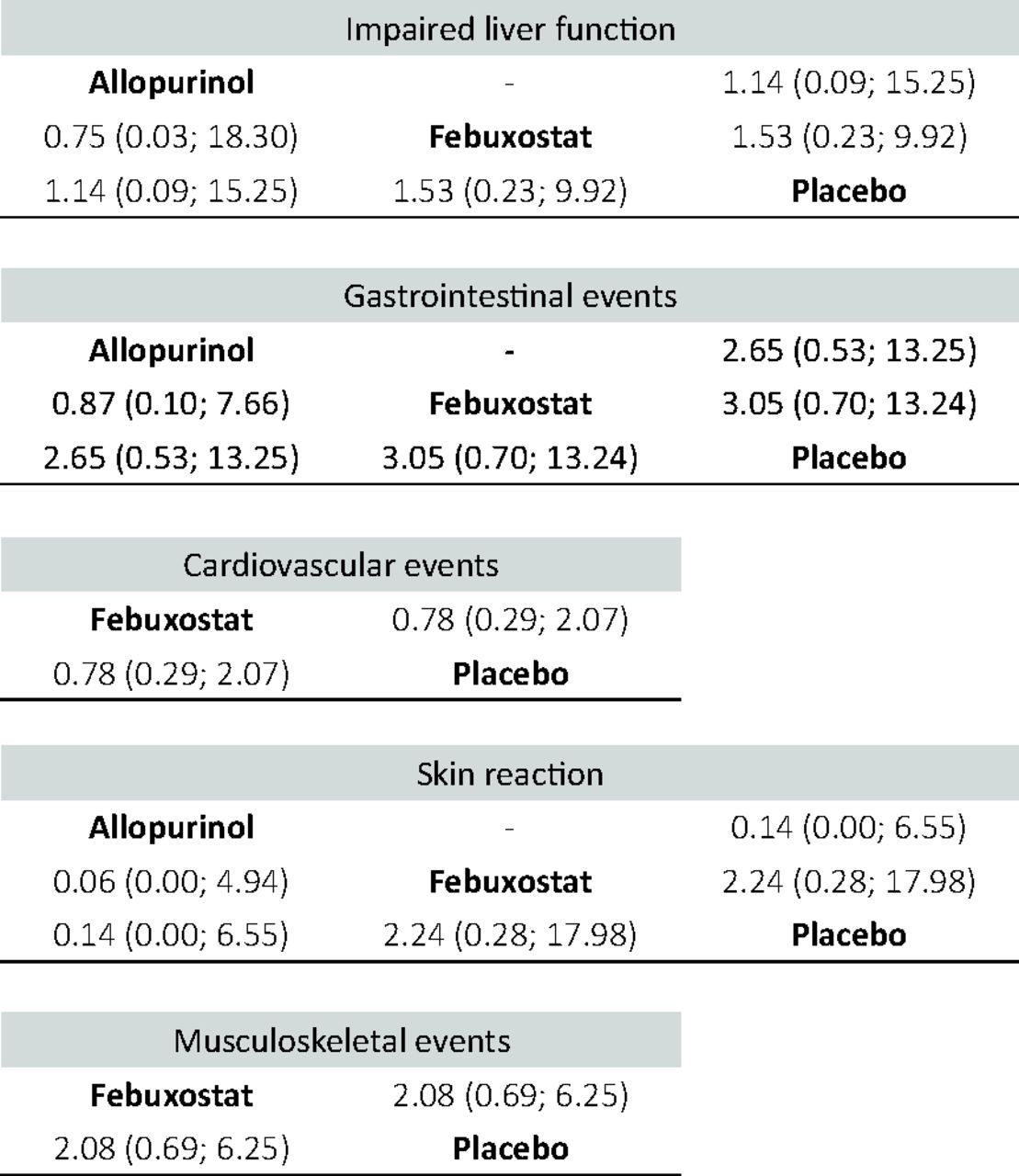
- Appendix 5.
League table of the network meta-analysis comparing the events of secondary outcomes of all drugs, including odds ratios and 95% confidence intervals
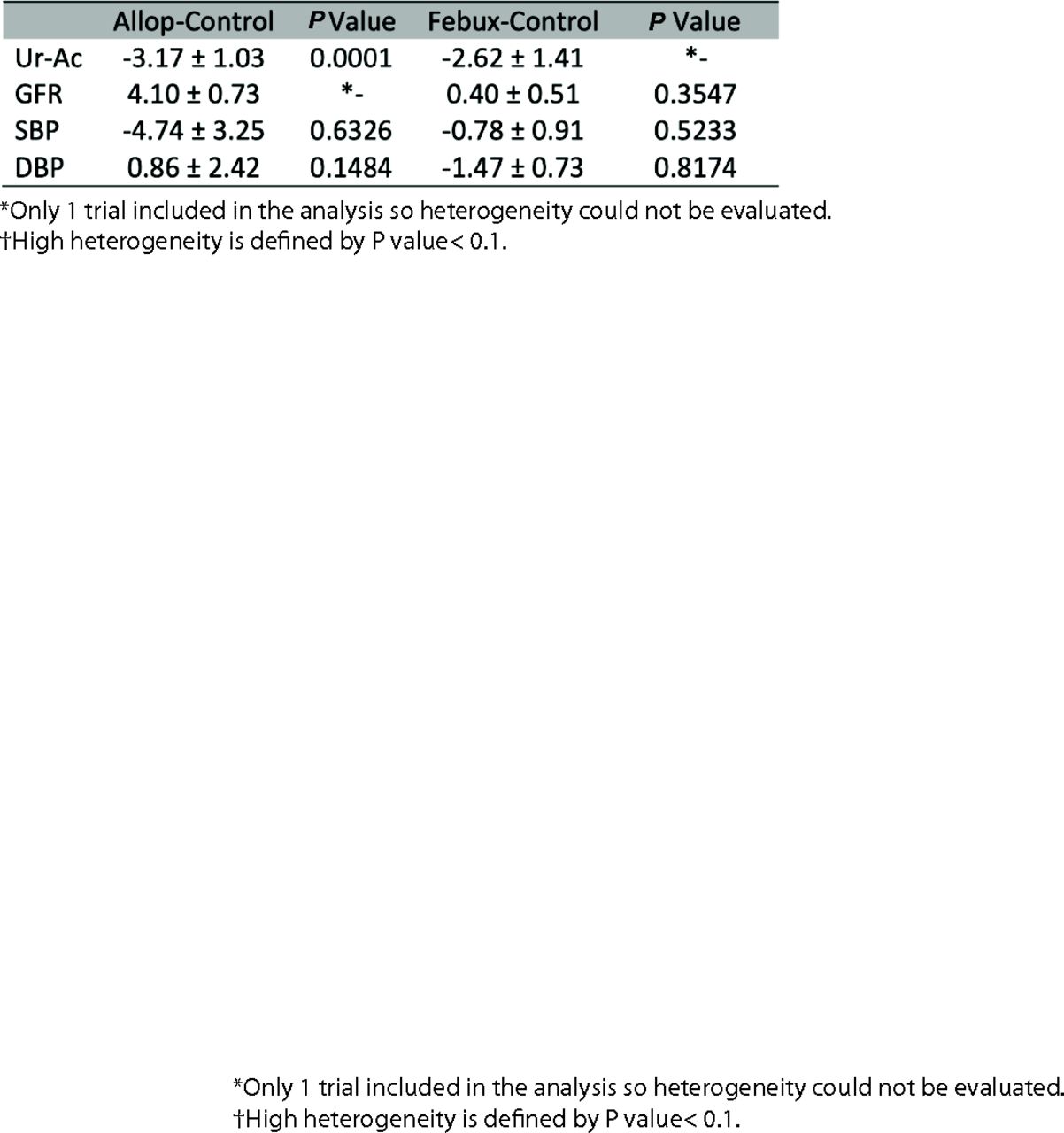
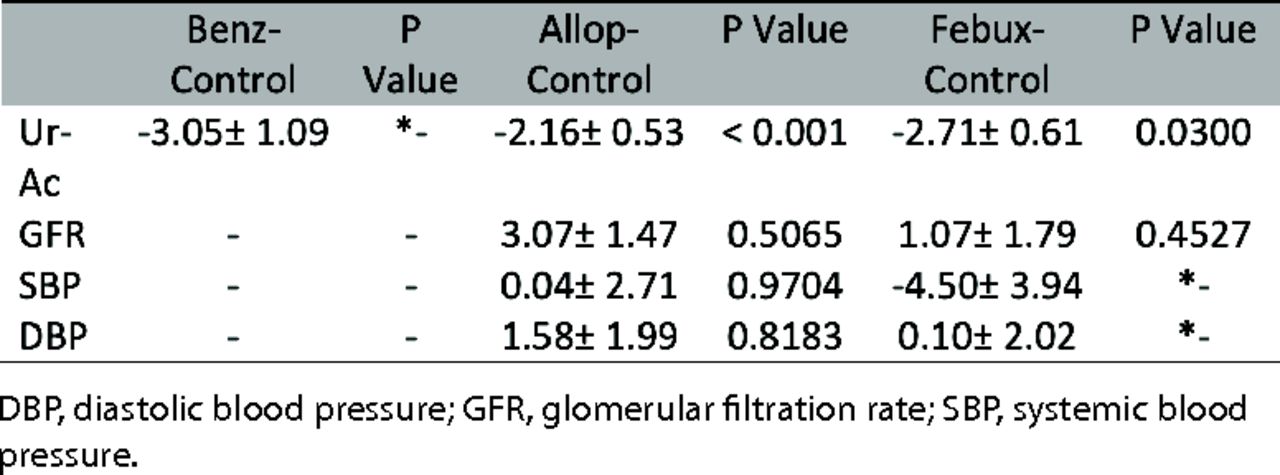
Result of pairwise meta-analyses of all directly compared interventions Appendix 6.1 Results of pairwise meta-analyses of all directly compared interventions of short-term results. P value is obtained from the Cochrane Q test for heterogeneity.
- Appendix 6.2
Results of pairwise meta-analyses of all directly compared interventions of long-term results. P value is obtained from the Cochrane Q test for heterogeneity.






Tables
Author/Country Population Study Design No. of Patients(Treatment/Control) Baseline Characteristic* (Treatment/Control) Treatment Comparison Period(weeks) Primary Outcome Siu, 2005 China28 patients with chronic kidney disease randomized controlled trial 25/26 uric acid (mg/dL): 9.75/5.88 Cr (mg/dL): 1.62/1.86 SBP (mm Hg): 138/135 DBP (mm Hg): 79/71 allopurinol, 100 to 300 mg/day no urate-lowering medical therapy 48 – stable kidney function with less than 40% increase in serum creatinine level
– impaired renal function with creatinine level increase greater than 40% of baseline valueOgino, 2010 Japan29 patients with stable compensated CHF double-blind, placebo-controlled, randomized crossover study 14/14 uric acid (mg/dL): 10.2/10.2 Benzbromarone 50 mg/day placebo 8 – the change of BNP levels
– change in echocardiographic parameters of left ventricle dimensions and LVEFKanbay, 2011 Turkey30 patients with normal renal function randomized, controlled trial 30/37 uric acid (mg/dL): 8.3/7.9†,‡ eGFR: 86.3/84.3 SBP (mm Hg):127.6/123.2 DBP (mm Hg): 75.1/75.6 allopurinol 300 mg/day no urate-lowering medical therapy 16 – endothelial dysfunction
– BP
– eGFRLiu, 2015 China31 patients with type 2 diabetes randomized open parallel-controlled study 88/88 uric acid (μmol/L) : 433/432 eGFR: 90.1/90.1SBP (mm Hg): 121/121 DBP (mm Hg): 74/74 allopurinol starting from 100 mg/day no urate-lowering medical therapy 144 changes in the carotid IMT Sircar, 2015 India32 eastern India aged 18 to 65 years with CKD stages 3 and 4 double-blind, randomized, parallel-group, placebo-controlled study 45/48 uric acid (mg/dL): 9.0/8.2 eGFR: 31.5/32.6 febuxostat 40 mg/day placebo 24 ≥10% decline in eGFR from baseline Takir, 2015 Turkey33 patients without a history of diabetes mellitus, kidney and liver disease randomized, controlled trial 40/33 uric acid (mg/dL): 7.86/7.45 Cr (mg/dL): 0.9/1.07 allopurinol 300 mg/day no urate-lowering medical therapy 12 improvement in insulin resistance defined by homeostatic model assessment of insulin resistance Beddhu, 2016 USA34 overweight or obese adults with type 2 diabetic nephropathy double-blinded randomized controlled trial 37/39 uric acid (μmol/L): 426/422 eGFR: 52.2/54.8SBP (mm Hg): 125.2/128.3DBP (mm Hg): 68.1/72.0 febuxostat 80 mg/day placebo 24 – adipose tissue TBARS and adiponectin concentrations
– urinary transforming growth factor–βJalal, 2017 USA35 ≥ 18 years of age with stage 3 CKD double-blind, randomized, controlled trial 39/41 uric acid (mg/dL): 8.3/8.7 eGFR: 41.3/42.4 SBP (mm Hg): 127/130 DBP (mm Hg): 77.4/77.7 allopurinol 300 mg/day (200 mg, 100 mg) placebo 12 change in brachial artery flow-mediated Dilation Kimura, 2018 Japan36 patients with CKD stage 3 randomizeddouble-blind, parallel-group, placebo-controlled trial 219/222 uric acid (mg/dL): 7.8/7.8eGFR: 45.2/44.9 SBP (mm Hg): 132.5/129.6 DBP (mm Hg): 77.9/77.3 febuxostat (10 mg, 20 mg, 40 mg) placebo 108 eGFR slope Mukri, 2018 Malaysia37 CKD stage 3 and 4 patients with diabetic nephropathy open-label, randomized study 47/46 uric acid (μmol/L): 539.5/537.3 eGFR: 26.2/28.2 SBP (mm Hg): 141/146 DBP (mm Hg): 73.7/71.7 febuxostat 40 mg/day no urate-lowering medical therapy 24 slowing the eGFR decline Kojima, 2019 Japan38 elderly patients who had one or more risks for cerebral, cardiovascular, or renal disease randomized open-label, blinded endpoint study 537/533 uric acid (mg/dL): 7.54/7.50 eGFR: 54.62/55.35 SBP (mm Hg): 132.9/132.3 DBP (mm Hg): 73.5/73.6 febuxostat (10-40 mg/day) non-febuxostat groupno treatment or allopurinol 100 mg (27.2% patients) 144 – fatal and non-fatal cerebral, cardiovascular and renal
– death other than cerebral or cardiorenal vascular diseasePerrenoud, 2020 USA39 patients with CKD stage 3 double-blind randomized placebo-controlled study 39/41 eGFR: 41.4/41.7 SBP (mm Hg): 127/129 DBP (mm Hg): 77/77 allopurinol 300 mg/day placebo 12 – change of albumin-creatinine ratio
– neutrophil gelatinase-associated lipocalin
– kidney injury molecule 1 transforming growth factor β1Tanaka, 2020 Japan40 adults with maximum IMT of the CCA ≥ 1.1 mm at screening randomized, open-label, blinded-endpoint clinical trial 257/257 uric acid (mg/dL): 7.76/7.73 eGFR: 56.26/57.12 SBP (mm Hg): 128.9/127.3 DBP (mm Hg): 73.3/74.18 febuxostat (10-60 mg/day) no urate-lowering medical therapy 96 – percentage change from baseline to 24 months in mean IMT of the CCA Abbreviations: BNP, brain natriuretic peptide; BP, blood pressure; CCA, common carotid artery; CHF, chronic heart failure; CKD, chronic kidney disease; CRP, C-reactive protein; CV, cardiovascular; DBP, diastolic blood pressure; DN, diabetic nephropathy; eGFR, estimated Glomerular filtration rate; FMD, Flow-mediated dilation; IMT, intima-media thickness; IL-6, interleukin-6; LVEF, left ventricular ejection fraction; MCP-1, monocyte chemotactic protein-1; Ox-LDL, oxidized low-density lipoprotein; NF-kB, nuclear factor-kappa B; SBP, systemic blood pressure; TBARS, thiobarbituric acid-reducing substances; UAER, urinary albumin excretion rate.
↵* Values are expressed as mean.
↵† The unit of eGFR is mL/min/1.73 m2.
↵‡ Values are expressed as median.
- Table 2.
League Table of Random-Effects Network Meta-Analysis for Effect of Urate-Lowering Therapy*
Serum Uric Acid Level (Short-Term Follow-Up, mg/dL) Allopurinol . . −2.16 (−3.20 to −1.13) 0.89 (−1.49 to 3.26) Benzbromarone . −3.05 (−5.19 to −0.91) 0.55 (−1.03 to 2.13) −0.34 (−2.79 to 2.11) Febuxostat −2.71 (−3.90 to −1.52) −2.16† (−3.20 to −1.13) −3.05* (−5.19 to −0.91) −2.71† (−3.90 to −1.52) Placebo Serum Uric Acid Level (Long-Term Follow-Up, mg/dL) Allopurinol . −3.17 (−5.19 to −1.15) −0.55 (−3.97 to 2.88) Febuxostat −2.62 (−5.39 to 0.15) −3.17† (−5.19 to −1.15) −2.62 (−5.39 to 0.15) Placebo Renal Function (Short-Term Follow-Up, mL/min/1.73 m2) Allopurinol . 3.07 (0.18 to 5.95) 2.00 (−2.54 to 6.53) Febuxostat 1.07 (−2.43 to 4.57) 3.07† (0.18 to 5.95) 1.07 (−2.43 to 4.57) Placebo Renal Function (Long-Term Follow-Up, mL/min/1.73 m2) Allopurinol . 4.10 (2.66 to 5.54) 3.70† (1.94 to 5.46) Febuxostat 0.40 (−0.60 to 1.40) 4.10† (2.66 to 5.54) 0.40 (−0.60 to 1.40) Placebo Systolic Blood Pressure (Short-Term Follow-Up, mm Hg) Allopurinol . 0.04 (−4.22 to 4.30) 4.54 (−4.29 to 13.37) Febuxostat −4.50 (−12.23 to 3.23) 0.04 (−4.22 to 4.30) −4.50 (−12.23 to 3.23) Placebo Systolic Blood Pressure (Long-Term Follow-Up, mm Hg) Allopurinol . −4.74 (−11.12 to 1.63) −3.96 (−10.58 to 2.66) Febuxostat −0.78 (−2.57 to 1.01) −4.74 (−11.12 to 1.63) −0.78 (−2.57 to 1.01) Placebo Diastolic Blood Pressure (Short-Term Follow-Up, mm Hg) Allopurinol . 1.58 (−2.31 to 5.48) 1.48 (−4.06 to 7.03) Febuxostat 0.10 (−3.85 to 4.05) 1.58 (−2.31 to 5.48) 0.10 (−3.85 to 4.05) Placebo Diastolic Blood Pressure (Long-Term Follow-Up, mm Hg) Allopurinol . 0.86 (−3.88 to 5.61) 2.34 (−2.62 to 7.29) Febuxostat −1.47 (−2.90 to −0.04) 0.86 (−3.88 to 5.61) −1.47† (−2.91 to −0.04) Placebo SHORT-TERM LONG-TERM Serum Uric Acid Serum Uric Acid Benzbromarone 0.7908 Allopurinol 0.8108 Febuxostat 0.7146 Febuxostat 0.6728 Allopurinol 0.4937 Placebo 0.0164 Placebo 0.0009 Renal Function Renal Function Allopurinol 1.0000* Allopurinol 0.8937 Febuxostat 0.3912 Febuxostat 0.4598 Placebo 0.1088 Placebo 0.1465 Systolic Blood Pressure Systolic Blood Pressure Allopurinol 0.9035* Febuxostat 0.8581 Febuxostat 0.4626 Allopurinol 0.3246 Placebo 0.1340 Placebo 0.3173 Diastolic Blood Pressure Diastolic Blood Pressure Febuxostat 0.9000 Placebo 0.6534 Placebo 0.3307 Febuxostat 0.5900 Allopurinol 0.2693 Allopurinol 0.2567 ↵* Large value of P-score (eg, >0.90) may reflect that treatment is quite certain to be the most efficacious or safest.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Development, validation and economic evaluation of a machine learning algorithm for predicting the probability of kidney damage in patients with hyperuricaemia: protocol for a retrospective study
- Response: Re: To Treat or Not to Treat? Effect of Urate-Lowering Therapy on Renal Function, Blood Pressure and Safety in Patients with Asymptomatic Hyperuricemia
- Re: To Treat or Not to Treat? Effect of Urate-Lowering Therapy on Renal Function, Blood Pressure and Safety in Patients with Asymptomatic Hyperuricemia
- Health Care Equity for Family Medicine Patients and Family Physician Equity