
Abstract
Introduction: Biopsychosocial approaches to health care are critical to addressing childhood obesity. This study aimed to examine how multiple indicators of the home environment related to child weight-related outcomes. We hypothesized that families with home environments of higher chaos and stress, and lower quality parent-child interactions, would have children with a higher body mass index (BMI), less healthy dietary intake, and less healthy eating behaviors.
Methods: Data were drawn from the cross-sectional Phase I of the Family Matters study. Participants were 150 racially/ethnically diverse families with a child between 5 to 7 (mean, 6.4) years old. We used a latent profile analysis approach. A 4-class solution fit the data well, and we used predicted class posterior probabilities to assign families to classes. We then regressed the results onto the distal outcomes of child BMI, healthy dietary intake, and healthy eating behaviors.
Results: Families were classified as Collaborative-Chill (n = 38), Busy Bees (n = 37), Engaged (n = 61), and Inconsistent-Distant (n = 14). Collaborative-Chill was used as the reference class. Inconsistent-Distant families had children with higher BMI (P < .001) that were more food responsive (P < .001). Busy Bees families had children who were more food responsive (P = .04) and more satiety responsive (P = .02). Engaged families had children who were marginally more food responsive (P = .06).
Conclusion: Household chaos, parent stress, and parent-child interactions are important components of the home environment implicated in children's weight-related outcomes. Health care providers should consider these indicators with child patients who struggle with obesity.
- Behavioral Sciences
- Body Mass Index
- Caregivers
- Child Health
- Counseling
- Cross-Sectional Studies
- Eating Habits
- Family Health
- Parent-Child Relations
- Pediatric Obesity
- Primary Health Care
Introduction
Children's physical health is critically important to their long-term well-being. Biopsychosocial approaches to health care, as opposed to the long-dominant biomedical model, consider the many layers of the patient's social environment.1,2 A biopsychosocial approach is critical in delivering whole-person, preventive care, and understanding the home environment for children can facilitate more personalized and effective treatment for weight-related concerns.
Positive parenting behaviors (eg, warmth, sensitivity to children's emotions, monitoring, and consistency3⇓⇓–6) contribute to several positive child outcomes (eg, child self-regulation) and are important to examine with regard to child weight-related outcomes.7⇓⇓⇓⇓–12 Parenting behaviors evaluated in the literature thus far include overall parenting style (ie, authoritarian, authoritative, permissive, or neglectful13⇓⇓–16), parent feeding practices (for example, pressuring to eat, restricting certain foods or amounts,8,17,18 and family members' behaviors around family meals.19,20 There are other aspects of the home environment. We know less about both their relationship with parent-child interactions and how these variables relate to child weight-related outcomes. Household chaos has been put forth as a possible social determinant of health that currently is not regularly assessed or considered for child well-being in a clinical context.21
Research has demonstrated that household chaos has a negative impact on parents' behaviors and children's health, including weight-related outcomes.22 Household chaos is an independent variable unique from parenting style23 and has been found to be related to a less healthful home food environment.24 It is still unknown whether household chaos may contribute to unhealthy child weight-related outcomes.
A closely related but distinct family environment variable is the level of parent stress. Parental stress has been demonstrated as a key moderating factor in the impact of environmental stressors on children's mental and physical health.25⇓–27 The relationship between household chaos and parents' stress levels may look different in different families. Further, there is a reasonable amount of evidence for the relationship between parental stress and child weight-related outcomes, including BMI,28,29 but in combination with the other variables, has not been considered.
While each of the above components has been demonstrated to be related to child health outcomes separately, they do not operate in isolation in actual households. Therefore, it is critical to examine how the combination of household chaos, parent stress, and parent-child interactions work together to create home environment patterns that may relate to child health outcomes. To successfully develop and implement family-based prevention and intervention programs for childhood obesity, we must know what behaviors to target for change. Household chaos and parent stress are novel potential targets that could improve intervention efficacy.
The current study aims to identify profiles from home environment characteristics and examine associations between these home environment profiles and child weight-related outcomes. Our 2 research questions: (1) What home environment profiles emerge when examining household chaos, parent stress, and parent-child interactions?; and (2) How are these home environment profiles associated with child weight-related outcomes, including body mass index (BMI), healthy eating behaviors, and healthy dietary intake?
Methods
Participants
Data for the present cross-sectional study were drawn from Phase I of the Family Matters study, an incremental mixed-methods longitudinal study examining risk and protective factors for childhood obesity in a racially/ethnically diverse sample of primarily low-income children and families.30 Participants were 150 families from 1 of 6 diverse racial/ethnic backgrounds; see Table 1 for full demographic characteristics of the child and primary caregiver who were the focus of this study. Families lived in or near a large Midwestern urban city. Our analyses used child race, child age, child sex, primary caregiver age, and household income as control variables.
Family Matters Phase I Demographic Characteristics (n = 150)
Procedures
Families were recruited through letters sent from their primary care physicians and visited their homes 2 times (10 days apart) to complete data collection. Home visits were conducted in the family's preferred language (eg, Hmong, English, Somali, Spanish). During home visits, research assistants noted data about the home and immediate surroundings, which can be found in Supplementary Table 1. Eligibility criteria for children to participate in the study were if they were 5 to 7 years old, had a sibling 2 to 12 years old living in the same home, lived with their parent or primary guardian more than 50% of the time, and shared at least 1 meal/day with them, and were from 1 of 6 racial/ethnic or immigrant/refugee categories (African American, Native American, Latinx, Hmong, Somali, and white). If there was more than 1 eligible sibling, the closest-age sibling was chosen. The sample was intentionally stratified by race/ethnicity and by child weight status. The University of Minnesota Institutional Review Board approved all protocols for both phases of the Family Matters study, and all participants consented or assented before data collection.
Measures
Household Chaos
Chaos was measured by 4 items from the Confusion, Hubbub, and Order (CHAOS) scale,31 including “We almost always seem to be rushed,” “It is a real zoo in our home,” “No matter what our family plans, it usually does not seem to work out,” and “You cannot hear yourself think in our home.” Items were rated on a scale 1 to 4 (Strongly disagree to Strongly agree). These items were utilized as indicators in the family environment profile. The full CHAOS scale has 15 questions; we used a shorter, 4-question version used in prior studies.24 Preliminary analyses of these 4 questions indicated variability in response patterns to these questions. Because of this, the indicators were kept separate rather than combined as a scale to assess whether specific items had greater or differential impacts.
Parent Stress
One question asked parents, “On a scale of 0 to 10, with 0 being not stressed at all and 10 being very stressed, how would you rate your average level of stress in the PAST 30 DAYS?”.32
Parent-Child Interactions
Families engaged in a video-recorded family board game task at the first home visit. Families were told anyone considered family and anyone who lived in the home was eligible to play the game, and the game was played before any other data collection (except weight to establish eligibility for the study) to decrease potential influences on interactions. The research team member set up a video camera, left the room, and engaged in other study tasks while the family read the instructions and played the game. Families typically spent 20 to 50 minutes to complete the game. The full description of the board game has been published elsewhere.33
The recordings of the task were coded by a team who were blinded to the study hypotheses and who had extensive training on the coding system, the Iowa Family Interaction Rating Scales (IFIRS34). The IFIRS is a global, macro-level observational coding system that measures interpersonal behaviors across multiple family dyads and has shown high validity (r = 0.77-0.86) among racial/ethnic minority samples.34 There were 4 coders on the team, 1 of each were bilingual, speaking 1 of the study languages (Hmong, Somali, Spanish) and English, and the fourth spoke only English. Reliability was attained to 95% at the beginning, and then interrater reliability was assessed at a ratio of 1:5 throughout the coding process. The present study utilized coding from the target child-to-primary caregiver and vice versa, including the constructs of warmth, dominating, and consistent discipline on a scale of 1 to 9 (1 = lowest, 9 = highest).
Child BMI
Children were weighed at the home visit (for full details, see research protocol30). The children's heights and weights were then translated to BMI according to Centers for Disease Control and Prevention (CDC) criteria.
Child Dietary Intake
Using the Nutrition Data System for Research,35 3 separate 24-hour dietary recalls (2 weekdays and 1 weekend day, 2 in-person at-home visits and 1 via telephone) were conducted with the primary caregiver to assess child dietary intake. These records were used to create the Healthy Eating Index-2010 scores.36
Child Eating Behaviors
The Child Eating Behavior Questionnaire37 was used to measure child eating behaviors, including food fussiness (ie, pickiness), food responsiveness (ie, desire/urge to eat when 1 see's smells or tastes palatable foods), and satiety responsiveness (ie, stop eating when full). Example items include “My child is difficult to please with meals” (fussiness), “Even if my child is full up, she or he finds room to eat his/her favourite food” (food responsiveness), and “My child cannot eat a meal if she or he has had a snack just before” (satiety responsiveness). Items are rated on a scale 1 to 5 (Never to Always). Each subscale is summed for a final subscore.
Analytic Plan
Latent profile models38 that are used for identifying latent subpopulations based on personal and environmental random variables39 were fitted to classify families based on the household, parent, and dyadic items operationalized as continuous predictors of family environment class, and an unstructured covariance structure was specified for dominance and warmth dyadic interactions (parent-to-child, child-to-parent) to account for the within-dyad correlation error term. Starting values were selected by seed for 10 random draws in each model. The Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were used to test model fit in 4 latent profile parameterizations in which each subsequent model added one additional predicted class. A 4-class solution had overall best fit based on both AIC and BIC (see Table 3) and predicted class posterior selection probabilities were used to assign families to 1 of 4 classes. Robustness checks were performed to determine if a saturated model that incorporated ecological momentary assessment of family meal atmosphere (eg, proportion of family meals reported chaotic, tense, relaxed, etc.) and food preparation (eg, homemade, preprepared, and fast food) better fit the data compared with the more parsimonious model described above, and the parsimonious model was retained.
Descriptive methods were used to describe how child BMI, eating behaviors, and dietary intake (HEI-2010) differed by class to predict family environment characteristics. Underlying class differences were applied to a regression framework to quantify statistically meaningful anthropometric, eating behavior, and dietary intake outcomes using inferential statistics. Family race/ethnicity, child and parent age and sex, and income were controlled in multiple regression. Robust standard errors were utilized in each adjusted regression model to minimize model misspecification, and predictive marginal estimates from each model were used to characterize effect size and direction of association for the 4 family environment classes. All data management and quantitative analysis were performed in Stata 16.1MP (College Station, TX).
Results
Bivariate correlations are displayed in Table 2. Of note are strong correlations (r = 0.65, P < .001) between child and parent dominating and warm behaviors, meaning when parents behaved warmly, children behaved warmly (or vice versa), and when parents behaved in a dominating manner, children did as well (or vice versa). There were also strong correlations (rs = 0.27-0.45) between the household chaos indicators, although low enough that they were clearly measuring unique aspects of chaos, and between 3 of the chaos indicators (rushed, plans fail, and cannot think) and parent stress (rs = 0.32-0.37). Finally, consistent discipline by parents was significantly correlated with parents and children both behaving more warmly. Parent stress was not significantly correlated with any of the parent-child behavior indicators.
Bivariate Correlations for Home Environment Profile Indicators
Home Environment Profile Model Enumeration
Determination of Home Environment Profiles
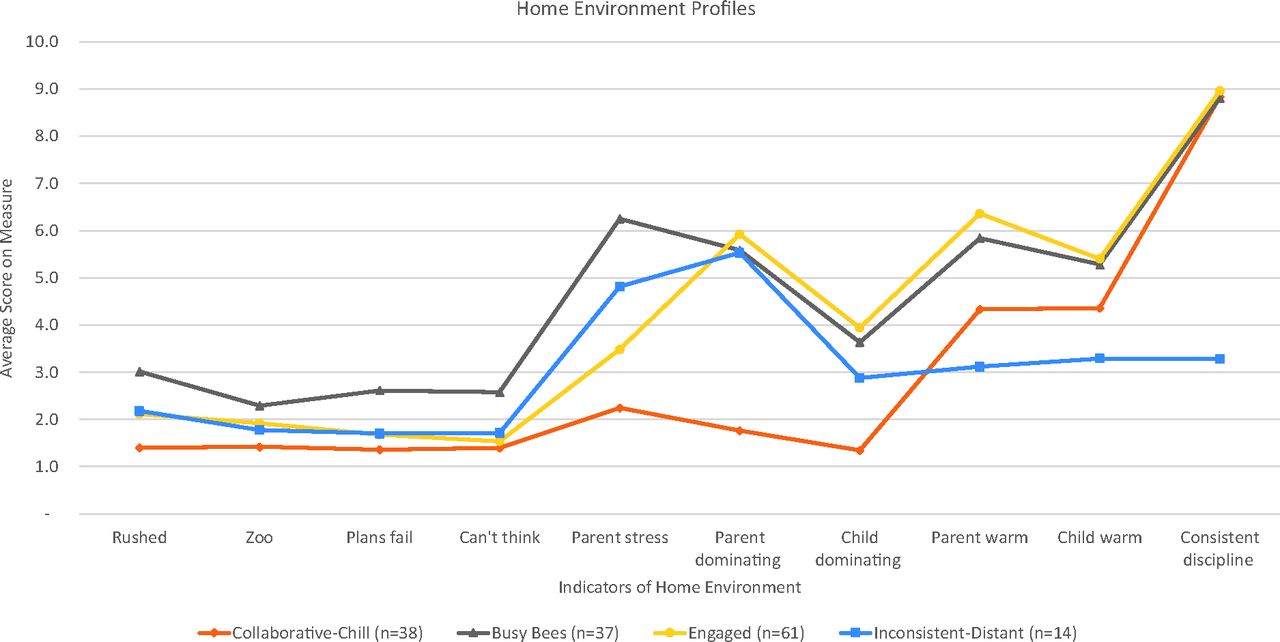
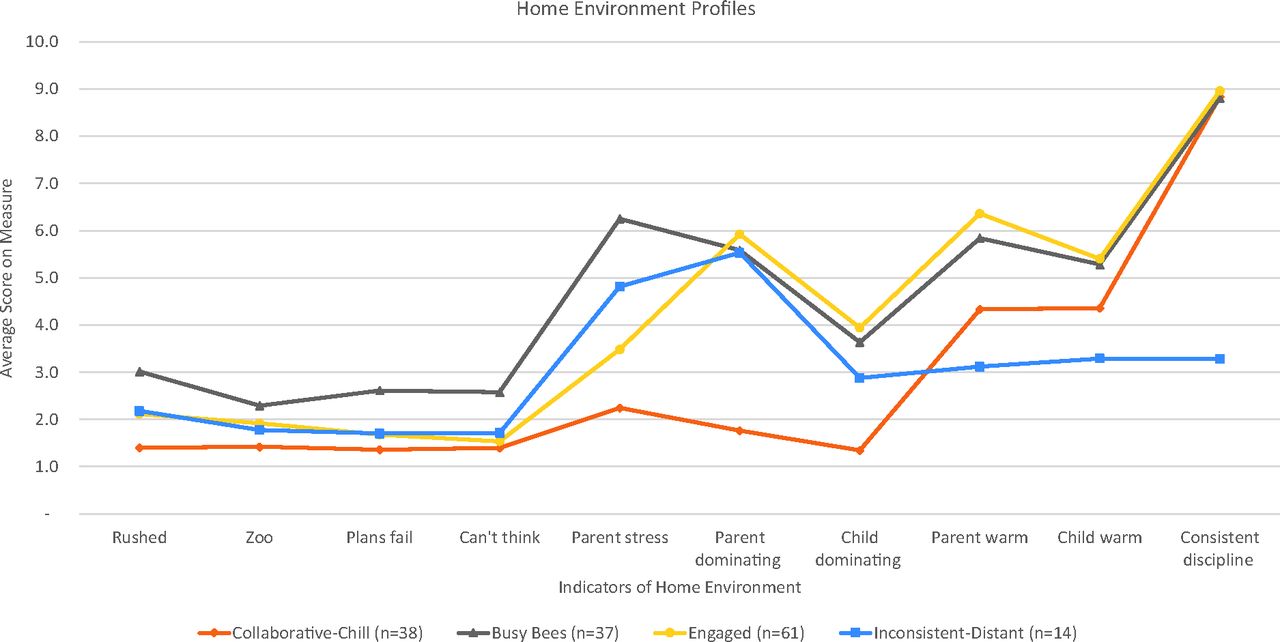
Our first research question was to understand what profiles would emerge when considering home environment characteristics of household chaos, parent stress, and parent-child interactions. The 4 profiles were identified as (1) Collaborative-Chill (n = 38), (2) Busy Bees (n = 37), (3) Engaged (n = 61), and (4) Inconsistent-Distant (n = 14) (Table 4). See Figure 1 to explore the differences between the profiles. Because we included both parent behaviors and child behaviors in the profiles, it is interesting to note that parent dominating behaviors were generally higher than child dominating behaviors across the profiles, parent warmth was generally at the same level or slightly higher than child warmth, with warmth behaviors overall generally higher than dominating behaviors. A notable departure from these patterns is the Inconsistent-Distant parents being much more dominating than their children but not warmer.
Home Environment Profiles Among Family Matters Study Participants
Home environment latent profiles
In summary, the 4 profiles demonstrate systematic variation in family environment around household chaos, parent stress, and parent-child interactions. However, there were no families with either high chaos/low parent stress or low chaos/high parent stress, so our ability to explore the differential impact of these indicators was attenuated. Parents' levels of stress appeared to track with the level of chaos in their households in our sample.
How Home Environment Profiles Relate to Child Weight-Related Outcomes
After establishing the home environment profiles, we examined how those profiles related to child BMI, eating behaviors (fussy eating, food responsiveness, and satiety-responsiveness), and healthy dietary intake (Table 5). Profile 1 (Collaborative-Chill) families were the reference group. Profile 2 (Busy Bees) families included children who were more food responsive (β = 0.46, SE = 0.22, P = .04) and more satiety responsive (B = 0.45, SE = 0.19, P = .02) than Profile 1 (Collaborative-Chill). Profile 3 (Engaged) families were marginally more food responsive (β = 0.40, SE = 0.21, P = .06) than Profile 1 (Collaborative-Chill). Profile 4 (Inconsistent-Distant) families had children with a significantly higher BMI (β = 21.77, SE = 5.8, P < .01) and were more food responsive (β = 0.88, SE = 0.30, P < .01) than Profile 1 (Collaborative-Chill). There was no relationship between the family profiles and either child fussy eating or child healthy dietary intake.
Regression Analyses Between Home Environment Profiles and Child Weight-Related Outcomes
Discussion
Our study considered a broad range of characteristics of the home environment and associations with child weight-related outcomes using latent profile analysis. Individually, household chaos, parent stress, and parent-child interactions characteristics have been linked to risk for childhood obesity, but this study was the first to examine these characteristics in a person-centered statistical analysis structure that allowed patterns or profiles to emerge. Most notably, families with the Inconsistent-Distant profile were found to be strongly associated with childhood obesity. Our results are consistent with a literature review that found several studies have demonstrated significant effects between uninvolved/low control parents and higher BMI.14,40 It is possible that the Inconsistent-Distant (Profile 4) profile may have the most immediate impact on increasing children's BMI compared with other home environment profiles, but that other weight-related outcomes, such as greater food responsiveness and reduced satiety responsiveness, can result in elevated BMI over time.41⇓⇓–44 Home environments such as the Busy Bees (Profile 2), which relate to the latter outcomes, may still be obesogenic due to different mechanisms. Children in Inconsistent-Distant families have higher BMIs, which may be because they have both poorer parent-child dynamics and higher household chaos/parent stress; children in Busy Bees families only have the chaos/parent stress factor but still may eventually develop higher BMIs. There is some previous research that supports this interpretation.20,45,46
Children in families in the Busy Bee, Engaged, and Inconsistent-Distant profiles were more food responsive (ie, ate more in response to external cues rather than due to hunger) than children in Collaborative-Chill families (profile 1). Children and parents were more dominating in parent-child interactions, and parents reported being more rushed and more stressed overall. These 3 home environment profiles differed in their levels of child and parent warmth, levels of discipline consistency, and level of household chaos, which indicates that there may be something specifically about dominating behaviors and parents being rushed/stressed that results in children developing an external locus of control, or that children respond to rushed/stressed, dominating parents by eating (though we did not measure emotional eating specifically). Interestingly, previous research8 has demonstrated that when parents use instrumental feeding practices (using food as a reward/bribe) or emotional feeding practices (feeding in response to child emotion/mood), they may create an environment where the child becomes more food responsive. It is possible that parents in stressed/rushed, dominating home environments use these parent feeding practices47,48 which have been shown to be associated with higher child BMI.49 Conversely, it is worth considering that in Collaborative-Chill families, children may be given the time and space to listen to internal cues for what and when they want to eat, thus responding to true hunger cues rather than external suggestions. Some research50 suggests that parents high in mindfulness had more healthful food-related parenting behaviors.
Finally, children in Busy Bee families had higher levels of satiety responsive than children in Collaborative-Chill families. Typically, satiety responsiveness is considered positive, indicative of better self-regulation.41 Busy Bee families demonstrated the highest household chaos and parent stress, but their parent-child interaction indicators were the highest along with Engaged families, demonstrating moderate-to-high dominating and warmth both ways and highly consistent discipline. It seems likely that the strong parent-child relationships, particularly high in warmth and consistency, may buffer children's abilities to self-regulate even in fairly chaotic or stressed family environments, as some research has indicated.51,52 It is also interesting that Busy Bee children and parents were significantly more dominating than Collaborative-Chill children and parents.
The contrasting results for Busy Bee children that they are both more likely to start eating even when not hungry and more likely to stop eating when they are full was unanticipated. It may be that these families are less structured with their meals and are grazing/snacking a lot, but more research is needed to understand this result.
Implications for future research include examining how the home environment profiles relate to additional child outcomes beyond BMI and eating behaviors, using longitudinal and experimental data to assess possible causality. Researchers and implementers should also consider how interventions designed to address specific aspects of the home environment (eg, parenting behaviors, household chaos) might be combined or otherwise adjusted to incorporate a more comprehensive household intervention. Research can also be completed regarding implementation of standardized assessments in clinical settings (primary care and/or psychiatric) for the potential risk factors of household chaos, parent stress, and parent-child relationships. Health care providers (eg, physicians, nurse practitioners) can provide higher-quality care and may be more effective at helping their patients achieve and maintain healthy weights by using these assessments. While some practices or health care providers may already assess for some of these indicators either informally (through listening to parent-child interactions in visits) or formally (through use of standardized assessments), we suggest that providers who are concerned about a child's weight or eating behaviors might want to introduce household and family relational health assessments, such as the Family Health Scale (long or short form),53 in a systematic way, as these may be contributing factors that are often not identified or addressed. These assessments can inform provider interventions and recommendations and may be indicators for referral to behavioral health for family-level support. Clinics and providers that serve children with weight concerns may find benefit in implementing evidence-based programs such as Family Checkup 4 Health54 in their practices or coordinate with their behavioral health referrals for such programming.
Finally, implications for medical education include that this study is additional support for taking a multi-generational approach to family medicine, considering the family as a whole as well as the individual patient, and considering the impact of the patient's psychosocial and home environment, in this case, the amount of chaos children experience, parental stress, and their relationships with parents, on their physical health. It is also critical that medical training and practice around the topics of household chaos, stress, and parent-child relationships be culturally sensitive and antiracist to engage families in meaningful ways and build the trust that is so important to family physicians working with families over time.
Strengths and Limitations
Our study has some notable strengths as well. It is 1 of few examining the relationship between child weight-related outcomes and family environment variables, especially parent-child behaviors, that used coded parent-child observations rather than self-report parenting scales, providing additional validity to the results.40 In addition, our sample is highly diverse regarding race/ethnicity, which provides more confidence in generalizing the findings.
There are limitations to our study. First, this is a cross-sectional study; thus, directionality cannot be determined. Some research8 indicates there can be a cyclic pattern, especially regarding parent stress and parent-child interactions, and child weight and eating. Another limitation is that the sample is relatively small, and results should be replicated with a larger sample. However, the diversity of the sample and the multimethod approach to data collection aid in external and internal validity. We also used the short 4-question version of the CHAOS scale rather than the full 15-question version. Finally, we did not examine the relationship between the household environment profiles and parent BMI and eating behaviors because it was beyond the scope of this study; comparing these with the child results would be useful for future research in terms of expanding our knowledge of how household environments affect adults in the family as well.
Conclusion
Our results identified co-occurring home environment characteristics, including household chaos, parent stress, and parent-child interactions that clustered into 4 profiles and were significantly associated with child BMI, food responsiveness, and satiety responsiveness. Providers have the opportunity to improve care for children with weight concerns by considering the larger household environment and parent-child relationship in their assessment and plan for treatment.
Acknowledgments
The Family Matters study was a team effort and could not have been accomplished without the dedicated staff members who carried out the home visits, including Awo Ahmed, Nimo Ahmed, Rodolfo Batres, Carlos Chavez, Mia Donley, Michelle Draxten, Carrie Hanson-Bradley, Sulekha Ibrahim, Walter Novillo, Alejandra Ochoa, Luis “Marty” Ortega, Anna Schulte, Hiba Sharif, Mai See Thao, Rebecca Tran, Bai Vue, and Serena Xiong.
Notes
This article was externally peer reviewed.
Funding: This research was supported by the National Heart, Lung, and Blood Institute (Grant No. R01HL126171 to Primary Investigator: Jerica M. Berge). Additionally, GJRB was supported by the National Institutes of Health's National Center for Advancing Translational Sciences grants TL1R002493 and UL1TR002494. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health's National Center for Advancing Translational Sciences.
Conflicts of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/6/1163.full.
- Received for publication April 12, 2021.
- Revision received July 22, 2021.
- Accepted for publication July 26, 2021.




{kind=link}