
Article Figures & Data
Figures
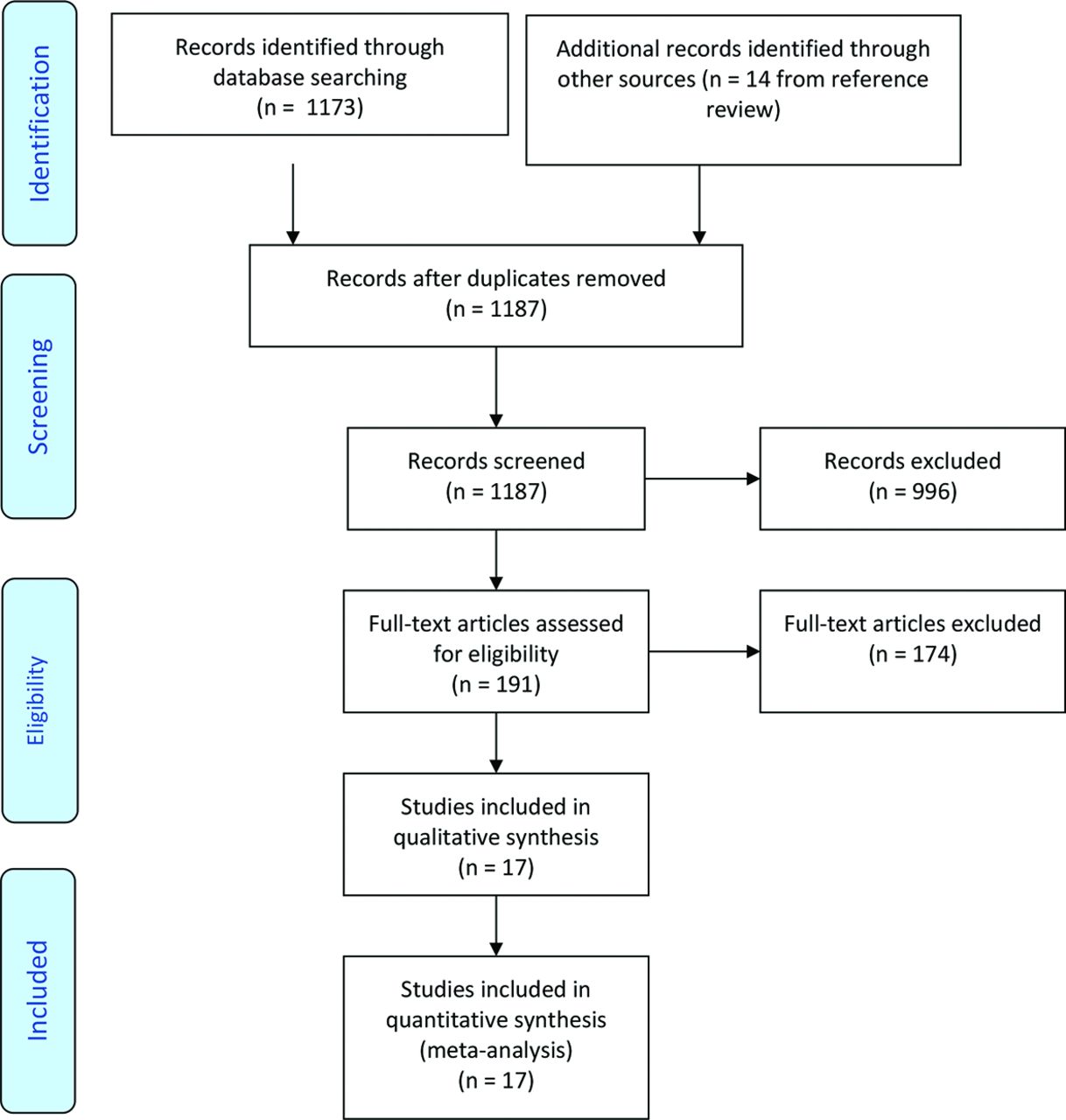
- Figure 1.
PRISMA flow diagram describing the search process.
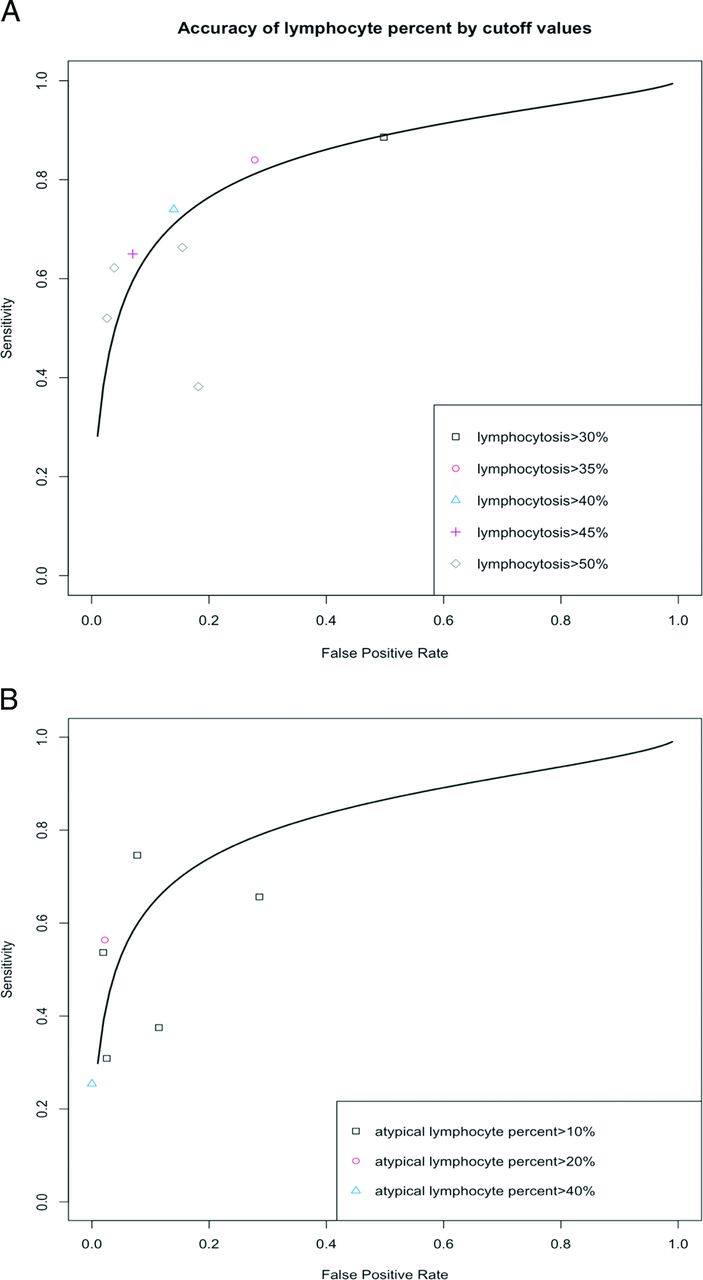
- Figure 2.
Receiver operative characteristic curve by cutoff values for (a) lymphocyte percentage and (b) atypical lymphocyte percentage.
- Figure 3.
Receiver operative characteristic curve stratified by the reference standard tests for (a) lymphocytes greater than 50% and (b) atypical lymphocytes greater than 10%.



Tables
Author, Year Design Number Inclusion Criteria Age Sex / Country Year(s) Patients Recruited Balfour, 200516 Prospective cohort 25 College students aged ≥18 years who had a clinical diagnosis of IM and presented within 10 days after the onset of symptoms were included. Students were excluded if they had acute infection consistent with IM or if they were immunocompromised. Mean, 21 years 72% female EBV profile was tested by EIA (80%) United States 2002 to 2004 Biggs, 20139 Retrospective cohort 726 Retrospective patients presenting with sore throat, fever, and lymphadenopathy and undergoing Monospot test at university health service were included in the study. Patients without full blood count results were excluded from the study. Positive group: Mean, 21 years; Negative group: Mean, 30 years NA Monospot test (Heterophile antibody test) (6.9%) United Kingdom 2011 to 2012 Grotto, 20036 Prospective cohort 590 Young adults who were clinically suspected with IM and reported diagnosis of clinical IM for physical and lab examinations at military lab were included. Patients with intermediate EBV or CMV IgM were excluded from the study. NA 40% female Mono-Latex (heterophile antibody test) and detection of IgM by ELISA kit (64.4%) Israel 1988 to 1991 Hossain, 198922 Prospective cohort 38 Patients aged 5 to 32 years presenting with symptoms suggestive of IM were studied. The minimal criteria included temperature greater than 37°C, greater than 50% lymphocytes and monocytes, and at least 10% atypical lymphocytes. NA NA IM Quick test to detect heterophile antibodies and EBV profile was tested by indirect/IFA (76.3%) Saudi Arabia NA Llor, 201223 Prospective cohort 144 Consecutive adults aged over 14 years with sore throat and 4 Centor criteria—tonsillar exudate, fever, lymph glands tenderness, and absence of cough—and negative pharyngeal testing for group Aβ were recruited. Mean, 24 years 53% female OSOM MonoTest (Genzyme) as immunochromatographic technology to detect EBV profile, then PBD test (10.9%) Spain 2006 to 2009 Lennon, 201027 Retrospective cohort 1000 1000 patients with tonsillitis both in an outpatient and inpatient setting were analyzed to compare the L/WBC ratio in 500 positive and 500 negative Monospot test results. NA 68% female Monospot test (Heterophile antibody test) (50%) Ireland NA Sumaya, 198517 Case series 113 Pediatric patients aged 16 years and younger who had clinical manifestations consistent with IM (fever, tonsillopharyngitis, cervical adenopathy, hepatomegaly, splenomegaly) were included in the study. Patients with WBC≥50% or ≥5000 lymphocytes and at least 10% atypical lymphocytes were also included. Median, 4 years NA EBV profiles were tested by indirect/IFA, and rapid slide tests to detect heterophile antibodies (100%) United States 1976 to 1982 Ventura, 200418 Retrospective cohort 147 Consecutive patients with clinical features that were suspected with IM and had heterophile antibody tests ordered were included in the study. Mean, 20 years 58% female Mono-Latex slide (heterophile antibody test) (46.3%) United States NA Rea, 20013 Case series 150 Patients aged 16 years or older with EBV infection had a positive heterophile antibody test and reported the onset of symptoms within 2 weeks of the test ordered were included in the study. Those suffering chronic, disabling medical condition or having been treated with steroids were excluded. Mean, 22 years 48% female All patients had positive heterophile antibody test; IFA was used to detect VCA-IgM and VCA-IgG (100%) United States NA Brigden, 19998 Prospective cohort 181 Sera were obtained from patients with clinical diagnoses of mononucleosis who subsequently tested positive for heterophile antibody using Monosticon test and from 181 patients with clinical suspected IM who tested negative for heterophile antibody test. Mean, 21 years 59% female Monosticon Dri-Dot test (heterophile antibody test) (50%) Canada NA Ginsburg, 197719 Prospective cohort 43 Children aged 1 to 13 years were selected based on the symptoms and signs compatible with IM. All of them had positive Monospot reactions and showed atypical lymphocytes, and their serum was collected during the acute phase at pediatric outpatient clinic. Mean, 7.7 years 37% female EBV profile was tested by indirect/IFA (69.8%) United States 1974 to 1975 Fleisher, 198320 Prospective cohort 500 Sera from consecutive patients seeking treatment at university health service with illness suggestive of IM were included for EBV-specific serological test. WBC and differential counts were performed uniformly during weekdays and sporadically at other times. NA NA EBV profiles were tested by indirect/IFA (28.3%) United States 1980 to 1981 Krabbe, 198124 Prospective cohort 43 Consecutive hospitalized children aged between 6 months and 7 years were selected if displaying one of the following: nonbacterial pharyngitis or tonsillitis, lymphadenopathy, hepatosplenomegaly, rash or unknown etiology, a blood count with more than 10% atypical lymphocytes, or thrombocytopenia. Below 7 years NA VCA-IgM and IgG were tested by indirect immunofluorescence test (18.6%) Denmark 1981 Chretien, 197721 Case series 150 Patients aged between 17 and 29 years diagnosed with IM from university health service were included in the study. The diagnoses were based on usual clinical criteria for the presence of atypical lymphocytes on peripheral blood smears and positive heterophile antibody tests. NA 36.7% female Monospot test (heterophile antibody test) (100%) United States NA Aronson, 19825 Prospective cohort 709 Consecutive ambulatory adult patients aged between 16 and 73 years presenting sore throat or strep throat from 4 primary care settings were included in the study. The extensive clinical data and heterophile antibody tests were obtained. Mean, 32 years 60% female Monospot test (heterophile antibody test) (2.1%) United States 1976 to 1977 Gartzonika, 201226 Case series 118 Sera from patients aged between 1 and 47 years with a clinical suspicion of IM or acute EBV infection were included in the study. Median, 21 years 51% female EBV profile tested using ELISA test and Cellognost-Mononucleosis test to detect heterophile antibodies (100%) Greece NA Ho-Yen, 198125 Prospective cohort 61 Sera from patients with suspected IM and having positive PBD test results were included in the study. Mean, 17 years 50% female PBD test (61%) United Kingdom NA CMV, cytomegalovirus; EBV, Epstein-Barr virus; EIA, enzyme-linked immunosorbent assay; ELISA, enzyme-linked immunosorbent assay; IFA, indirect immunofluorescence test/anti-complement immunofluorescence assay; IM, infectious mononucleosis; L/WCC, lymphocyte/white blood cell ratio; NA, not applicable; PBD, Paul-Bunnel Davidsohn (heterophile antibody) test; WBC, white blood cell.
Study, Year Patient Selection Index Test Reference Std Flow & Timing Overall Biggs, 2013 L L L L L Grotto, 2003 L L L L L Llor, 2012 L L L L L Lennon, 2010 L L L L L Rea, 2001 L L L L L Brigden, 1999 L L L L L Krabbe, 1981 L L L L L Aronson, 1982 L L L L L Gartzonika, 2012 L L L L L Hossain, 1989 L H L L M Sumaya, 1985 H L L L M Ventura, 2004 L H L L M Ginsburg, 1977 U H L L M Fleisher, 1983 L L L H M Chretien, 1977 L H H L H Ho-Yen, 1981 L H H H H Balfour, 2005 L H H L H ↵* L = 0, M = 1, and H = 2+ with high likelihood of bias.
- Table 3.
Diagnostic Accuracy for Individual Elements of the Clinical Symptom, Sign, and Hematologic Parameter Sort by Positive Likelihood Ratios (LR+) Within Each Category. Where the LR+, Negative Likelihood Ratio (LR-) or Diagnostic Odds Ratio Differed Significantly from 1.0, the Value is Shown in Bold Face
Studies (Patients)-Case Series Studies (Patients)-Cohort Studies Sensitivity (95% CI) Specificity (95% CI) LR+(95% CI) LR-(95% CI) Diagnostic Odds Ratio (95% CI) AUC Symptoms Nausea or vomiting 2 (262)3,21 3 (326)6,16,23 0.30(0.22-0.39) 0.72(0.34-0.93) 1.88(0.54-6.04) 0.99(0.63-1.24) 2.43(0.25-9.30) 0.40 Headache 2 (262)3,21 4 (1036)5,6,16,23 0.59(0.40-0.76) 0.37(0.23-0.54) 1.19(1.01-1.45) 0.72(0.50-0.98) 1.72(1.03-2.77) 0.59 Sore throat 2 (262)3,21 5 (474)6,16,24,25 0.81(0.68-0.90) 0.25(0.17-0.35) 1.121.01-1.25) 0.67(0.41- 1.01) 1.78(1.00-2.98) 0.52 Malaise or fatigue 3 (472)3,21,26 5 (1137)5,6,16,23–25 0.72(0.59-0.82) 0.24(0.11-0.43) 1.02(0.91-1.20) 0.99(0.67-1.48) 1.09(0.62-1.74) 0.57 Loss of appetite 0 2 (883)5,6 0.47-0.74 0.24-0.64 0.86-1.86 0.64-1.54 0.57-2.64 Cough 1 (140)3 1 (709)5 0.22-0.40 0.36(0.32-0.40) 0.63(0.31-1.01) 1.66(0.99-2.28) 0.43(0.14-1.02) Abdominal pain 0 2 (197)6,16 0.33-0.38 0.00-0.56 0.58-1.17 0.90-1.50 0.40-1.31 Myalgia or arthralgia 2 (262)3,21 2 (303)6,24 0.23(0.09-0.49) 0.39-0.59 0.45-1.35 0.47-1.39 0.34-2.76 Signs Lymphadenopathy Posterior cervical 2 (253)3,17 1 (709)5 0.67(0.51-0.80) 0.87(0.84-0.89) 3.16(1.45-5.20) 0.68(0.41-0.93) 5.18(1.55-12.6) Axillary or inguinal 1 (113)17 1 (632)5 0.23(0.09-0.47) 0.82-0.91 3.05(1.85-4.70) 0.67(0.36-0.91) 4.97(2.05-10.5) Anterior cervical 2 (253)3,17 1 (709)5 0.74(0.59-0.85) 0.43(0.39-0.47) 1.27(0.80-1.58) 0.65(0.25-1.28) 2.47(0.63-6.17) Any 4 (445)3,17,21,26 6 (1014)5,6,19,22,24,25 0.93(0.86-0.97) 0.21(0.07-0.49) 1.26(1.05-1.65) 0.37(0.20-0.67) 3.77(1.61-7.55) 0.81 Hepatomegaly 1 (140)3 5 (971)5,6,19,22,24 0.32(0.07-0.75) 0.84(0.18-0.99) 2.42(0.95-6.36) 0.78(0.48-1.10) 3.25(0.84-8.34) 0.63 Splenomegaly 2 (262)3,21 5 (972)5,6,19,22,24 0.45(0.20-0.73) 0.74(0.30-0.95) 2.39(1.11-5.51) 0.66(0.50-0.84) 3.63(1.38-7.77) 0.65 Palatal petechiae 1 (122)21 2 (838)5,23 0.14(0.06-0.28) 0.94-1.00 1.32-11.40 0.57-0.94 1.48-155 Exudate Tonsillar 1 (122)21 2 (747)5,22 0.47(0.30-0.64) 0.78-0.84 1.39-4.13 0.23-0.93 1.49-17.0 Pharyngeal 0 2 (752)5,19 0.13-0.50 0.54-0.93 0.72-4.35 0.62-1.29 0.57-5.39 Fever Measured fever >37.5°C 3 (332)3,21,26 4 (938)5,6,14,17 0.64(0.37-0.84) 0.46(0.17-0.79) 1.20(0.91-1.84) 0.88(0.63-1.33) 1.45(0.67-2.68) 0.56 Subjective fever 0 2 (122)14,23 0.67(0.48-0.82) 0.40(0.24-0.60) 1.14(0.85-1.60) 0.85(0.49-1.32) 1.50(0.64-3.15) Jaundice 0 1 (177)6 0.17(0.10-0.25) 0.79(0.68-0.88) 0.85(0.45-1.51) 1.06(0.91-1.23) 0.83(0.37-1.65) Diarrhea 0 1 (175)6 0.15(0.09-0.23) 0.79(0.67-0.89) 0.79(0.39-1.41) 1.07(0.94-1.26) 0.76(0.31-1.50) Rash 4 (445)3,17,21,26 4 (323)6,16,19,24 0.12(0.06-0.21) 0.75(0.59-0.86) 0.48(0.18-1.12) 1.24(0.98-1.66) 0.41(0.11-1.15) 0.22 Rhinorrhea 0 2 (838)5,24 0.14-0.47 0.37-0.83 0.40-1.53 0.85-2.20 0.25-1.78 Pharyngitis 2 (210)3,26 0 0.94(0.68-0.99) - - - - Hematologic parameters >50% lymphocytes and >10% atypical lymphocytes 0 3 (1361)5,8,20 0.45(0.29-0.62) 0.99(0.92-1.00) 50.4(8.43-162) 0.58(0.38- 0.76) 81.2(19.10-216) 0.82 Atypical lymphocytosis (%) >40% 0 1 (362)8 0.25(0.19-0.32) 1.00(0.98-1.00) 50.3(38.6-64.1) 0.75(0.68-0.82) 355(7.43-622) >20% 0 1 (362)8 0.56(0.49-0.64) 0.98(0.94-0.99) 28.1(9.68-61.4) 0.45(0.38-0.52) 63.9(10.5-148) >10% 0 5 (888)6,8,18,20,24 0.55(0.38-0.70) 0.94(0.91-0.96) 8.97(3.39-19.5) 0.48(0.31-0.65) 19.30(6.48-44.4) 0.83 Lymphocytosis (>4 × 109/L lymphocytes) 0 3 (1235)8,9,18 0.59(0.27-0.84) 0.94(0.93-0.96) 10.2(4.79-16.0) 0.44(0.16-0.75) 30.6(6.53-99.4) 0.64 Lymphocytosis (%) >45% 0 1 (1000)28 0.65(0.61-0.69) 0.93(0.90-0.95) 9.46(6.76-13.1) 0.38(0.34-0.42) 25.2(16.5-36.8) >50% 0 4 (1740)6,8,20,27 0.56(0.46-0.65) 0.93(0.84-0.97) 8.52(2.86-19.9) 0.49(0.36-0.63) 18.7(4.8-51.1) 0.76 >40% 0 1 (1000)27 0.74(0.70-0.78) 0.86(0.83-0.89) 5.31(4.24-6.68) 0.30(0.26-0.35) 17.7(12.8-24.3) >35% 0 1 (1000)27 0.84(0.80-0.87) 0.72(0.68-0.76) 3.02(2.63-3.50) 0.22(0.18-0.27) 13.8(10.1-18.8) >30% 0 1 (1000)27 0.88(0.85-0.91) 0.5(0.46-0.55) 1.78(1.62-1.97) 0.23(0.18-0.30) 7.94(5.63-10.8) Monocytosis (>1 × 109/L monocytes) 0 2 (1088)8,9 0.14-0.72 0.89-0.95 1.46-7.89 0.11-0.98 1.49-55.3 Atypical lymphocytosis (>1 × 109/L atypical lymphocytes) 0 1 (38)22 0.93(0.76-0.98) 0.11(0.01-0.48) 1.11(0.82-1.78) 1.20(0.07-5.69) 4.16(0.15-25.2) Leukocytosis >10 × 109/L 0 4 (1281)6,8,9,19 0.43(0.37-0.49) 0.83(0.76-0.88) 2.55(1.58-3.99) 0.68(0.56-0.82) 3.85(1.93-7.01) 0.63 >5 × 109/L 0 2 (193)6,19 0.93-0.94 0.15-0.21 1.05-1.36 0.15-0.70 1.51-8.73 Neutrophilia (>7.5 × 109/L neutrophils) 0 1 (726)9 0.02(0.00-0.13) 0.88(0.85-0.90) 0.25(0.02-1.03) 1.11(0.99-1.16) 0.23(0.02-1.04) AUC, receiver operating characteristics curve; CI, confidence interval.




{kind=link}
{kind=link}
{kind=link}