
Abstract
Background: Disruptions in primary care practices, like ownership change, clinician turnover, and electronic health record system implementation, can stall quality improvement (QI) efforts. However, little is known about the relationship between these disruptions and practice participation in facilitated QI.
Methods: We explore this relationship using data collected from EvidenceNOW in a mixed-methods convergent design. EvidenceNOW was a large-scale facilitation-based QI initiative in small and medium primary care practices. Data included practice surveys, facilitator time logs, site visit field notes, and interviews with facilitators and practices. Using multivariate regression, we examined associations between disruptions during interventions and practice participation in facilitation, measured by in-person facilitator hours in 987 practices. We analyzed qualitative data on 40 practices that described disruptions. Qualitative and quantitative teams iterated analyses based on each other's emergent findings.
Results: Many practices (51%) reported experiencing 1 or more disruptions during the 3- to 15-month interventions. Loss of clinicians (31.6%) was most prevalent. In adjusted analyses, disruptions were not significantly associated with participation in facilitation. Qualitative data revealed that practices that continued active participation were motivated, had some QI infrastructure, and found value in working with their facilitators. Facilitators enabled practice participation by doing EHR-related work for practices, adapting work for available staff, and helping address needs beyond the explicit aims of EvidenceNOW.
Conclusions: Disruptions are prevalent in primary care, but practices can continue participating in QI interventions, particularly when supported by a facilitator. Facilitators may benefit from additional training in approaches for helping practices attenuate the effects of disruptions and adapting strategies to help interventions work to continue building QI capacity.
- Family Medicine
- Health Personnel
- Health Services Research
- Primary Health Care
- Qualitative Research
- Quality Improvement
- Surveys and Questionnaires
- Workforce
Background
Primary care medicine in the United States has experienced significant transformations over the past 2 decades due to new federal and state policies and recommendations,1⇓⇓–4 evolving care delivery models and frameworks,5⇓⇓⇓⇓⇓⇓⇓–13 technological innovations,6,14 and revised payment structures.15⇓⇓⇓–19 These changes have increased the need for quality improvement (QI): planning, monitoring, and adjusting workflows to new evidence-based practices; using electronic health records (EHRs) to identify and resolve care gaps; and measuring performance concerning clinical guidelines, stakeholder mandates, and incentives.20⇓⇓⇓⇓–25 To stay viable in today's landscape, primary care practices need to develop the ability to adapt quickly and embrace continual change.26,27
Thus far, making rapid and sustained change has been difficult for primary care practices,28⇓⇓⇓⇓–33 particularly small independent practices lacking financial and staff resources.34⇓⇓⇓⇓–39 Health system buy-outs, new affiliations, location changes and mergers, and new EHR implementations can disrupt staff, team structures, and workflows. Clinician and staff turnover has also risen in recent years,40⇓⇓⇓–44 creating discontinuities in leadership and basic practice operations.
Researchers and QI organizations recognize the need for external support to help practices implement QI within this environment.45⇓⇓–48 Practice facilitation (henceforth, facilitation) has arisen to do this.49⇓⇓⇓⇓⇓⇓⇓–57 However, facilitators and researchers alike note that practice disruptions like turnover, EHR implementation, and ownership or leadership change can present serious obstacles to practices' engaging in facilitation and QI.39,58⇓⇓⇓⇓–63 In particular, pervasive turnover44,64,65 is noted as highly disruptive for team building and retaining institutional knowledge, reducing the capacity and motivation of remaining staff to do QI.66
Few studies, though, have systematically examined the prevalence and impact of different types of disruptions on practices' participation in facilitated QI.61,67 We examine qualitative and quantitative data from EvidenceNOW, an Agency for Healthcare Research and Quality (AHRQ) national initiative to improve primary care practices' capacity for QI and cardiovascular preventive care delivery, to explore the independent and cumulative effects of disruptions on practices' abilities to participate in facilitation-based QI interventions.
Methods
Setting
AHRQ funded 7 Cooperatives across the United States for the EvidenceNOW initiative. Each Cooperative implemented multiple support strategies during an intervention to increase practice capacity for QI and improve cardiovascular preventive care as measured through the “ABCS of heart health”:68 prescribing Aspirin when appropriate, controlling Blood pressure, managing Cholesterol, and providing Smoking cessation counseling.69 Cooperatives collectively enrolled 1721 primary care practices, each enrolling between 208 and 276 sites.70 Practices varied in ownership, but most comprised 10 or fewer clinicians (see Table 1). Cooperatives varied in their intervention designs, including use of change models, length of interventions (3 to 15 months), facilitation models, and expected number of facilitator visits;56 intervention designs are reported elsewhere,71⇓⇓⇓⇓–76 but all used facilitators to support intervention goals.77 AHRQ funded our independent national evaluation team, ESCALATES (Evaluating System Change to Advance Learning and Take Evidence to Scale), to assess lessons across Cooperatives.
Practice Characteristics
Data Collection and Analysis
For this study, we used multiple types and sources of quantitative and qualitative data collected by the Cooperatives and the ESCALATES team in a mixed-methods convergent design. We iteratively conducted mixed-methods analysis: emergent qualitative findings informed hypotheses and variables for quantitative modeling, and quantitative findings provoked additional qualitative analyses.
Quantitative Data Collection
Cooperatives administered 2 types of surveys. The Practice Survey, answered by 1 practice leader (office manager, practice owner, or lead clinician), included questions about practice size, ownership, location, and past participation in demonstration projects. This survey also asked if the practice had experienced a “major change,” providing a list of 6 potential disruptions and a write-in response (see Figure 1).
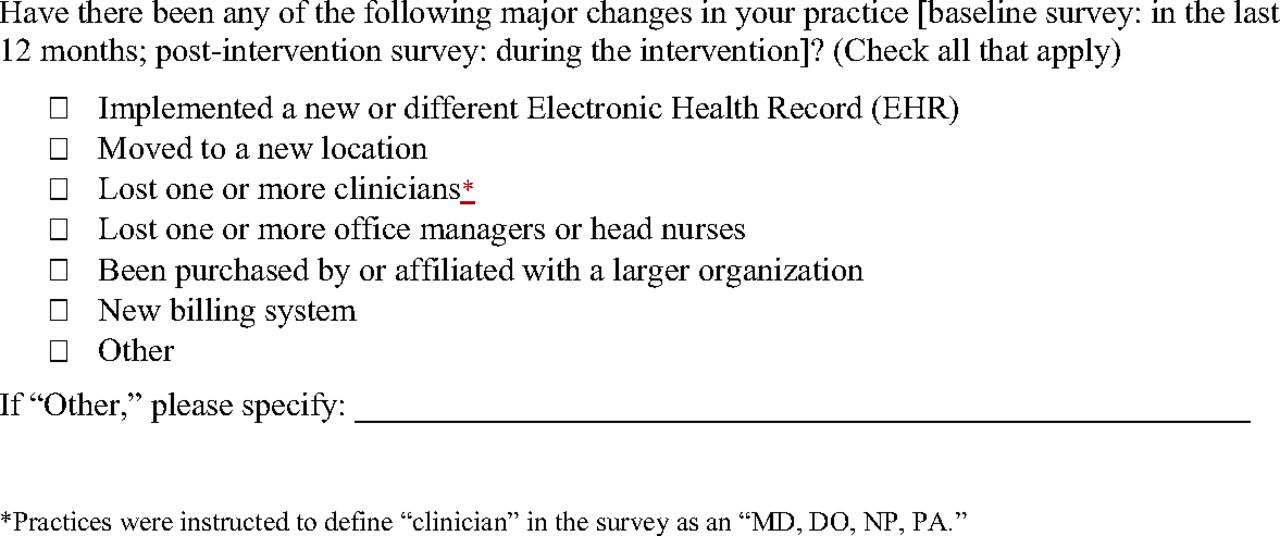
Practice Survey Question About Disruptions.
Cooperatives also administered confidential Practice Member Surveys to multiple employees within each practice. This survey included the 18-item Adaptive Reserve questionnaire, assessing leadership and teamwork qualities associated with practice adaptation and resilience.78,79
Both surveys were administered at baseline (9/2015 to 3/2017) to assess the year before the intervention and post-intervention (11/2016 to 12/2017) to assess the intervention time frame. Survey administration (article, web-based, phone), incentive type (cash, gift card), and incentive amount ($2-$75) varied across Cooperatives.
Facilitators kept logs across the intervention time frame to record the hours and mode (in-person, phone, or web) they worked with and in the practice.
Quantitative Analysis
We drew the primary independent variable, occurrence of types of disruptions during the intervention, from the post-intervention Practice Survey. We operationalized participation in facilitation, our outcome variable, as logged total hours of in-person facilitator time per practice. Our thinking was that practices would divert time from facilitation participation to managing disruptions if practice operations were unduly stressed. Covariates of practice size and ownership, geographic location, participation in other demonstration projects, occurrence of disruptions before the intervention, and Adaptive Reserve were obtained from baseline Practice and Practice Member Surveys. We dichotomized practices' Adaptive Reserve scores into the top 25% (scores of 0.78 and above) versus the bottom 75%, hypothesizing that practices with higher scores would be better able to continue interventions despite disruptions. We included whether or not disruptions occurred before EvidenceNOW to control for ongoing effects of past disruptions.
We used frequencies to describe practice characteristics and participation in facilitation per Cooperative (see Table 1). To explore the relationship between disruptions and participation in facilitation, we performed a series of multivariable regressions, presenting estimated marginal means in hours. To account for Cooperative differences in intervention design and length, we used a generalized estimating equation (GEE) model with a γ distribution; this model accounts for clustering by Cooperative to give accurate estimates of the number of hours practices spent in facilitation and association with the selected independent variables.
For disruptions during the intervention, we examined associations between participation in facilitation with each disruption type; with the number of disruption types experienced (0, 1, 2, and 3+); and with having 1 or more types of disruptions. We collapsed “being purchased by or affiliated with a larger organization” (n = 34) and “moving to a new location” (n = 79) into 1 category representing organizational disruptions. We collapsed “implemented a new or different EHR” (n = 160) and “new billing system” (n = 120) into a category representing information system disruptions. We recoded “Other” (n = 139) responses into the above categories when applicable. We did not include remaining write-in responses because descriptions were highly variable (see Appendix Table 1). We conducted sensitivity analyses using different definitions of practice participation in facilitation to ensure the reliability of our findings (see Appendix, Table 4). Statistical software included R version 4.0.0 and Stata version 15.1.
Qualitative Data Collection
ESCALATES collected interview and observational data throughout EvidenceNOW. During interventions, we shadowed 44 facilitators at 62 practices across the 7 Cooperatives. Cooperatives selected the facilitators and practices for us to observe. We wrote field notes from these site visits and interviewed 41 facilitators about 54 practices. Post-intervention, we sampled practices that had improved in at least 1 ABCS and/or had unique characteristics. We interviewed 66 practice members and 74 facilitators about their work in 110 of these practices. Altogether, the ESCALATES team collected qualitative data on 158 practices. Interviews were audio-recorded and professionally transcribed. Qualitative data were managed in Atlas.ti 7 Windows.
Qualitative Data Analysis
A team of analysts (JRH, AB, JDH, CP) read interviews and field notes for each of the 158 practices, identifying practices that had descriptions of the disruptions specified in the Practice Survey. Because medical assistants (MAs) were integral to EvidenceNOW intervention work, we included MA loss as a disruption. This team met weekly to analyze data, reading, and discussing key passages together. We wrote practice summaries and identified patterns in how and why disruptions affected participation in facilitation.
Results
Practice Characteristics and Reported Disruptions
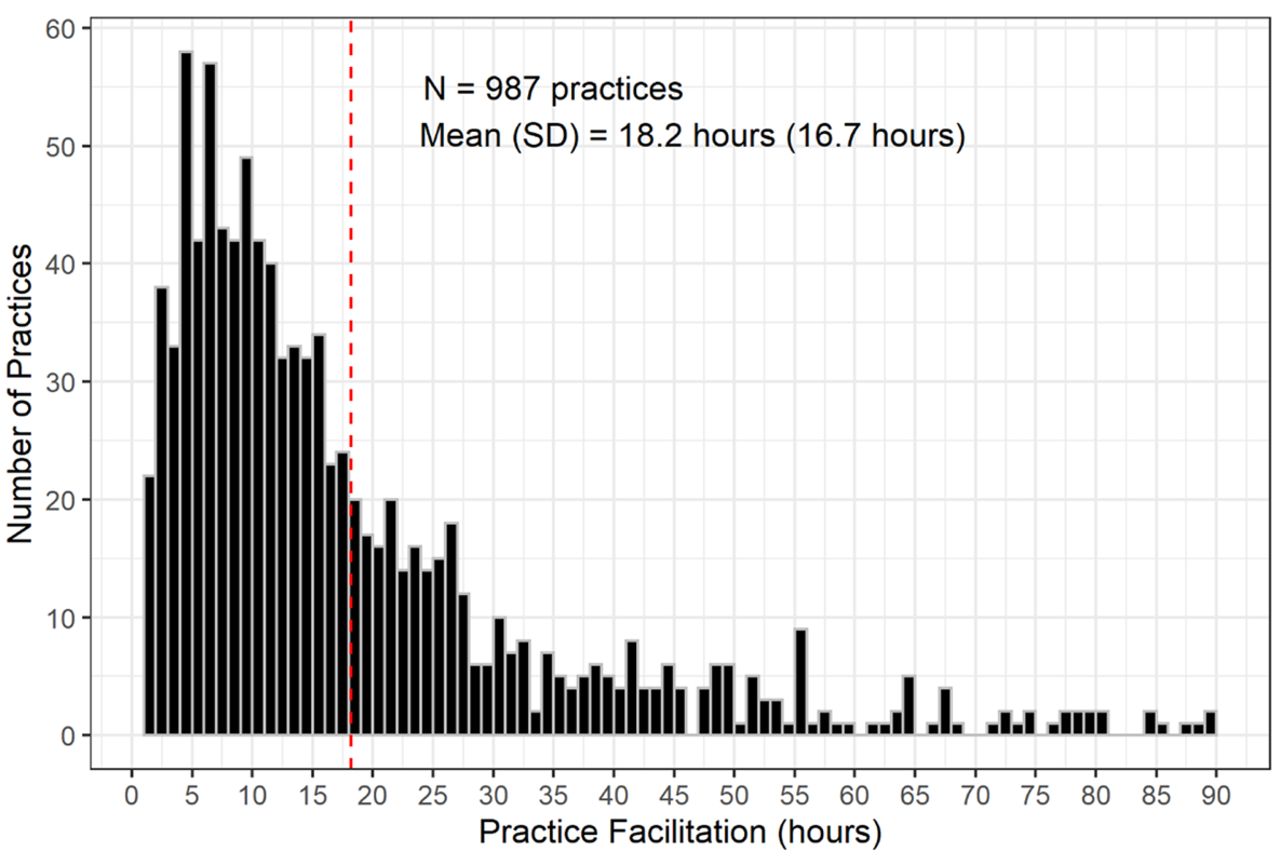
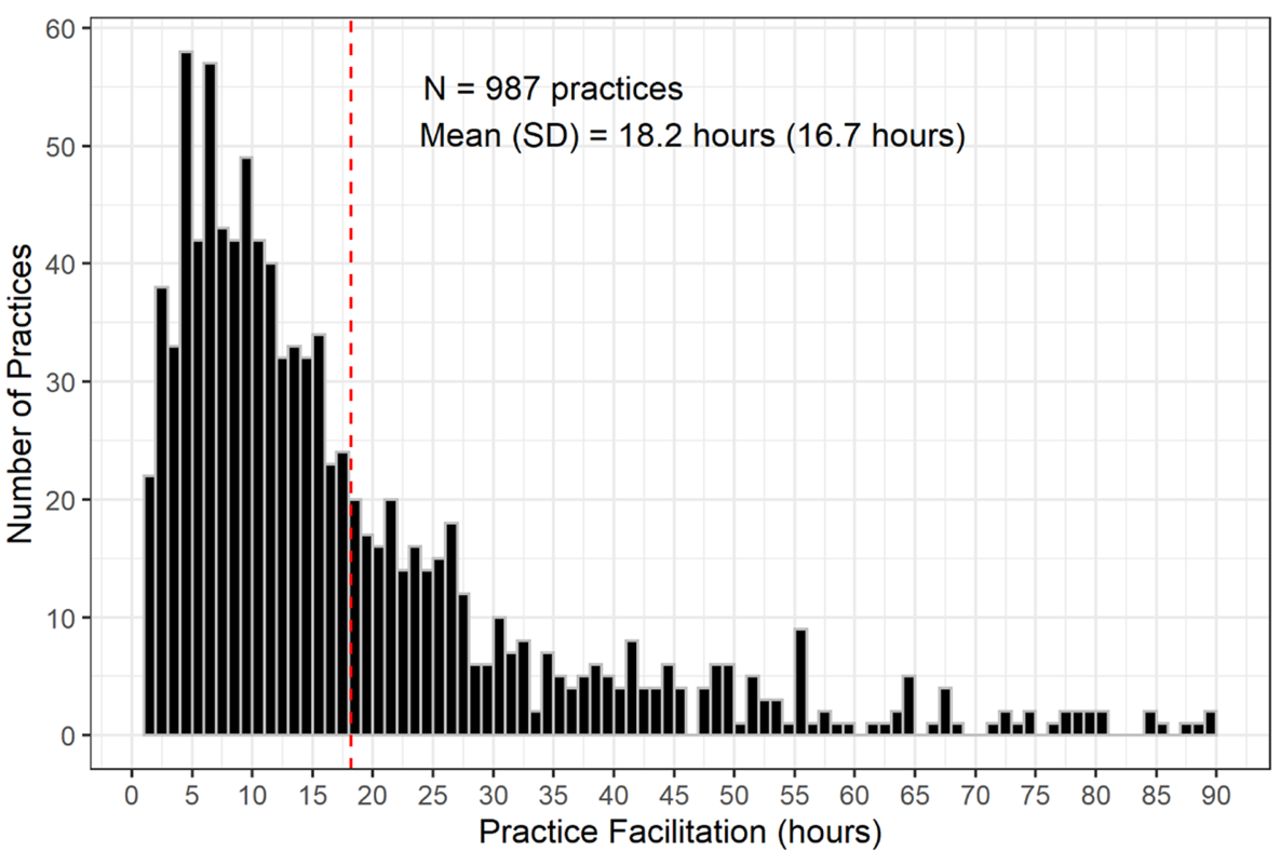
Of the 1721 practices enrolled in EvidenceNOW at baseline, 987 (57.4%) had complete data from baseline and follow-up surveys and between 1 and 90 hours of facilitation participation (see Appendix Figure 1). Practices varied in size and ownership, but most were located in an urban core and had not participated in a demonstration project previously. Practices, on average, participated in 18.2 hours of facilitation (SD = 16.7). (See Table 1.)
Just over half of practices that completed the surveys reported at least 1 disruption both before and during the interventions (see Table 2), with one-third of these reporting 2 or more disruptions. The most common disruptions were loss of clinician(s) or office manager/head nurse(s), both of which happened more frequently during the intervention than pre-intervention.
Disruptive Events Reported by Practices Before and During EvidenceNOW Interventions
In our interview data and field notes, practice members or facilitators described disruptions in 40 of 158 practices. More than half of these practices were described as experiencing multiple types of disruption. Loss of personnel—clinicians, office managers/head nurses, or MAs—were described more often than organizational or information system disruptions.
Disruptions' Effects on Practice Participation in Facilitation
In quantitative models, practices that reported 1 or more disruptions during their intervention did not differ significantly in participation in facilitation from practices that did not report disruptions. Furthermore, participation in facilitation did not vary significantly by type or number of disruption types reported. (See Table 3; Appendix Table 2.) Neither Adaptive Reserve nor prior participation in demonstration projects was associated with participation in facilitation (Appendix Table 3).
Association of Disruptive Events During Intervention with Participation in Facilitation
Qualitatively, we found that disruptions had differing effects on practices' abilities to participate in facilitation. Some practices decreased or stopped participation in facilitation when disruptions occurred, particularly when they had only 1 person responsible for QI and this person left the practice. However, other practices that experienced similar types or numbers of disruptions continued facilitation. Practices that sustained participation in facilitation through disruptions shared several key attributes: they exhibited high motivation to do the intervention or some degree of preexisting QI infrastructure, and they were able to normalize disruptions as part of the work environment. In addition, practices that found value in their facilitator were likely to continue participating in facilitation despite, and sometimes because of, disruptions. Facilitators' approaches to working with practices appeared to influence practices' abilities to maintain participation, as well.
QI Motivation and/or QI Infrastructure
Practices that continued participating in facilitation during disruptions had specific goals they wanted to achieve through EvidenceNOW. Some of these practices were energized by embarking on QI or felt pressure to catch up on innovations or evidence-based learnings; others had well-established QI routines. Having specific reasons for joining the intervention bolstered participation regardless of QI experience, but practices with QI experience benefited from the stability of set monthly meetings, QI teams, and QI roles. Practices with an engaged QI team, rather than a single QI contact, were less vulnerable to negative turnover effects on participation:
[T]hey're a great clinic to work with, … [T]hey've been doing a lot of practice transformation… .[T]hey already had QI team put together. They were dedicated to actually work on the things we talked about in between sessions…. At the time we were doing this, they were in the process of losing three [providers] and gaining another three…. I don't really feel like they let that affect their work in this project too much…. [T]he QI team was very dedicated. (Facilitator interview, Cooperative 6)
Normalizing Disruptions
Some practices accepted disruptions as an inevitable part of practice operations. Practices with consistent staff turnover adjusted to working with capacity gaps. Others realized that they needed to work on QI despite disruptions to avoid penalties or lost incentives, falling behind in evidence-based practices, or patient dissatisfaction. Practices that prioritized QI goals or committed to getting work “done” learned how to work around disruptions. For example, this practice experienced clinician loss and MA turnover during the intervention:
For the satellite office, [turnover is] not anything new. For the main location, it has been something new…. We had to pull people from this location to help the other location. That's why it's been a rat race.
Interviewer: Yeah. Do you think that's influenced your ability to work on [EvidenceNOW] at all?
CMA: I don't think so, because it's—things that we have to get done, it just means that you have to learn to multi-task and communicate more with your co-workers to fill in the gaps. (CMA/Health Education Specialist interview, Cooperative 1)
Valued Facilitators
Facilitators fulfilled a variety of functions for practices. Practices with long-term facilitator relationships appreciated being accountable to someone they trusted. Practices new to QI often felt beholden to facilitators for the skills, tools, information, and support they delivered. Practices that continued participation in facilitation continued receiving these benefits, particularly important to some during times of disruption. For example, 1 clinician-owner who had several staff leave appreciated that his long-term facilitator could help train the new staff: “She works with our staff, and she really gives us a lot of help. It is like we have an extra manager help us” (Clinician Owner Interview, Cooperative 3). Another practice's administrator appreciated their facilitator's persistence despite office manager and staff turnover: “[C]oming in and meeting as a group and then also coming through individually was really good…. [S]he was persistent about being here [and] making sure she made contact with… all the different people here. [H]aving [information] repeated all the time… was really helpful” (Practice Administrator interview, Cooperative 7).
Facilitators' Approaches to Working with Practices During Disruptions
Facilitators used approaches that encouraged and, in some cases, enabled practices experiencing disruptions to continue their participation in facilitation. For example, facilitators focused on helping practices improve their ABCS performance often did basic EHR work for the practice: facilitators scheduled reminders, produced data reports, called EHR vendors to map out workflows, redesigned templates, and conducted chart audits. Facilitators described doing this kind of work to enable the practice to work on higher-order practice changes:
Turnover [has been] huge…. [T]hey've had actually three different office managers throughout the intervention…. Now we have this one office manager that's sort of been with them for a while…. [But] when I try to bring up, “Hey, can you run these reports?” she looks at me like to say, “I really like working with you, but I can't take any more work”…. For now, [I'm running the reports]…. I'm willing to take a few extra steps for them…. [T]hen when I need them to do something for me, they perform in return…. [S]ometimes that is also the incentive…. (Facilitator interview, Cooperative 3)
Other facilitators focused on helping practices build QI capacity rather than doing work for the practice; they adapted intervention work to the situation by limiting the scope of PDSAs and aligning goals to help leverage other QI projects. If practices lost personnel, facilitators focused on work those remaining could do. When teams felt overwhelmed, facilitators paused work to give practices time to rebuild capacity. Sometimes, facilitators leveraged disruptions to improve leadership-staff dynamics or streamline workflows. These facilitators viewed progress as a long-term process and adjusted accordingly. For example, this facilitator helped her practice continue participation despite losing a head nurse and MA during the intervention:
The office manager tells the facilitator that they've been doing huddles to see who is high-risk…. [B]ecause of hiring and turnover, the office manager hasn't had a chance to change the test group of patients. (This practice started by focusing on 8 hypertensive patients and planned to slowly add more). The facilitator tells her, “That's OK!” The facilitator asks, “So how are you going to reach out to these patients?” The office manager thinks for a moment and then suggests they do a mailing. The facilitator asks her if she thinks [the business office] could just do five mailings a day, 25 a week. The office manager thinks that sounds doable. They walk through the workflow…. (ESCALATES Site Visit Fiel dnotes, Cooperative 1)
To retain practice engagement, sometimes facilitators helped practices work on projects outside explicit EvidenceNOW goals. For example, facilitators helped practices with incentive programs like Meaningful Use or broader issues like high emergency department (ED) use, transportation needs, food scarcity, substance use disorders, and mental health needs. Facilitators attempted to address practice priorities, sometimes by merging them with EvidenceNOW-specific goals, but often working on these needs in parallel or before their EvidenceNOW agenda. In the following example, the clinician-owner lost a clinician and much of his MA staff. The facilitator focused on priorities the clinician outlined:
We worked some on ED utilization and just doing callbacks for patients that had ED visits… some other things that he was really interested in, too, that weren't specifically related to [EvidenceNOW]… around his populations that have behavioral health substance abuse problems…. [S]ome of them have chronic conditions such as hypertension… and he didn't [know] where to refer them. We worked on that as well as kind of an aside, but really tied [that] into providing good comprehensive care for his high-risk patients, too. (Facilitator interview, Cooperative 6)
Discussion
EvidenceNOW findings affirm that disruptions are a reality across primary care practices, particularly the high turnover of key personnel. Nevertheless, and to our surprise, quantitative analyses revealed little evidence that any particular type of disruption, or even multiple disruptions, affected practices' abilities to participate in facilitation aimed at building QI capacity to achieve cardiovascular care goals. Qualitative analyses may help explain these unexpected results. We found that practices with specific motivations to participate in EvidenceNOW and/or preexisting QI infrastructure continued participating in facilitation while experiencing disruptions. Accepting disruptions as an inevitable part of their work also seemed to moderate the disruptive impact of disruptions. In addition, facilitators encouraged and, in some cases, enabled practices to continue participating in facilitation by doing EHR-related work, adapting QI work to available staff, and helping them make progress toward patient care goals beyond stated aims of EvidenceNOW. In fact, disruptions may have impelled some practices to continue working with facilitators to receive these highly valued benefits. Facilitators used these approaches to engage practices not experiencing disruptions, as well;80,81 however, these approaches may have been especially important for practices experiencing high levels of disruption that needed extra support.
It is also possible that these types of disruption are not as disruptive as they once were. For instance, implementing a new EHR was a paradigm shift a decade ago, but most practices are now upgrading already-existing EHRs; they may know from previous experience what to expect, how to prepare, and where to receive support.59,82 Clinician and staff loss may also not be as surprising as it was a decade ago when physician-owned practices were dominant and long tenures the norm.83,84 Turnover has increased with increased system acquisitions and mergers, but systems may better compensate for personnel turnover due to their size and resources.61 These types of disruptions are no longer surprising or unexpected in the primary care practice landscape.
While practices may have acculturated to these prevalent disruptions, the COVID-19 pandemic, occurring after this research was completed, has raised new research questions about practices' abilities and the strategies needed to quickly adapt or pivot when faced with unprecedented and large-scale disruptions. Future research may seek to assess how disruptions happening at different scales or levels (eg, practice, community, region, and beyond), in different domains (eg, personnel, supply delivery), and to different degrees of expectation affect practices' abilities to improve or even maintain their care performance.
This study has a few notable limitations. In the Practice Surveys, we did not capture the number of specific disruption occurrences a practice experienced, only the number of types they experienced. We also did not capture the precise timing of disruptions. Logging disruptions as they occur would enable more sophisticated analyses of how disruptions affect participation in facilitation and for how long.85 We suspect that the timing of disruptions—for example, in the beginning, when facilitators and practices are forming relationships—could affect participation in facilitation. In addition, practices experiencing extreme disruptions may have declined to enroll in EvidenceNOW altogether.
Qualitatively, we performed a secondary analysis of our data. Practices included in our qualitative sample were not selected based on survey reports of disruptions, nor were interview guides designed specifically to explore disruptions. Yet, when asked about intervention implementation and participation challenges, facilitators and/or practice contacts spontaneously described disruptions in 40 of the 158 practices. Our sample may skew toward better-performing practices in EvidenceNOW, but our findings of influential practice characteristics and facilitator support are likely generalizable across practices.
We call attention to a couple of measurement considerations for future research. We chose practice participation in facilitation as our dependent variable because time spent in facilitation indicates an ability to commit to and invest in QI, as time is a precious resource in primary care practices. We operationalized participation as the number of hours of facilitation because this unit of analysis could be standardized across Cooperatives as the “dose” of facilitation that a practice received. We tested several operationalizations of facilitation “dose” (see Appendix Table 4) and found that reports of disruptions were not significantly associated with any of these measures. However, as our qualitative findings show, dose does not capture the complexities of practice engagement,85⇓–87 nor does it reflect entirely the amount and content of the intervention work the practice accomplished.85 Practice motivation to participate in QI likely influences engagement and participation as well, but a standardized measure was not collected across Cooperatives. Investigating various facets of participation in tandem with dose would help achieve a fuller understanding of the mechanisms leading to sustained practice improvement. We also relied on hours of in-person facilitation, positing that in-person visits require a deeper commitment to the intervention than phone or virtual facilitation; however, this assumption may need to be reevaluated in post-COVID-19 research, as practices continue to adopt and adapt to virtual health care innovations.
It is important to note that our analysis relied on a list of specified disruptions. We suggest more precise and expanded specifications for future studies. For instance, “Lost 1 or more office managers or head nurses” was included as one type of disruption, although the loss of these roles may be experienced quite differently by practices, and each loss should be counted separately to determine disruptive load. Write-in responses and qualitative data suggest that other potential disruptions that should be considered for inclusion in survey response categories include loss of MAs,65,88 system-level leadership turnover,89 practice expansions, and consolidations.83,84 A separate and important consideration is turnover in the facilitator role.
Despite these limitations, it is encouraging that practices continued working with facilitators during disruptions, as facilitation is a potential mechanism of practice change.90 External facilitators may be particularly poised to navigate the challenges and varying conditions that shape practice QI efforts, guiding practices toward holistic practice change,63,91,92 as they are not part of these conditions. Specific training in harnessing disruptions to help practices make necessary but difficult changes may help facilitators build greater practice capacity and get closer to achieving performance improvement goals. However, important questions remain about what facilitator approaches and types of participation in facilitation result in measurable performance improvement. Our study takes one step in that direction by showing that disruptions need not disrupt practice QI time, particularly when practices are supported by skilled facilitators who can help them design their QI efforts to fit their current conditions.
Conclusion
Disruptions are prevalent within primary care practices in the U.S. Practices can continue facilitation-based QI interventions during disruptions. Disruptions may motivate practices to work with a facilitator, and external facilitators can support practices that may otherwise experience deleterious effects of disruptions. Specific training that addresses how to modify intervention work based on the capacity and knowledge gaps that disruptions can produce will aid facilitators in helping practices make sustained improvements. Future studies should continue to investigate the impacts of different disruptions on different types of interventions and how facilitation can help strengthen practice QI capacity within these conditions.
Acknowledgments
We are grateful for the advice from Leah Gordon, David Ezekiel, Tom Kottke, Miguel Marino, Rachel Springer, and the EvidenceNOW Cooperatives.
Appendix
Descriptions of “Other” Responses to Post-Intervention Practice Survey Question About Disruptions
Variation in facilitation hours by practice
Methods for Appendix Tables 2-4
We reported rates (exponentiated log-coefficients) and 95% asymptotic confidence intervals (CI). Postestimation of the model yielded estimated marginal means in hours, stratified by 1 or more disruptions versus no disruptions and difference in hours. 95% CIs were reported for all 3 outcomes (see Appendix Figure 1). Equal weight was assumed to calculate the estimated marginal means. To account for missing data, we implemented multiple imputation by chained equations, which determined the stability of model estimates (See Appendix Table 2).
Estimated Marginal Hours and Difference in Hours (95% CI) of Participation in Practice Facilitation by Occurrence of Disruption*
Association of Disruptions During Intervention with Participation in Practice Facilitation: Complete Model, with Imputed and Non-Imputed Results.*
Alternative Definitions of Participation in Practice Facilitation: Summary and Association with Any Disruption
Notes
This article was externally peer reviewed.
Funding: This work is supported by Agency for Healthcare Research and Quality grant #R01HS023940.
Conflict of Interests: The authors report no conflicts of interest in producing and submitting this manuscript for publication. Parts of this early manuscript were presented at the North American Primary Care Research Group, 48th Annual Meeting, November 20, 2020.
To see this article online, please go to: http://jabfm.org/content/35/1/124.full.
- Received for publication May 17, 2021.
- Revision received August 16, 2021.
- Revision received September 16, 2021.
- Accepted for publication September 27, 2021.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵




{kind=link}
{kind=link}