
Abstract
Introduction: Irritable bowel syndrome (IBS) and diverticulitis share clinical features. Misdiagnosed diverticulitis can cause unnecessary antibiotic therapy. Among IBS and non-IBS patients, we compared outpatient, clinically diagnosed (no computed tomography) diverticulitis rates. Among primary-care, diverticulitis-diagnosed IBS patients, we assessed imaged diverticulosis and probable misdiagnosed diverticulitis.
Methods: Among 3836-patient IBS and 67,827-patient non-IBS cohorts identified from 2000 to 2002, we retrospectively compared the frequency of outpatient, clinically diagnosed, antibiotic-treated diverticulitis from 2003 to endpoints of December 31, 2017, disenrollment, or death. In IBS patients, we reviewed records of initial, primary care-managed episodes for misdiagnosis.
Results: In 3836 clinically diagnosed IBS and 63,991 non-IBS cohorts, followup (median [interquartile range]) was 12.4 (3.9 to 15.0) years versus 10.2 (3.0 to 15.0) years, respectively (P < .001). The incidence rate/1000 patient-years (95% CI) of diagnosed diverticulitis was 14.0 (12.1 to 16.3) and 4.2 (4.0 to 4.5), respectively, (crude incidence rate ratio, 3.3 [2.8–3.9]; P < .001). Of examined features, the diagnosis of IBS was most strongly associated with clinically diagnosed diverticulitis (adjusted incidence rate ratio [95% CI]; 2.64 [2.21–3.15], P < .001). Of initial diverticulitis diagnoses in 189 IBS patients, objective evidence-based diagnosis revision or exclusion occurred in 12 (6.3%), including 6 hospitalized; 29 (15.3%) had colon imaging before and/or afterward without diverticulosis reported; 143 (75.1%) had image-documented diverticulosis; and 6 (3.2%) had no imaging.
Conclusions: Outpatient, clinically diagnosed, antibiotic-treated diverticulitis was increased 3-fold in IBS patients. Primary care clinical misdiagnosis of initial episodes occurred in 1 of 5 patients, but additional misdiagnosis due to misattribution of IBS pain to diverticulitis is suggested.
- Antibiotics
- Diagnostic Errors
- Incidence
- Irritable Bowel Syndrome
- Diverticulitis
- Outpatients
- Primary Health Care
- Retrospective Studies
Introduction
Irritable bowel syndrome (IBS), a common functional disorder, is clinically diagnosed by typical symptoms and exclusion of organic disease, usually by limited testing. It is characterized by recurrent abdominal pain and disordered bowel habits.1 Colonic diverticulosis is also common, but only a minority of patients with it develop acute diverticulitis.2,3 Abdominal pain is the most common gastrointestinal symptom prompting outpatient visits,4 and diverticulitis is often diagnosed in outpatients.5,6 Abdominal pain varies from mild to severe in both IBS7 and diverticulitis, and abdominal tenderness is found with both disorders.1,7⇓–9 Furthermore, many patients with diverticulitis report constipation or diarrhea.8,10,11 These shared clinical features, the frequent absence of fever and leukocytosis,8 and common uncertainty about whether a patient has diverticulosis promote confusion of IBS with diverticulitis.11,12 Outpatients diagnosed with diverticulitis are often treated with antibiotics, so misdiagnosis can result in unnecessary antibiotic therapy.
In a retrospective long-term cohort study, we aimed to 1) compare health examinees with and without IBS regarding the frequency of outpatient clinically diagnosed (no computed tomography), antibiotic-treated diverticulitis and assess associated patient features; and 2) assess imaging reports of diverticulosis, a prerequisite for diverticulitis, and documented misdiagnosis among IBS patients who had an initial primary care diagnosis of diverticulitis.
Methods
Study Setting, Patients, and Data Sources
We enrolled consecutive patients ≥ 18 years of age who had undergone a health screening evaluation during 3 years in the San Diego service area of Kaiser Permanente–Southern California (KPSC), an integrated, prepaid health care system whose members reflect the diversity of Southern California by census.13 All KPSC members have a primary care physician. On October 7, 2007 article records were replaced by electronic medical records. Before that date complete records, including radiologic imaging reports, may not have always been available at outpatient visits; beginning then comprehensive electronic records were uniformly available. Electronic databases included the Charlson Morbidity Index (comprised of potentially life-limiting diseases), comprehensive pharmacy dispensing data and diagnosis coding of all patient encounters using the International Classification of Diseases, Ninth Revision (ICD-9) before October 2015 and the International Classification of Diseases, Tenth Revision (ICD-10) thereafter. Coding staff review codes for all emergency department and inpatient encounters and samples of outpatient encounters.
Identification of IBS and Non-IBS Cohorts
Subjects had previously submitted a self-completed, pre-examination questionnaire eliciting demographic, symptom, and medical/surgical history data, between 2000 and 2002 as part of a separate Institutional Review Board–approved project.14 As previously described, we validated a question on whether a physician had diagnosed IBS by comparing the responses with documented physician diagnosis in the medical records. Agreement occurred in 83.6% of 201 patients (ĸ = 0.82).14 Therefore, examinees were placed in the IBS or non-IBS cohorts according to the question response. We excluded patients initially without IBS who were diagnosed with IBS during followup as identified by ICD-9 code 564.1 and ICD-10 code K58.
Identification of Diverticulitis
We identified diverticulitis from an outpatient ICD-9 code (562.11 or 562.13) or ICD-10 code (K57.20, K57.30, K57.92, or K57.93) and pharmacy dispensing of an antibiotic ≤ 7 days after diagnosis. The outpatient settings comprised nonhospital offices, including after-hours urgent care clinics. Emergency department visits were not included. Most of the practitioners were primary care physicians, but nurse practitioners and physician assistants working under their supervision likely diagnosed some cases. As previously published, we developed this case finding method in a pilot sample by assessing multiple computerized algorithms based on electronic data, including diagnosis codes, dispensing of antibiotics and pain medication and/or pain diagnoses, and excluding patients with infections and/or conditions that could mimic diverticulitis. Testing the method in 1502 randomly selected KPSC members revealed a sensitivity of 84.6% and positive predictive value of 98.1% for physician-diagnosed diverticulitis in outpatients.15 As we assessed only clinically diagnosed diverticulitis, we excluded patients who had undergone computed tomography (CT) of the abdomen and/or pelvis with or without oral contrast ≤ 14 days before diagnosis, identified by Current Procedural Terminology codes 74176 to 74178, 74150, 74160, and 74170. We assessed the frequency of outpatient, clinically diagnosed, antibiotic-treated diverticulitis diagnosis from January 1, 2003 to December 31, 2017.
Evaluation of the IBS Cohort for Misdiagnosis and Diverticulosis Documentation
Two gastroenterologists independently reviewed the medical records of patients in the IBS cohort who had an initial episode of outpatient clinically diagnosed, antibiotic-treated diverticulitis. They recorded data from the outpatient visits when the diagnoses were made, including clinical features and leukocyte counts. Fever was defined as temperature > 37.5°C and leukocytosis as >11,500 leukocytes/mm3. They searched outpatient visit records, hospitalization summaries, and laboratory and pathology reports following the visit for evidence of a revised diagnosis with changed therapy or exclusion of diverticulitis, the latter requiring CT ≤ 3 days after diagnosis that revealed no colonic wall thickening, inflammation of peri-colic fat, or other findings of diverticulitis. They recorded all barium enema, flexible sigmoidoscopy, colonoscopy, and abdominopelvic CT procedures performed before and after the diagnosis and considered the patient as having diverticulosis if a single procedure reported diverticulosis of any severity. Patients with multiple imaging tests were classified as having no diverticulosis only if no procedure reported it, either before or after the diagnosis. The reviewers resolved any discrepancies by joint record review.
Statistical Analysis
We summarized categorical data as percentages and continuous data as mean ± standard deviation (SD) or median (interquartile range) as appropriate. We compared categorical data with the c2 test and continuous data with the Student's t-test. Incidence rates per 1000 patient-years were calculated and corresponding 95% CIs were estimated using robust Poisson regression. Controlling for age, sex, race/ethnicity, and all other medical and surgical history variables from the patient questionnaires (Table 1), multivariable Poisson regression was fitted to derive the adjusted incidence rate ratio of diverticulitis in the IBS cohort versus the non-IBS cohort. All tests were 2 tailed, and the level of significance was < .05. We used SAS statistical software (version 9.4; SAS Institute, Cary NC).
Baseline Demographic, Medical, and Surgical Features in 67,827 Examinees with and without IBS (2000–2002)
Results
Patient Features
Demographic and history features differed between the 3836 subjects in the IBS cohort and the 63,991 subjects in the non-IBS cohort (Table 1), as previously described in the larger cohorts from which they were derived.14 Length of followup was 12.4 (3.9 to 15.0) years versus 10.2 (3.0 to 15.0) years in IBS and non-IBS cohorts, respectively (P < .001).
Diverticulitis Diagnosis Frequency and Associations in IBS and non-IBS Cohorts
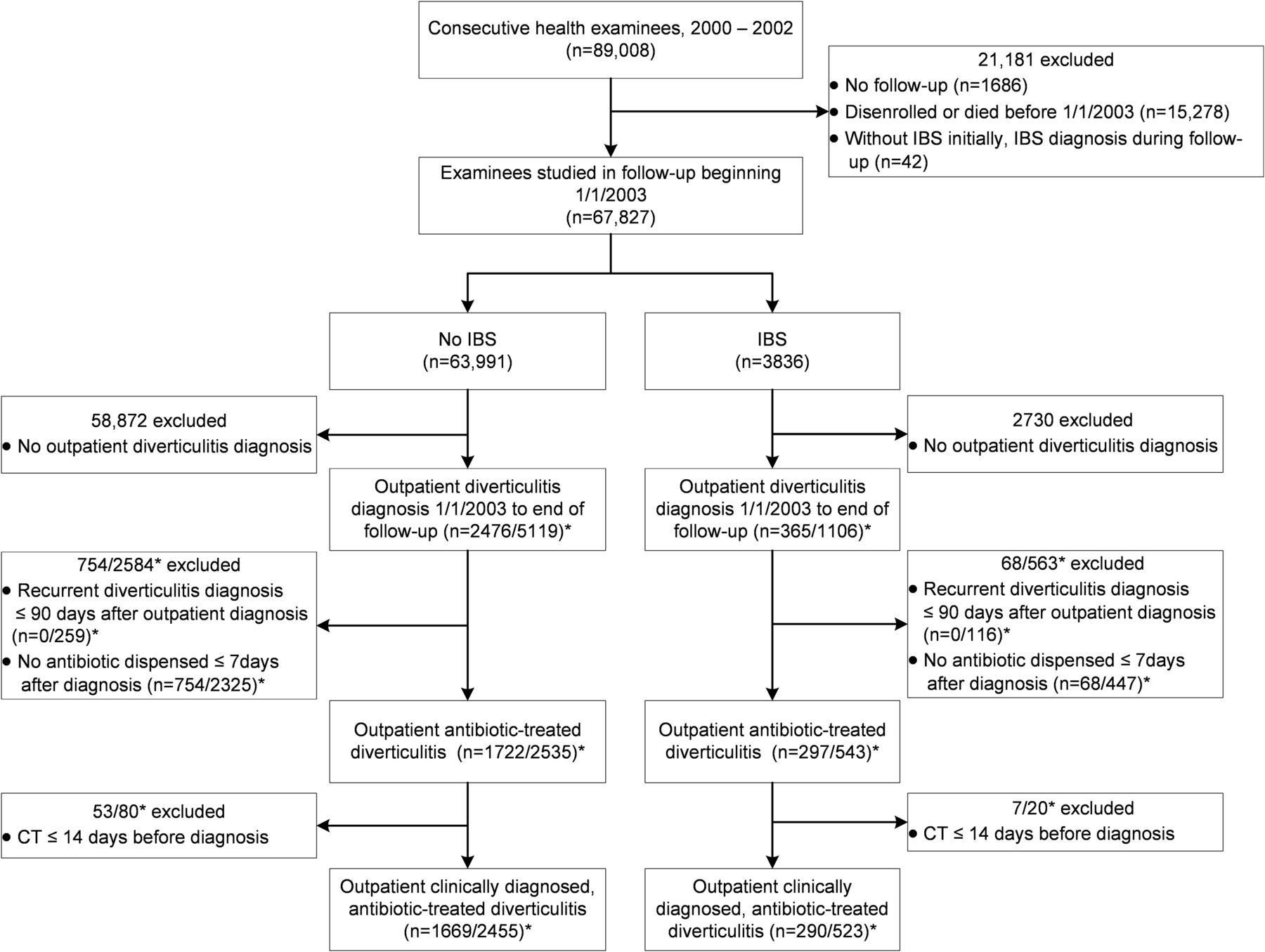
Of 89,008 examinees, we excluded 21,181 as detailed in Figure 1, yielding 67,827 examinees, 3836 (5.7%) IBS and 63,991 (94.3%) non-IBS examinees. Additional exclusions by electronic database criteria yielded 290 IBS individuals with 523 episodes and 1669 non-IBS individuals with 2455 episodes.

Flowchart summarizing derivation of the cohorts with and without irritable bowel syndrome by electronic database criteria. *Number of unique patients/number of episodes. Abbreviations: CT, computed tomography; IBS, irritable bowel syndrome.
At least 1 episode of clinically diagnosed, antibiotic-treated diverticulitis occurred in 290 of 3836 (7.6%) and 1669 of 63,991 (2.6%) outpatients with and without IBS, respectively (P < .001). The incidence rate (95% CI) per 1000 patient-years of outpatient clinical diagnosis and antibiotic treatment was 14.0 (12.1 to 16.3) versus 4.2 (4.0 to 4.5) in IBS and non-IBS cohorts, yielding a crude incidence rate ratio of 3.3 (2.8 to 3.9) (P < .001).
Multivariate Poisson regression revealed that of the patient features, IBS was most strongly associated with outpatient diagnosis (Table 2). Age was only negligibly associated, and a race/ethnicity association varied from negative associations in Asians/Pacific Islanders and blacks to a positive association in Hispanics compared with whites. Frequent headaches, current smoking, hypertension, cholecystectomy, and back surgery were positively associated, and vegetarianism and diabetes were negatively associated. The Charlson Comorbidity Index was not associated with the diagnosis.
Patient Features Associated with Clinically Diagnosed Diverticulitis in 1959 Examinees, 290 with IBS and 1669 Without IBS, During Followup (2003 to 2017)
Initial Outpatient, Clinically Diagnosed, Antibiotic-Treated Diverticulitis in the IBS Cohort
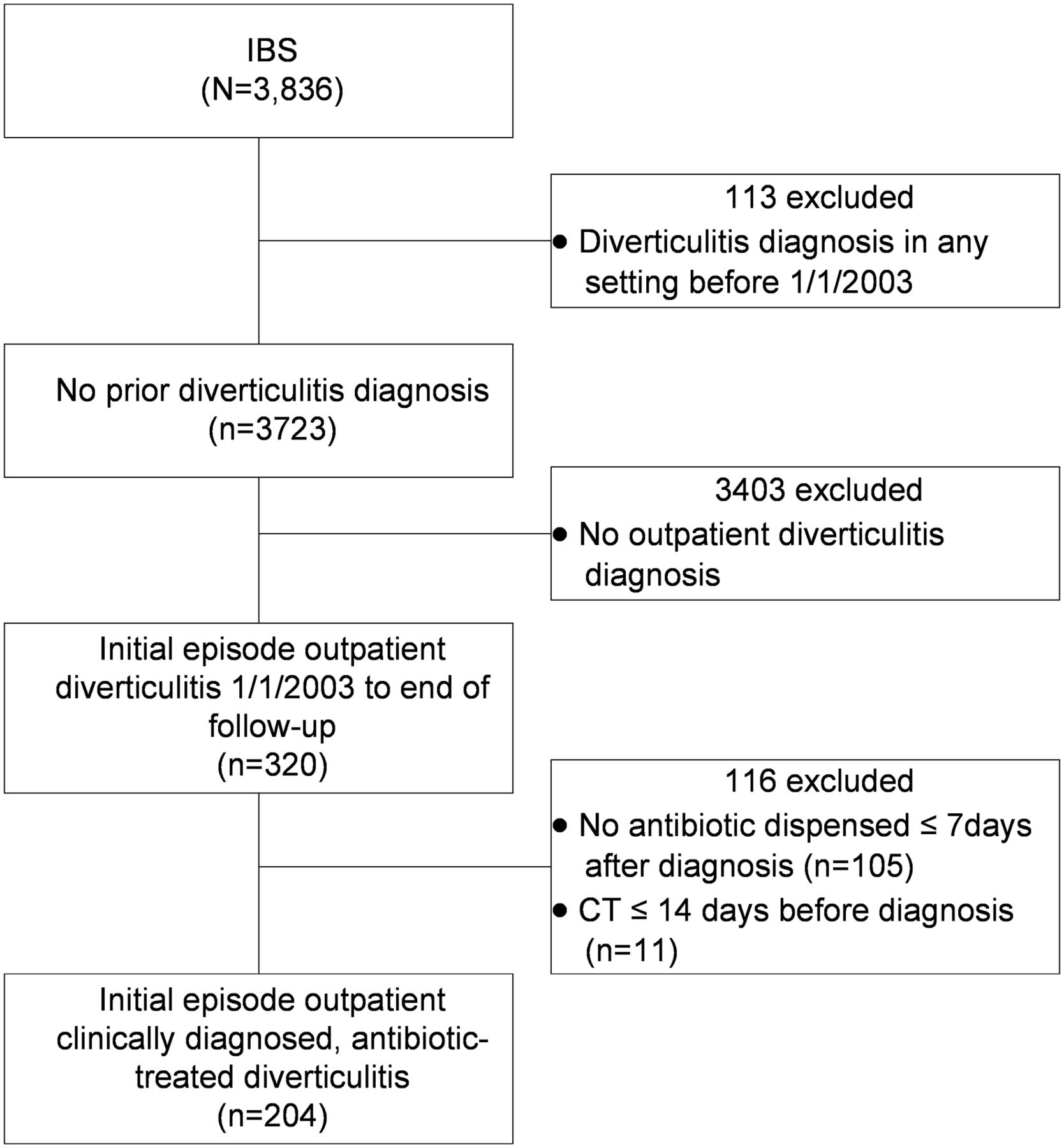
To identify initial episodes of diverticulitis during followup in the IBS cohort, we excluded patients electronically from the total 3836-patient IBS cohort for a diverticulitis history, lack of outpatient diagnosis, use of CT and lack of antibiotic treatment, yielding 204 patients (Figure 2). Record review led to exclusion of 15 additional patients, yielding a final cohort of 189 IBS patients with an initial episode (Figure 3). The age (mean SD) at diagnosis was 65 ± 12.7 years, and 142 (75.1%) were female. Clinical and laboratory records were available on all patients. Temperature was recorded on 118 (62.2%) patients. Abdominal pain, tenderness, and fever occurred in 181 of 189 (95.8%), 176 of 189 (93.2%) and 3 of 118 (2.5%) patients, respectively. Of 76 (40.2%) patients who had a leukocyte count performed, 26 (34.2%) had leukocytosis.

Flowchart summarizing derivation by electronic database criteria of the subcohort of irritable bowel syndrome patients who had an initial episode of outpatient clinically diagnosed, antibiotic-treated diverticulitis during followup (2003 to 2017). Abbreviations: CT, computed tomography; IBS, irritable bowel syndrome.
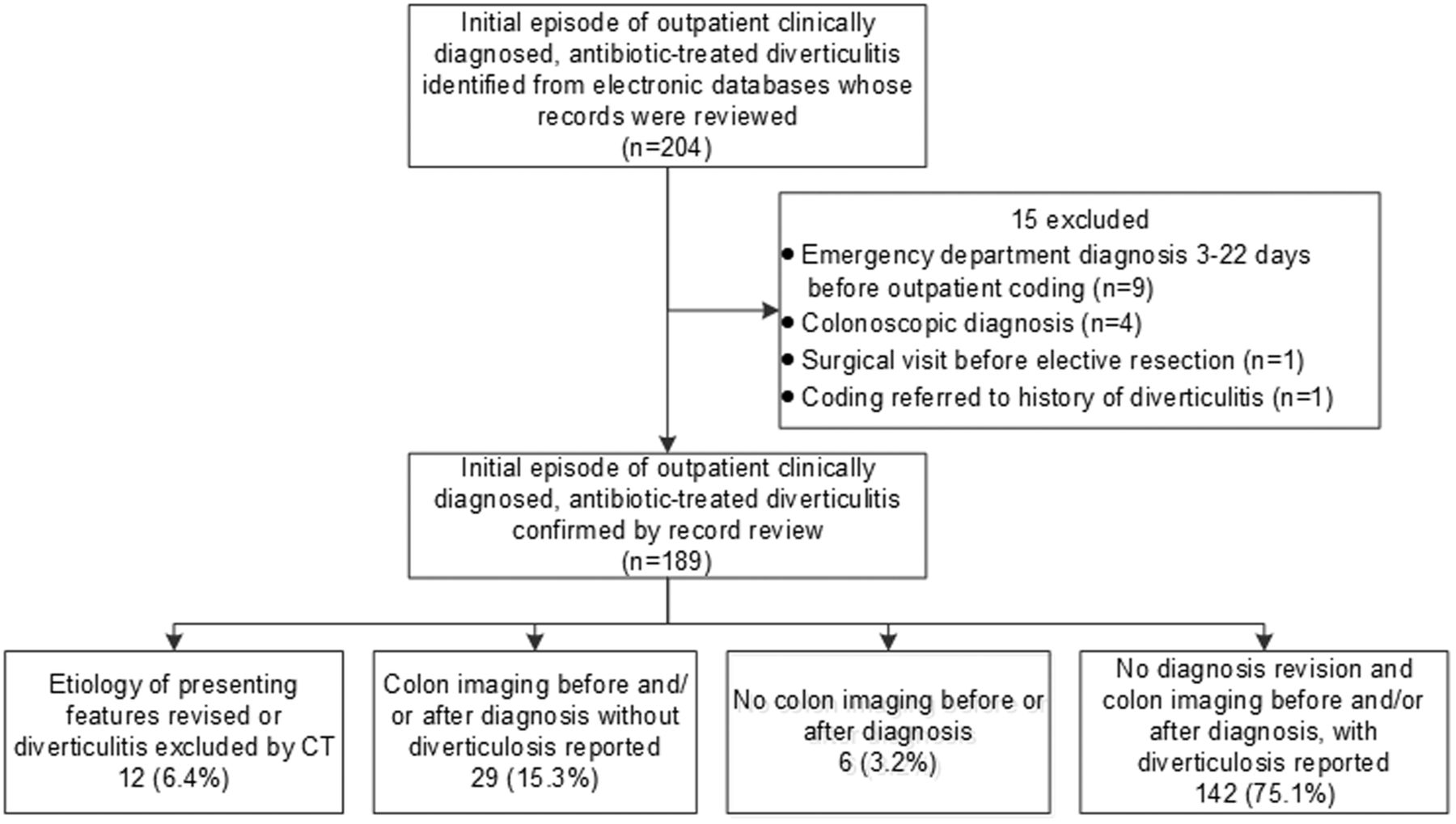
Flowchart summarizing further derivation by record review of the subcohort of irritable bowel syndrome (IBS) patients who had an initial episode of outpatient clinically diagnosed, antibiotic-treated diverticulitis during follow-up (2003 to 2017). Patients are classified according to revision or exclusion of the diagnosis, colon imaging and diverticulosis documentation.
Misdiagnosis and Diverticulosis Documentation in the IBS Cohort
Figure 3 also summarizes patients whose diverticulitis diagnosis was revised or excluded and the results of colon imaging studies. Within 2 weeks after antibiotics were dispensed for diverticulitis, 12 (6.3%) patients were found to have objective evidence of another etiology for their presenting features (11) or lack of diverticulitis on CT (1). As detailed in Table 3, diseases in the 11 patients were Clostridium difficile colitis (2), urinary tract infection (2), Crohn's disease (2), cholecystitis (1), small bowel obstruction (1), sigmoid volvulus (1), and ovarian cyst (1), and cholecystitis and pancreatitis (1). Six of the patients were hospitalized, and all 12 survived. CT was performed in 3 additional patients 1 to 7 days after diagnosis, which confirmed diverticulitis in all.
Twelve Patients with Irritable Bowel Syndrome Whose Diagnosis of Diverticulitis Was Subsequently Revised or Excluded (2003 to 2017)
Twenty-nine (15.3%) patients had no diagnosis revision, but they had colon imaging that did not reveal diverticulosis before and/or after diagnosis. As detailed in Appendix, the age of these patients ranged from 25 to 84 years, 26 (89.7%) were female, and at least 1 procedure revealing no diverticulosis occurred before, after or both before and after diagnosis in 5, 15, and 9 patients, respectively. Nineteen (65.5%) patients had > 1 negative procedure, including 11 who underwent ≥ 3 procedures.
Combined with the revised diagnoses or CT exclusion of diverticulitis in 12 patients, a lack of diverticulosis on imaging supported misdiagnosis in 41 of 189 (21.7%) patients. One hundred forty-two (75.1%) patients (age 66.3 ± 11.4 years; 58 [40.8%] < 65 years; 102 [71.8%] female) had a diagnosis that was not revised nor excluded by CT and had imaging before and/or after the episode that revealed diverticulosis. Six (3.2%) had no colon imaging.
Discussion
In this retrospective, long-term, cohort study of health examinees, patients with an IBS diagnosis had a 3-fold increase in the frequency of outpatient, clinically diagnosed and antibiotic-treated diverticulitis compared with those without IBS. Of the features assessed in association with diverticulitis, the strongest association was found with diagnosis of IBS. In patients with IBS and an initial episode of diverticulitis managed in primary care, diagnosis revision and changed therapy occurred in 6.3% of patients. An additional 15.3% of patients had colon imaging studies before and/or after the diagnosis that reported no diverticulosis. These findings support misdiagnosis in 1 of 5 patients.
Published evidence is lacking to support such a strong association between IBS and diverticulitis, as we found. An association was reported between IBS, especially diarrhea-predominant IBS, and diverticulosis only in patients aged ≥ 65 years, but not with diverticulitis.16 Another survey found an association between IBS and diverticulosis only in patients > 60 years but did not assess diverticulitis.17 We did not determine bowel habit predominance; 40.8% who had diverticulosis diagnosed and lacked evidence of misdiagnosis were < 65 years when initially treated for diverticulitis. Therefore, it seems unlikely that increased diverticulosis alone explained the 3-fold increased rate of physician-diagnosed diverticulitis in the IBS cohort.
Diagnosis of diverticulitis in our IBS cohort was primarily based on abdominal pain and tenderness, as fever and leukocytosis were infrequent. Surgeons have also reported on the scarcity of objective evidence of diverticulitis diagnosed in most clinic patients and suggested that many outpatients have mild disease or no diverticulitis at all.6,18 However, we are unaware of other investigations that compared the frequencies of the outpatient clinical diagnosis of diverticulitis in patients with and without IBS or attempted to document misdiagnosis in IBS patients.
Some of the patients had life-threatening disorders. Other patients lacked diagnosis revision or CT exclusion of diverticulitis and had colon imaging, two thirds with multiple procedures, without a report of diverticulosis.
These 2 types of misdiagnosis may not fully explain the greatly increased diverticulitis frequency in IBS patients. Just as increased abdominal and pelvic surgery in the IBS cohort was attributed to symptom misattribution,14 abdominal pain and tenderness could have been incorrectly attributed to diverticulitis. Such misattribution was proven in only 1 case, but few patients had CT before symptoms resolved to allow this assessment, which is typical in outpatient settings. There is evidence of a deficiency in physician awareness of features of IBS patients, including their health care–seeking behavior. Surveys of American19 and European20 primary care physicians revealed only a minority knew important aspects of IBS or used the Rome diagnostic criteria. About three quarters of American primary care physicians regarded IBS as a diagnosis of exclusion and relied less on symptoms and ordered more tests than specialists.21 To our knowledge, primary care physicians' awareness of abdominal tenderness in IBS has not been systematically studied, although a landmark publication almost 60 years ago7 detailed tenderness in over 60% of patients. Furthermore, patient reactions to abdominal palpation can help distinguish functional from structural disorders.22
Limitations include our inability to identify which IBS patients with diverticulosis and no other etiology evident for their acute symptoms, had diverticulitis versus a flare of IBS or another disorder. We cannot exclude the possibility that IBS was incorrectly diagnosed and that in follow-up diverticulitis was mimicked by another disease or coexisted with it, such as the Crohn's disease in 2 patients; however, most of the misdiagnoses were acute diseases. Symptoms of patients attributed to IBS are infrequently changed to another etiology over the long term.23 The high prevalence of diverticulosis and usual requirement of CT to confirm diverticulitis challenge any study of clinically diagnosed diverticulitis, retrospective or prospective. The predominant bowel pattern of the IBS patients was not determined, but all subtypes are characterized by abdominal pain.1 We did not investigate misdiagnosis in subjects without IBS.
Strengths of the study include large cohorts with validated methods of identifying physician-diagnosed IBS14 and diverticulitis15 that were assessed for a median of at least 10 years. We utilized comprehensive databases in a prepaid health care system, double-physician record review and objective evidence for revised diagnoses and exclusion of diverticulitis. We had computerized laboratory, radiology, pathology, physician diagnosis, and other data on all patients, enabling us to detect revised diagnoses by objective criteria. Agreement rates between colon imaging procedures range from 60% to 82%, but we accepted the presence or absence of diverticulosis revealed by any colon imaging procedure.18 We required absence of diverticulosis of any severity from all colon imaging studies in IBS patients with multiple procedures before and/or after initial diverticulitis diagnosis to classify them as not having diverticulosis. With this method, we considered some patients as having diverticulosis if an imaging test revealed diverticulosis several years after their initial diverticulitis diagnosis, even if multiple prediagnosis procedures reported no diverticulosis. Patients with negative imaging before initial diagnosis and no subsequent imaging could have developed diverticulosis before diagnosis. However, three quarters of patients classified as without diverticulosis had none reported on imaging after or both before and after diagnosis. Therefore, our strict definition of absent diverticulosis at any time likely classified some patients as having diverticulosis who did not have the disorder when diverticulitis was diagnosed. To minimize potential diagnostic bias related to a prior outpatient diagnosis, we assessed only the initial episodes in the IBS cohort. Our findings seem generalizable because similar proportions (about 70%) of diagnosed patients are managed as outpatients in our health care system and in a university system,5,6 and most outpatients with abdominal pain initially present to primary physicians.
Our findings are relevant to research and practice. Studies in which case finding includes outpatient clinical diagnoses could overestimate cases. In patients with chronic recurrent pain, physicians should be circumspect when a patient reports pain that was previously attributed to diverticulitis from clinical features alone.
Accepted practice calls for physicians to consider how IBS patients' abdominal pain and associated symptoms compare with their usual recurrent symptoms. Consideration of the psychosocial background and prior health care-seeking behavior, including amplified reporting of multiple symptoms and consultation24,25 is particularly important in patients with severe pain.26,27 However, based on clinical and laboratory findings alone8 both primary physicians and gastroenterologists will be uncertain as to whether some patients have diverticulitis.
How should physicians manage IBS patients with suspected diverticulitis? The American Gastroenterological Association suggested selective rather than the traditional routine use of antibiotics in uncomplicated diverticulitis,28 and additional data supported the safety of management without antibiotics.29 Although mistaken diagnosis of diverticulitis in IBS patients likely represents a minority of all outpatients treated for diverticulitis, avoiding antibiotic use in suspected diverticulitis would reduce the increased rates of antibiotic use and Clostridium difficile infection that we previously documented in the IBS cohort.30 Routine antibiotic treatment of diverticulitis may be more likely in the United States than in England where antibiotic use and Clostridium difficile infection have decreased. 31 It is prudent to manage selected outpatients with close observation and without antibiotics after careful clinical evaluation and relevant laboratory testing. The mean duration of episodically increased abdominal pain in IBS is 3 days.32 Failure to improve could lead to consideration of other tests and/or antibiotic treatment.
In conclusion, diverticulitis was diagnosed much more often in outpatients with IBS than those without IBS. This finding was partly attributable to mistaken attribution of presenting features of other diseases to diverticulitis. In other patients, absence of diverticulosis indicated misdiagnosis. Although the findings revealed misdiagnosis in about 1 of 5 patients, we speculate that additional patients had misattribution of abdominal pain and tenderness to diverticulitis. In view of the common uncertainty of outpatient diverticulitis diagnosis and safety of treating many documented cases without antibiotics, it is advisable to consider withholding these drugs in suspected cases. Further research could aim to identify clinical features that improve the accuracy of clinical diagnosis in primary care.
Appendix

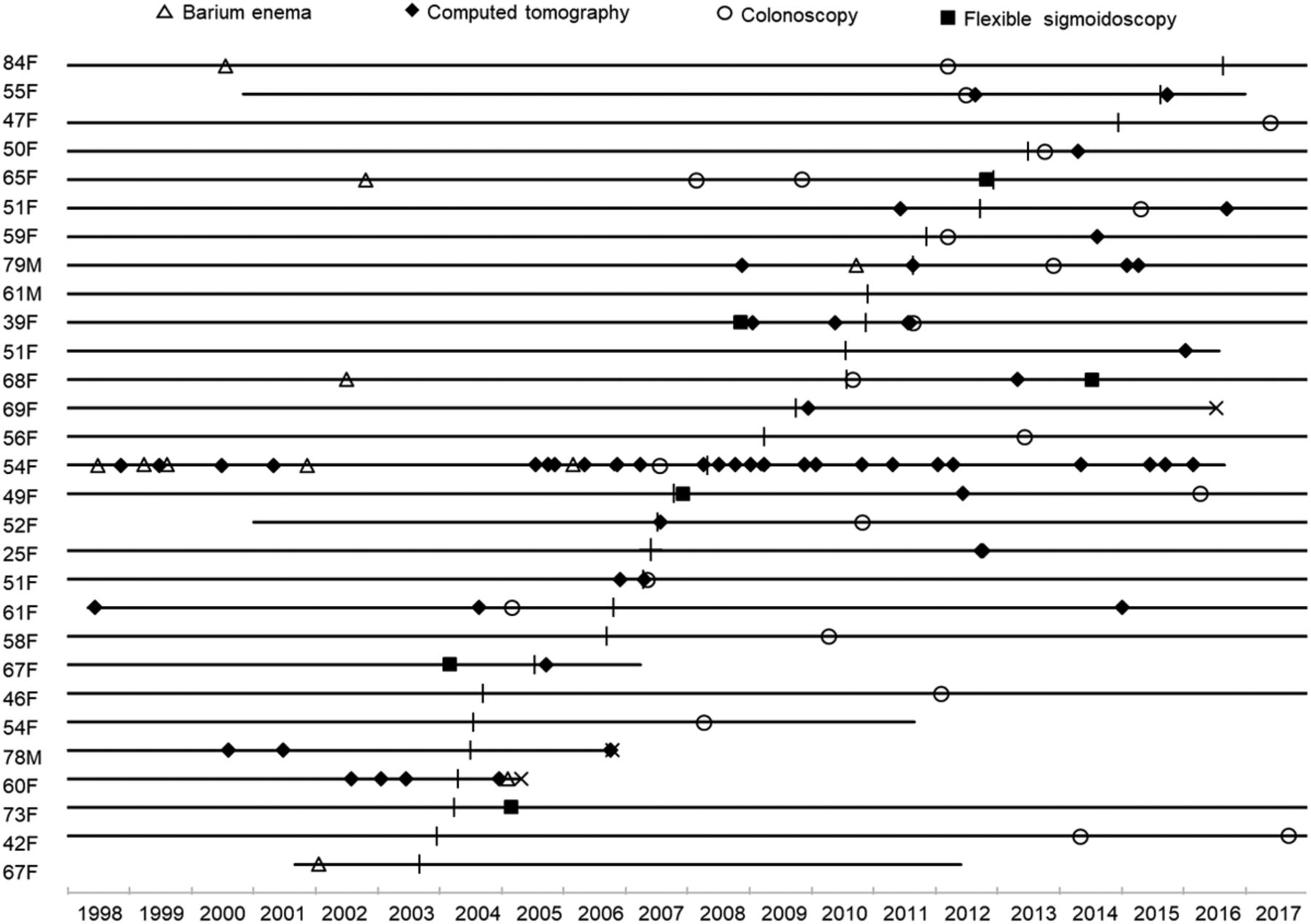
Colon radiologic and endoscopic imaging procedures that revealed no diverticulosis in 29 outpatients with irritable bowel syndrome whose presenting symptoms were treated with antibiotics as diverticulitis and not revised to another etiology or excluded by computed tomography. Individual patients are indicted by horizontal lines depicting health plan membership. Lines beginning at the onset of 1998 indicate membership starting then or earlier, and a terminal “x” indicates death. Age is at diagnosis of diverticulitis. F, female; M, Male.
Notes
This article was externally peer reviewed.
Funding: Kaiser Permanente–Southern California internal research funding.
Conflicts of interest: The authors deny any conflicts of interest.
To see this article online, please go to: http://jabfm.org/content/33/4/549.full.
- Received for publication September 17, 2019.
- Revision received January 28, 2020.
- Accepted for publication January 29, 2020.




{kind=link}
{kind=link}
{kind=link}
{kind=link}