
Article Figures & Data
Figures
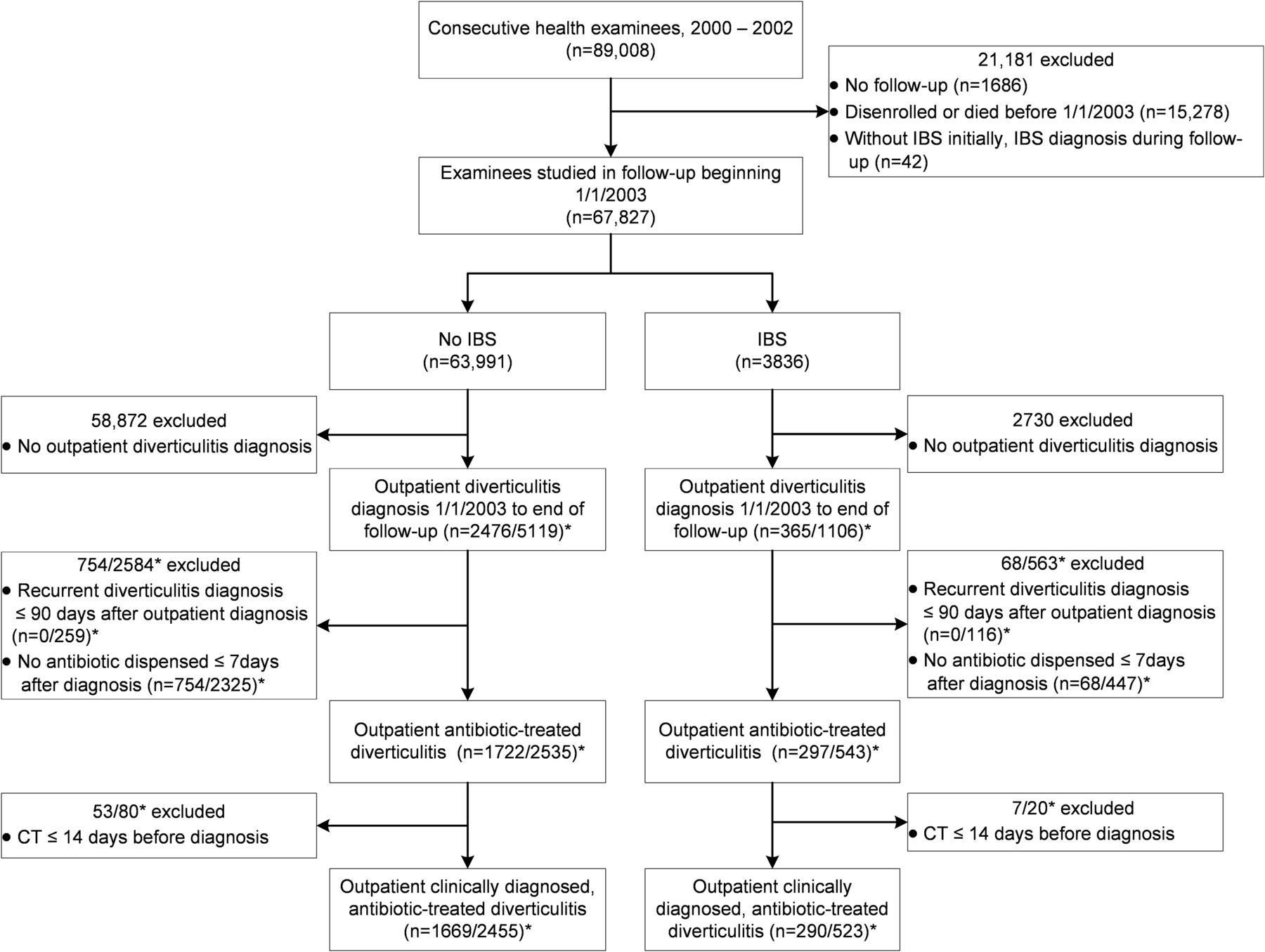
- Figure 1.
Flowchart summarizing derivation of the cohorts with and without irritable bowel syndrome by electronic database criteria. *Number of unique patients/number of episodes. Abbreviations: CT, computed tomography; IBS, irritable bowel syndrome.
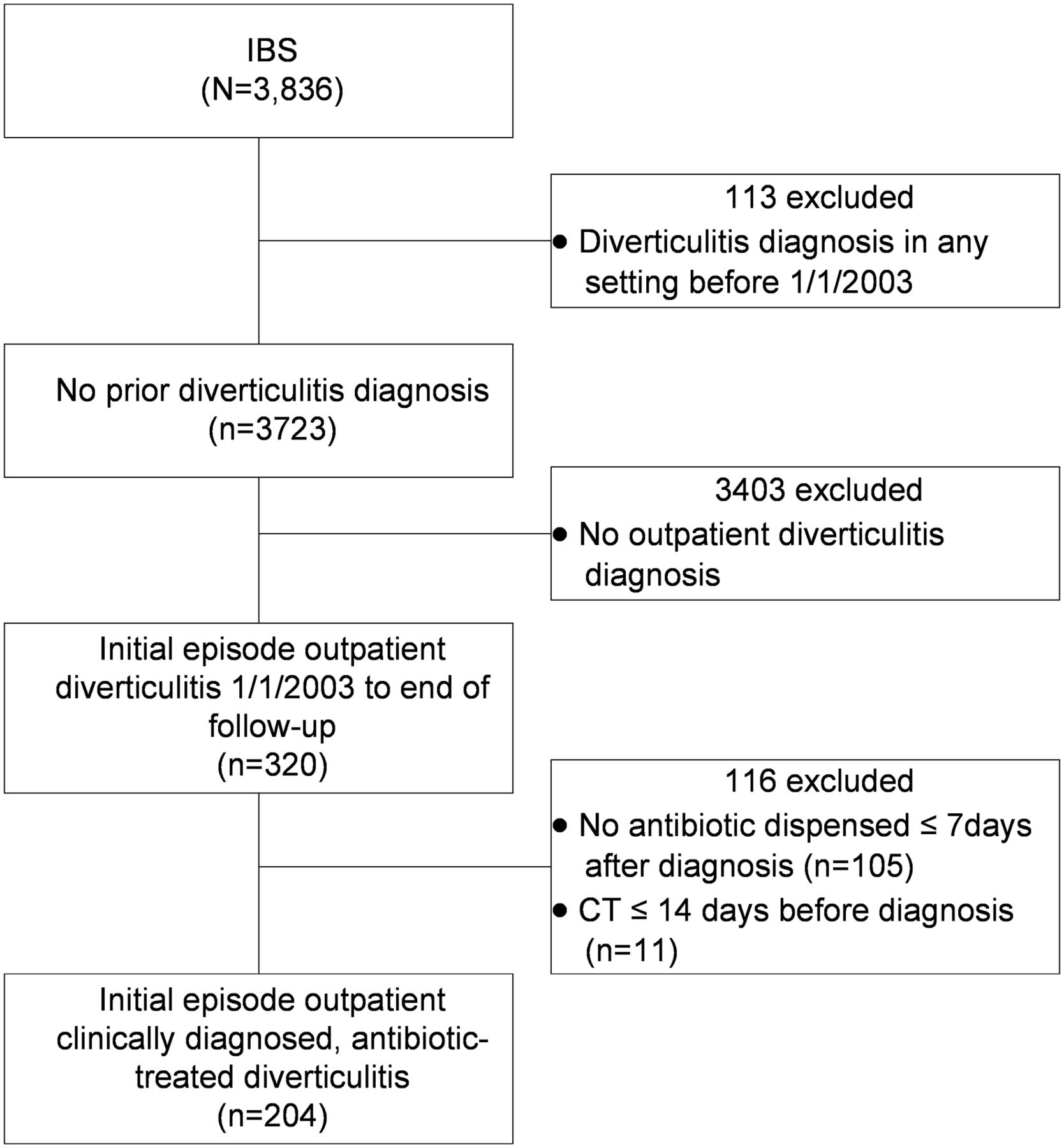
- Figure 2.
Flowchart summarizing derivation by electronic database criteria of the subcohort of irritable bowel syndrome patients who had an initial episode of outpatient clinically diagnosed, antibiotic-treated diverticulitis during followup (2003 to 2017). Abbreviations: CT, computed tomography; IBS, irritable bowel syndrome.
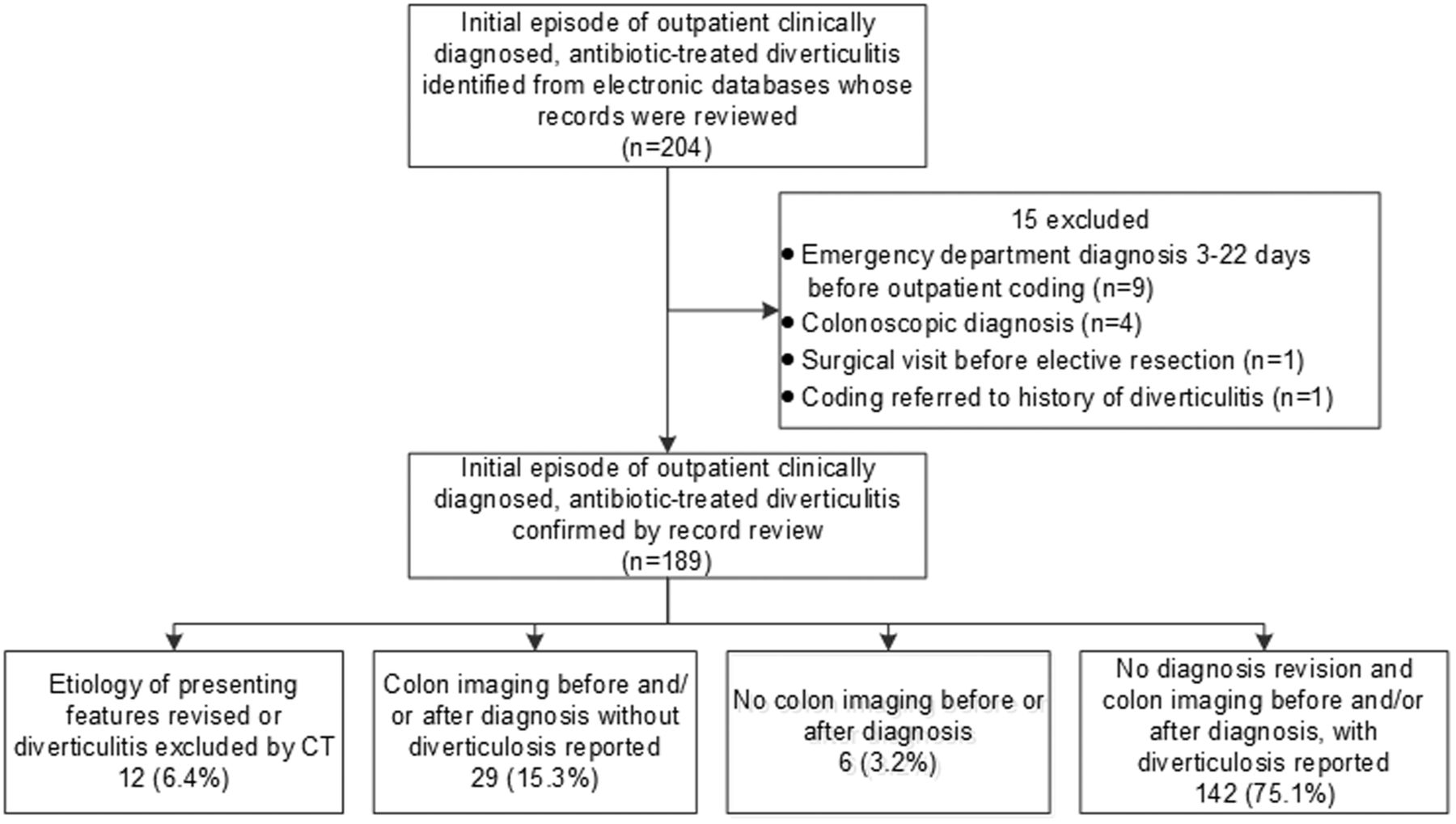
- Figure 3.
Flowchart summarizing further derivation by record review of the subcohort of irritable bowel syndrome (IBS) patients who had an initial episode of outpatient clinically diagnosed, antibiotic-treated diverticulitis during follow-up (2003 to 2017). Patients are classified according to revision or exclusion of the diagnosis, colon imaging and diverticulosis documentation.
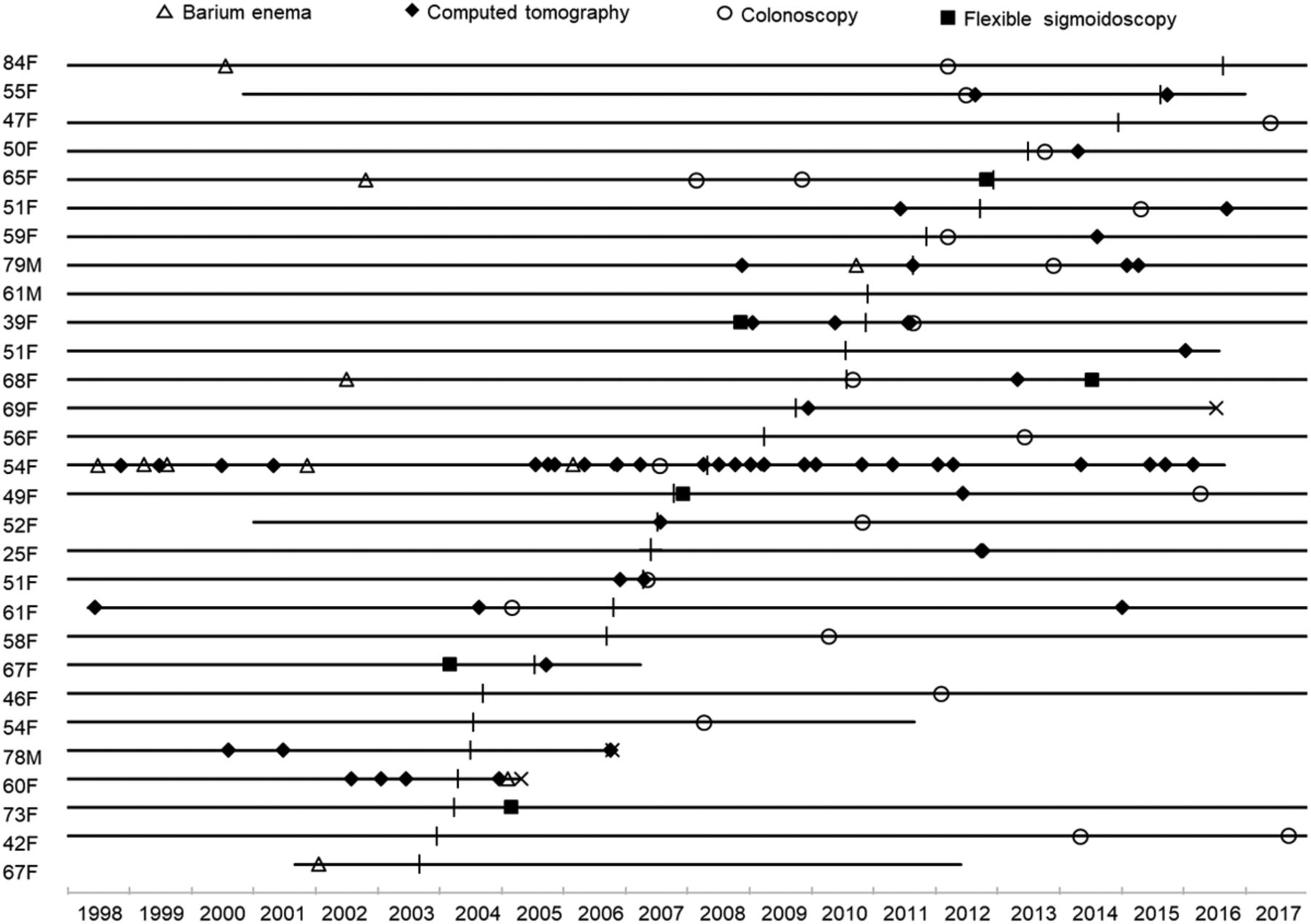
- Appendix.
Colon radiologic and endoscopic imaging procedures that revealed no diverticulosis in 29 outpatients with irritable bowel syndrome whose presenting symptoms were treated with antibiotics as diverticulitis and not revised to another etiology or excluded by computed tomography. Individual patients are indicted by horizontal lines depicting health plan membership. Lines beginning at the onset of 1998 indicate membership starting then or earlier, and a terminal “x” indicates death. Age is at diagnosis of diverticulitis. F, female; M, Male.



Tables
- Table 1.
Baseline Demographic, Medical, and Surgical Features in 67,827 Examinees with and without IBS (2000–2002)
Feature IBS (n = 3836) No IBS (n = 63,991) P Value Demographic Age, mean + SD, y 54.3 + 14.1 51.0 + 15.1 <.001 Sex, n (%) <.001 Male 1139 (29.7) 35,015 (54.7) Female 2697 (70.3) 28,976 (45.3) Race/ethnicity, n (%) <.001 White 3026 (78.9) 41,215 (64.4) Asian 124 (3.2) 5656 (8.8) Black 142 (3.7) 3801 (5.9) Hispanic 399 (10.4) 10,280 (16.1) American Indian 11 (0.3) 177 (0.3) Pacific Islander 22 (0.6) 786 (1.2) Multiple categories 112 (2.9) 2076 (3.2) Education, n (%) <.001 Some high school 201 (5.2) 4518 (7.1) Some college 1993 (52.0) 32,307 (50.5) College and above 1642 (42.8) 27,166 (42.5) Medical history, n (%) Charlson Comorbidity Index <.001 0 3334 (86.9) 57,712 (90.2) 1 to 2 480 (12.5) 5931 (9.3) 3 or more 22 (0.6) 348 (0.5) Anxious 1469 (38.3) 12,856 (20.1) <.001 Worried about being ill 1053 (27.5) 10,363 (16.2) <.001 Depression 1005 (26.2) 7545 (11.8) <.001 Frequent headaches 1149 (30.0) 10,555 (16.5) <.001 Smoking <.001 Never 2173 (56.6) 36,105 (56.4) Past 1361 (35.5) 21,650 (33.8) Current 302 (7.9) 6236 (9.7) Alcohol <.001 Daily 286 (7.5) 5651 (8.8) Never, hardly ever 2321 (60.5) 35,085 (54.8) Less than daily 1229 (32.0) 23,255 (36.3) Vegetarianism 135 (3.5) 995 (3.1) .166 Verbal or physical abuse 791 (20.6) 6659 (10.4) <.001 Sexual abuse 599 (15.6) 4421 (6.9) <.001 Diabetes 185 (4.8) 3088 (4.8) .993 Fibromyalgia 309 (8.1) 698 (1.1) <.001 Hypertension 1244 (32.4) 16,887 (26.4) <.001 Painful intercourse* 411 (15.2) 2681 (9.3) <.001 Chronic pelvic pain* 164 (6.1) 627 (2.2) <.001 Painful urination* 111 (4.1) 610 (2.1) <.001 Frequent urination* 1034 (38.3) 6902 (23.8) <.001 Irregular periods* 383 (14.2) 4259 (14.7) .485 Painful periods* 260 (9.6) 2902 (10.0) .535 Surgical history, n (%) Cholecystectomy 487 (12.7) 2617 (4.1) <.001 Appendectomy 837 (21.8) 7731 (12.1) <.001 Hysterectomy* 920 (34.1) 5206 (18.0) <.001 Back surgery 174 (4.5) 1926 (3.0) <.001 Coronary artery surgery 118 (3.1) 1691 (2.6) .105 Peptic ulcer surgery 19 (0.5) 235 (0.4) .207 IBS, irritable bowel syndrome; SD, standard deviation.
↵* Results from women only.
- Table 2.
Patient Features Associated with Clinically Diagnosed Diverticulitis in 1959 Examinees, 290 with IBS and 1669 Without IBS, During Followup (2003 to 2017)
Feature Adjusted IRR 95% CI P Value Irritable bowel syndrome 2.64 2.21 to 3.15 <.001 Age, y 1.02 1.01 to 1.02 <.001 Race/ethnicity <.001 White Reference Asian/Pacific Islander 0.62 0.49 to 0.79 <.001 Black 0.73 0.54 to 1.00 .047 Hispanic 1.53 1.29 to 1.83 <.001 Other 1.04 0.75 to 1.18 .817 Frequent headaches 1.46 1.25 to 1.70 <.001 Smoking .028 Never Reference Past 1.17 0.96 to 1.48 .106 Current 1.16 1.03 to 1.31 .012 Vegetarianism 0.65 0.45 to 0.93 .020 Diabetes 0.69 0.53 to 0.91 .007 Hypertension 1.35 1.19 to 1.54 <.001 Cholecystectomy 1.47 1.18 to 1.85 .001 Back surgery 1.41 1.09 to 1.81 .009 IRR, incidence rate ratio; IBS, irritable bowel syndrome; CI, confidence interval.
- Table 3.
Twelve Patients with Irritable Bowel Syndrome Whose Diagnosis of Diverticulitis Was Subsequently Revised or Excluded (2003 to 2017)
Case # Age Sex Presenting Features and Therapy of Clinically Diagnosed Diverticulitis Prior Colon Imaging Later Events, Revised Diagnosis, Therapy and Outcome 1
6 FAbdominal pain, diarrhea ×3 weeks, generalized abdominal tenderness. T 36.6°C, Long-term cephalexin usage for cystitis.
Leukocytes 7900/mm3.
Ciprofloxacin/metronidazole.Barium enema 8 years before— diverticulosis Hospitalized 2 days later, diarrhea and weakness.
CT—no diverticulitis,
C. difficile toxin–positive colitis, acute renal failure.
Vancomycin—recovered.
IBS symptoms during 4.3-year followup.2
90 FDiarrhea, mild LLQ pain ×1 week. Took amoxicillin or cephalexin daily in cycles until 10 weeks before, then took vancomycin for unproven C. Difficile infection until 2 weeks before. T 36.8°C, LLQ tenderness.
Leukocytes 11,600/mm3.
Ciprofloxacin/metronidazole.CT 0.4 years before, barium enema 8.3 years before—diverticulosis Hospitalized 2 weeks later, severe bloody diarrhea.
CT—sigmoid/descending colon wall thickening. Flexible sigmoidoscopy—severe pseudomembranous colitis.C. difficile toxin–positive.Vancomycin—recovered.
Recurrent antibiotic-induced C. difficile diarrhea before death from heart failure 4.7 years later.3
77 FLow abdominal pain ×2 days.
T 36.9°C, LLQ tenderness.
Leukocytes 9900/mm3.
Amoxicillin/metronidazole.Barium enema 6 years before— diverticulosis Urinalysis—urinary tract infection. Therapy changed: Ciprofloxacin/metronidazole later the same day—recovered. Diverticulitis diagnosed clinically again 4.1 year later. IBS symptoms during 11-year followup. 4
81 FLow abdominal pain ×1 day.
T 37.4°C, low abdominal tenderness.
Leukocytes 12,700/mm3.
Ciprofloxacin/metronidazoleCT 0.3 year before, colonoscopy 0.4 year before, barium enema 11 years before—diverticulosis Urinalysis—urinary tract infection. Therapy changed: Amoxicillin clavulanate 6 days later—recovered. Diverticulitis diagnosed clinically again 0.2 year later. Died from cancer 2.6 years later. 5
48 MLLQ pain, urgency, bloody stool ×4 days. T 37.1°C, LLQ tenderness.
Leukocytes 8400/mm3.
Ciprofloxacin/metronidazole.None CT 2 days later—sigmoid wall thickening without diverticulosis. Symptoms persisted. Colonoscopy 3.5 months later—colitis. Drug therapy-refractory. Proctocolectomy (Crohn's disease) 2.6 years later. Stable during 10.8-year followup. 6
36 FAbdominal pain, diarrhea ×3 weeks. T 36.3°C, low abdominal tenderness.
Leukocyte count not done.
Ciprofloxacin/metronidazole.None Flexible sigmoidoscopy 6 days later—Crohn's disease. Erythema nodosum, arthritis 8 days later. Drug therapy—did well during 2.4-year followup. 7
89 F“LLQ pain” ×3 days, history of cholecystitis. T 37.5°C, “LLQ tenderness.” On penicillin for dental disease.
Leukocytes 8600/mm3.
Metronidazole added.Colonoscopy 2.1 year before, CT 2.4 years before—diverticulosis. Hospitalized 12 hours later, pain worse. Surgeon noted mid-abdominal pain, epigastric tenderness. Ultrasound—gallstones, gallbladder wall thickened—cholecystitis. Amoxicillin clavulanate—recovered. Occasional low abdominal pain until death from pneumonia 2.5 years later. 8
77 MLeft abdominal pain ×1 day, history of metastatic ileal carcinoid and 2 episodes small bowel obstruction. T 36.8°C, left abdominal tenderness.
Leukocytes 6700/mm3.
Ciprofloxacin/metronidazole.CT 1.2 years before, colonoscopy 7.2 years before—no diverticulosis. Hospitalized 1 day later, pain worse, CT—small bowel obstruction. Resolved. Death from carcinoid 2.3 years later. 9
81 FLow abdominal pain, diarrhea ×10 days. T 36.7°C, low abdominal tenderness.
Leukocyte count not done.
Ciprofloxacin.Barium enema 9.5 years before—no diverticulosis Hospitalized 5 days later, pain worse. CT—sigmoid volvulus. Colonoscopic detorsion—recovered. No visits for abdominal pain until death from cancer 1.7 years later. 10
50 FLLQ pain ×1 day. T 36.4°C, LLQ tenderness.
Leukocytes 9800/mm3.
Ciprofloxacin/metronidazole.Flexible sigmoidoscopy 1.4 years before, colonoscopy 0.8 years before—no diverticulosis. To ED 2 days later, pain persistent. CT—4.6-cm left ovarian cyst. Oophorectomy (cystadenoma) 6 weeks later. No visits for abdominal pain during 4-year followup. 11
67 MMid-abdominal pain, ×1 day.T 37.1°C, “LLQ tenderness.” Leukocytes 15,300/mm3.
Ciprofloxacin/metronidazoleColonoscopy 0.7 years before—diverticulosis Hospitalized 13 days later, pain persisted, worsened. Severe RUQ tenderness. Leukocytes 18,300/mm3. CT—gallstones, gallbladder wall thickened with surrounding edema. Lipase, liver tests increased. Cholecystitis, pancreatitis. Cholecystectomy (chronic cholecystitis with focal gangrene)—recovered. Occasional IBS symptoms during 7.2-year followup. 12
86 FPresenting history, examination, temp data unavailable. Leukocyte count not done. Ciprofloxacin/metronidazole None To ED 3 days later due to vomiting, bloating after starting antibiotics. CT—diverticulosis without diverticulitis. Drug-induced symptoms. Antibiotics stopped. Recovered. Many visits for IBS symptoms, depression, anxiety and 3 more nondiagnostic CTs done for abdominal pain before general decline and death 7.2 years later. CT, computed tomography; ED, emergency department; F, female; M, male; IBS, irritable bowel syndrome; LLQ, left lower quadrant; RUQ, right upper quadrant; T, temperature.
Revised Diagnoses in Bold.




{kind=link}
{kind=link}
{kind=link}
{kind=link}