
Article Figures & Data
Figures
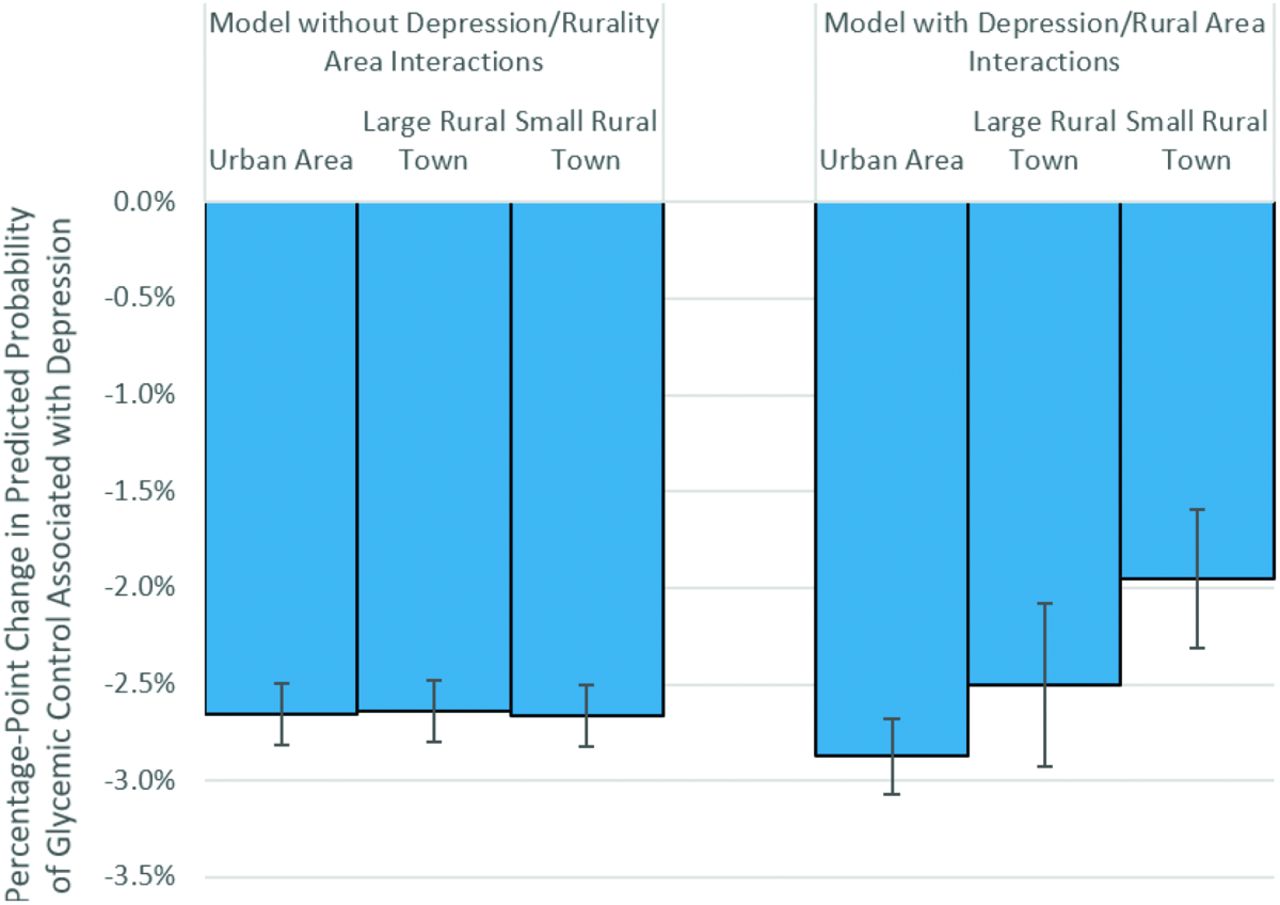
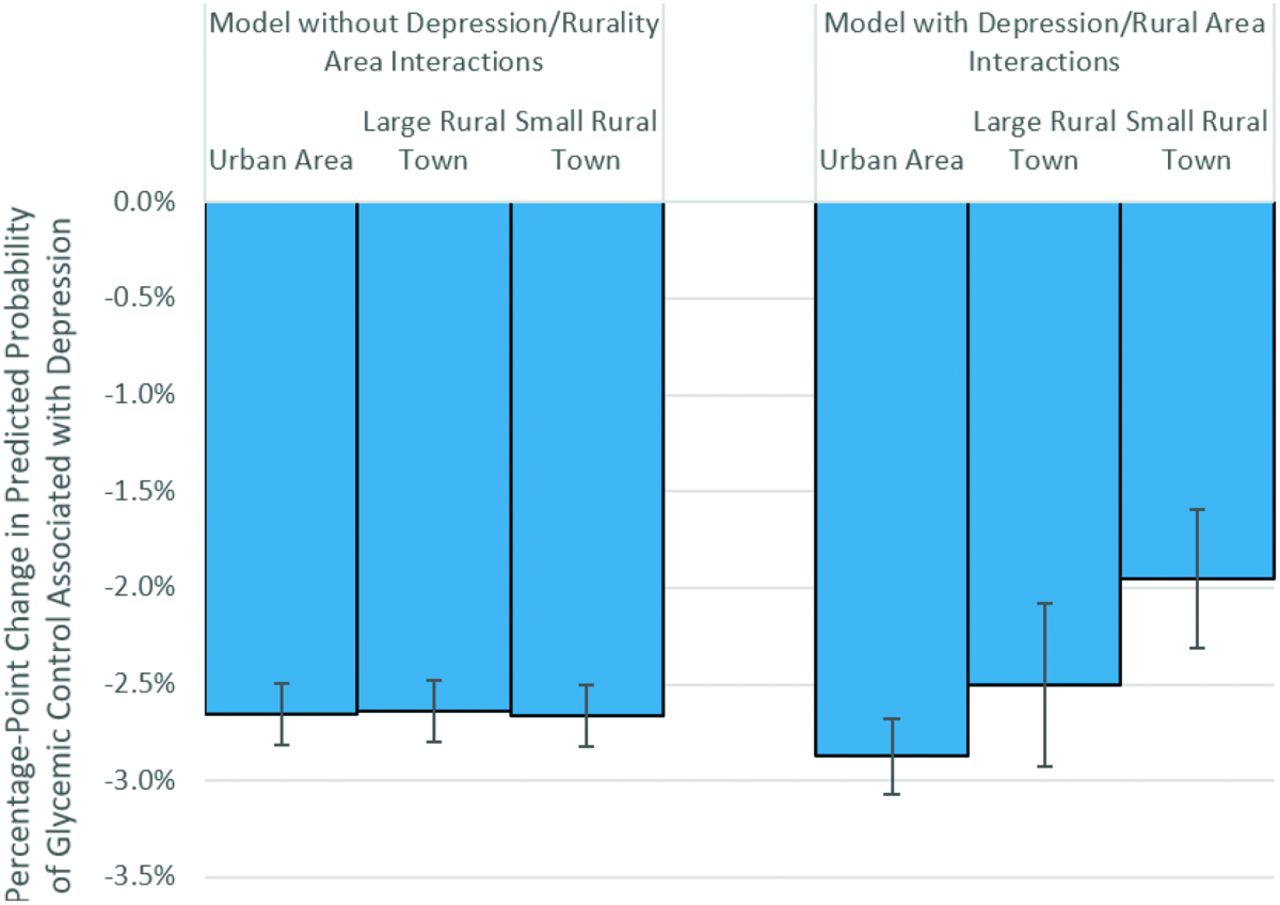
- Figure 1.
Predicted change in the probability of achieving HbA1c < 8% associated with change in depression status by residential location. Note: Predicted changes in probabilities are based on the multivariate logit models. The models are used to compute the average expected change in the probability that HbA1c < 8% when patient depression status changes from “no depression” to “depression,” assuming the residential location is fixed at the level described and all other patient characteristics are held at their true value. The negative changes in probability indicate that glycemic control worsens when a patient is depressed, though the level of this decline may vary by patient location. Error bars indicate the 95% CIs for the estimated changes in probability.
Tables
All Residential Locations Urban Areas† Large Rural Towns† Small Rural Towns† Patient-year observations, n (%) 1,697,173 (100.0) 1,158,921 (68.3) 219,677 (12.9) 318,575 (18.8) Outcome variables HbA1c value, mean (SD) 7.3 (1.5) 7.3 (1.5) 7.3 (1.5) 7.3 (1.5) HbA1c < 8%, n (%) 1,291,705 (76.1) 843,928 (77.4) 167,064 (76.1) 242,604 (76.2) Patient-Level Characteristics Depression, n (%) 384,699 (22.7) 263,583 (22.7) 5,1102 (23.3) 7,0014 (22.0) Patient age (years), n (%) 18 to 44 178,982 (10.6) 129,278 (11.2) 2,1731 (9.9) 2,7973 (8.8) 45 to 54 286,900 (16.9) 206,796 (17.8) 3,3661 (15.3) 4,6443 (14.6) 55 to 64 504,623 (29.7) 347,508 (30.0) 6,4905 (29.6) 9,2210 (28.9) 65 to 75 726,668 (42.8) 475,339 (41.0) 9,9380 (45.2) 151,949 (47.7) Female, n (%) 783,237 (46.2) 535,938 (46.2) 101,793 (46.3) 145,506 (45.7) Ischemic vascular disease, n (%) 291,998 (17.2) 188,746 (16.3) 4,1128 (18.7) 6,2124 (19.5) Type 1 diabetes, n (%) 100,045 (5.9) 6,8620 (5.9) 1,3199 (6.0) 1,8226 (5.7) Insurance, n (%) Commercial 708,927 (41.8) 510,258 (44.0) 8,2380 (37.5) 116,289 (36.5) Medicare 623,037 (36.7) 393,273 (33.9) 9,1842 (41.8) 137,922 (43.3) Medicaid 143,842 (8.5) 108,279 (9.3) 1,5744 (7.2) 1,9819 (6.2) Dual Medicare/Medicaid 8,0520 (4.7) 5,2833 (4.6) 1,0471 (4.8) 1,7216 (5.4) No insurance 5,4803 (3.2) 3,9285 (3.4) 5,382 (2.5) 1,0136 (3.2) Unknown 8,6044 (5.1) 5,4993 (4.8) 1,3858 (6.3) 1,7193 (5.4) Practice-Level Characteristics Certified as a Patient-Centered Medical Home, n (%) 462,728 (27.3) 329,007 (28.4) 5,4507 (24.8) 7,9214 (24.9) Ownership*, n (%) Single-site medical group 5,6155 (3.3) 3,6575 (3.2) 4,328 (2.0) 1,5252 (4.8) Small medical group 329,268 (19.4) 167,391 (14.4) 6,8705 (31.3) 9,3172 (29.3) Large medical group 1,311,750 (77.3) 954,955 (82.4) 146,644 (66.8) 210,151 (66.0) Neighborhood-Level (Patient ZIP Code) American Community Survey Characteristics Percent of population White, non-Hispanic, mean (SD) 82.3 (15.8) 78.5 (16.7) 89.3 (8.6) 91.3 (10.1) Educational distribution of adult population, mean (SD) Percent with no high school degree 8.2 (4.7) 7.5 (4.9) 8.9 (4.2) 10.1 (3.5) Percent with high school degree or GED but no 4-year college degree 60.9 (11.6) 56.9 (11.3) 66.6 (6.7) 71.3 (5.2) Percent with 4-year college degree 31.0 (13.4) 35.6 (13.1) 24.5 (7.6) 18.6 (5.7) Percent of households under the federal poverty level, mean (SD) 11.5 (7.4) 11.0 (8.1) 12.9 (5.9) 12.0 (5.2) - Table 2.
Logit Regression Coefficients for Glycemic Control (HbA1c < 8%) by Depression and Patient Location, Adjusted for Covariates at Patient, Practice, and Neighborhood Levels
Without Depression-Rural Interactions in Model With Depression-Rural Interactions in Model Coefficient P Value Coefficient P Value Depression* −0.150 <.001 −0.162 <.001 Residential location† (ref. group Urban) Large rural town 0.018 .031 0.012 .289 Small rural town −0.002 .734 −0.015 .139 Interactions terms (ref. group Depression* Urban area) (Depression)* (Large rural town) 0.019 .135 (Depression)* (Small rural town) 0.051 <.001 Patient-level control variables Annual trend −0.036 <.001 −0.036 <.001 Patient age, years (ref. group aged 65 to 75) 18 to 44 −0.840 <.001 −0.840 <.001 45 to 54 −0.609 <.001 −0.609 <.001 55 to 64 −0.273 <.001 −0.273 <.001 Female 0.122 <.001 0.122 <.001 Ischemic vascular disease* −0.210 <.001 −0.210 <.001 Type 1 diabetes −0.844 <.001 −0.844 <.001 Insurance (ref. group Commercial) Medicare 0.195 <.001 0.195 <.001 Medicaid −0.224 <.001 −0.224 <.001 Dual Medicare/Medicaid −0.181 <.001 −0.181 <.001 No insurance −0.401 <.001 −0.401 <.001 Unknown −0.018 .038 −0.018 .039 Practice-level control variables Certified as a patient-centered medical home 0.049 <.001 0.049 <.001 Practice ownership‡ (ref. group Large medical group) Single-site medical group −0.104 .006 −0.104 .006 Small medical group −0.087 <.001 −0.087 <.001 Neighborhood-level (Patient ZIP Code) ACS control variables§ Percent of population White, non-Hispanic 0.0027 <.001 0.0027 <.001 Percent of adults with high school degree only −0.0039 <.001 −0.0039 <.001 Percent of adults with 4-year college degree 0.0008 .306 0.0008 .319 Percent of households under the federal poverty level −0.0031 <.001 −0.0030 <.001 Intercept 1.680 <.001 1.684 <.001 ACS, American Community Survey.
↵* Depression and ischemic vascular disease were reported by the primary care practice to MN Community Measurement (MNCM). MNCM suggested the use of the Major Depression or Dysthymia (DEP-01) Value Set and Ischemic Vascular Disease Value Set, but stated that “Any documentation of a new or existing diagnosis of depression [IV.D] during the measurement period [for IV.D: or year prior] is accepted.”
↵† Rurality was determined by mapping patient ZIP code to Rural-Urban Commuting Areas, and summarizing to the WWAMI Rural Health Research Center’s Categorization B. (https://depts.washington.edu/uwruca/index.php).
↵‡ Small medical groups were defined as 2 to 11 primary care sites; large medical groups were defined as 12 or more primary care sites.
↵§ Coefficients represent the impact of a one percentage-point increase in the ACS-based statistic (e.g., 50% to 51%). Educational distribution was represented by percentage of adults with a high school degree but no 4-year college degree, and percentage with a 4-year college degree. We omitted the percentage without a high school degree to avoid collinearity in the estimation. A U-shaped impact of educational distribution in the patient’s neighborhood was evident, with neighborhoods more heavily weighted toward the high-school-only category showing poorer glycemic control.
- Table 3.
Annualized Rates of Office Visit Encounters by Depression Status and Residential Location Observed in Health Plan Administrative Data 2008 to 2014
Urban Patients Rural Patients Average Office Visits per Year % Average Office Visits per Year % Patients without depression Primary care 2.49 44.1 2.28 45.3 Specialty care 3.15 55.9 2.75 54.7 Total 5.64 100.0 5.03 100.0 Patients with depression Primary care 3.58 39.0 3.09 42.9 Specialty care 5.60 61.0 4.11 57.1 Total 9.18 100.0 7.20 100.0 Reduction in primary care fraction −5.2 −2.4
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Successful Change Management Strategies for Improving Diabetes Care Delivery Among High-Performing Practices
- Glycemic outcomes among rural patients in the type 1 diabetes T1D Exchange registry, January 2016-March 2018: a cross-sectional cohort study
- Must-Read Family Medicine Research--Glucosamine/Chondroitin Supplements and Mortality, Telomere Length and the Doctor-Patient Relationship, Reducing Opioid Use, and More