
Article Figures & Data
Figures
- Figure 1.
Average National Quality Forum quality care metrics (QM) scores reported over the period 2011 to 2013 for the chronic care (left), preventive care (middle), and mental health care domains (right), stratified by practices with high and low case mix. P values designate statistical significance of the average total change from 2011 to 2013.
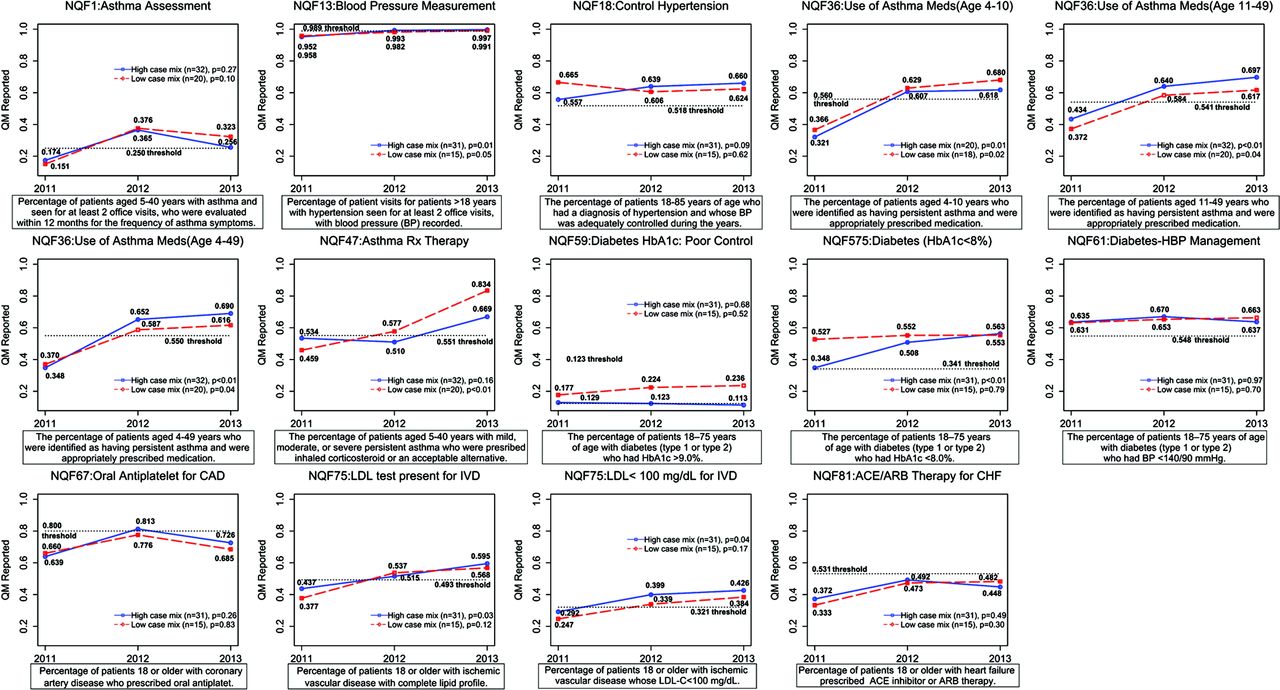
- Appendix Figure 1.
Chronic care domain: average National Quality Forum (NQF) quality metrics (QM) scores reported for 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the mean total change from 2011 to 2013.
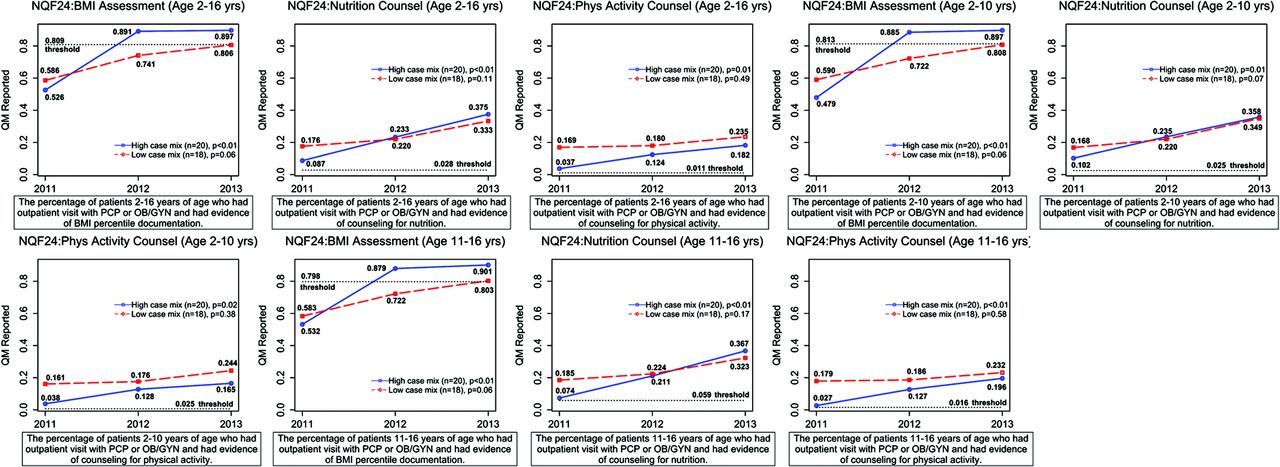
- Appendix Figure 2.
Preventive care domain (body mass index assessment, physical activity counseling, and nutrition counseling for children): average National Quality Forum (NQF) quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.
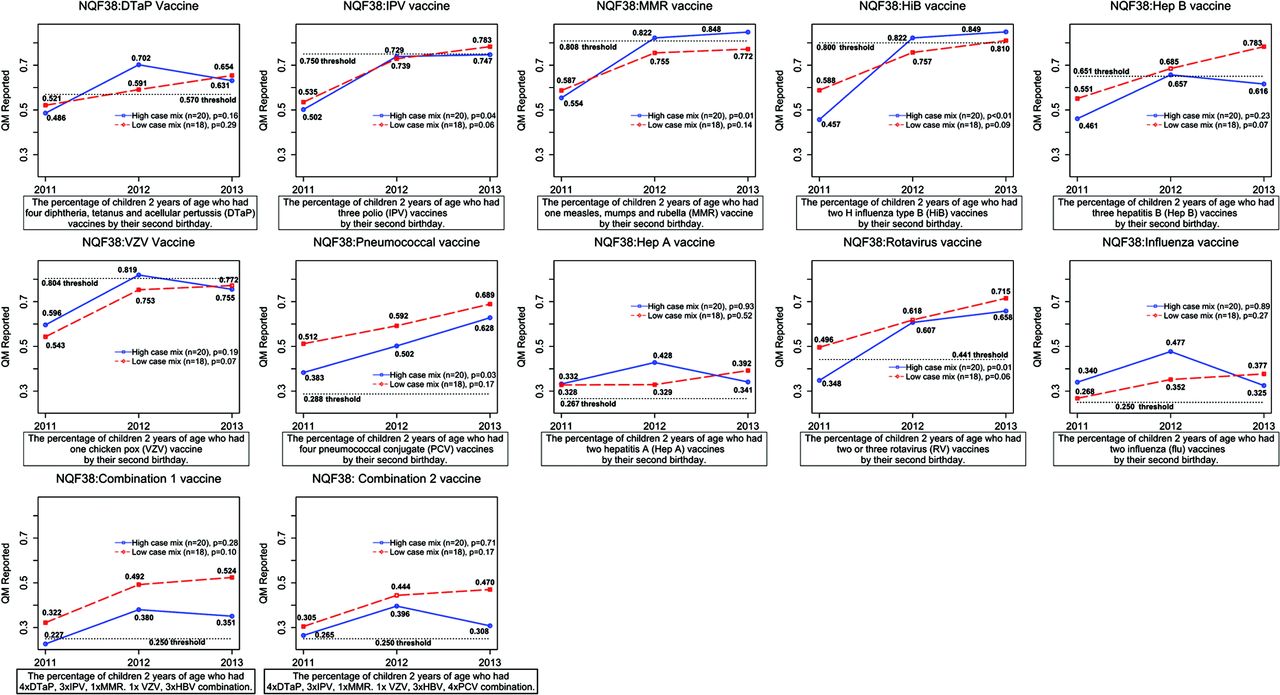
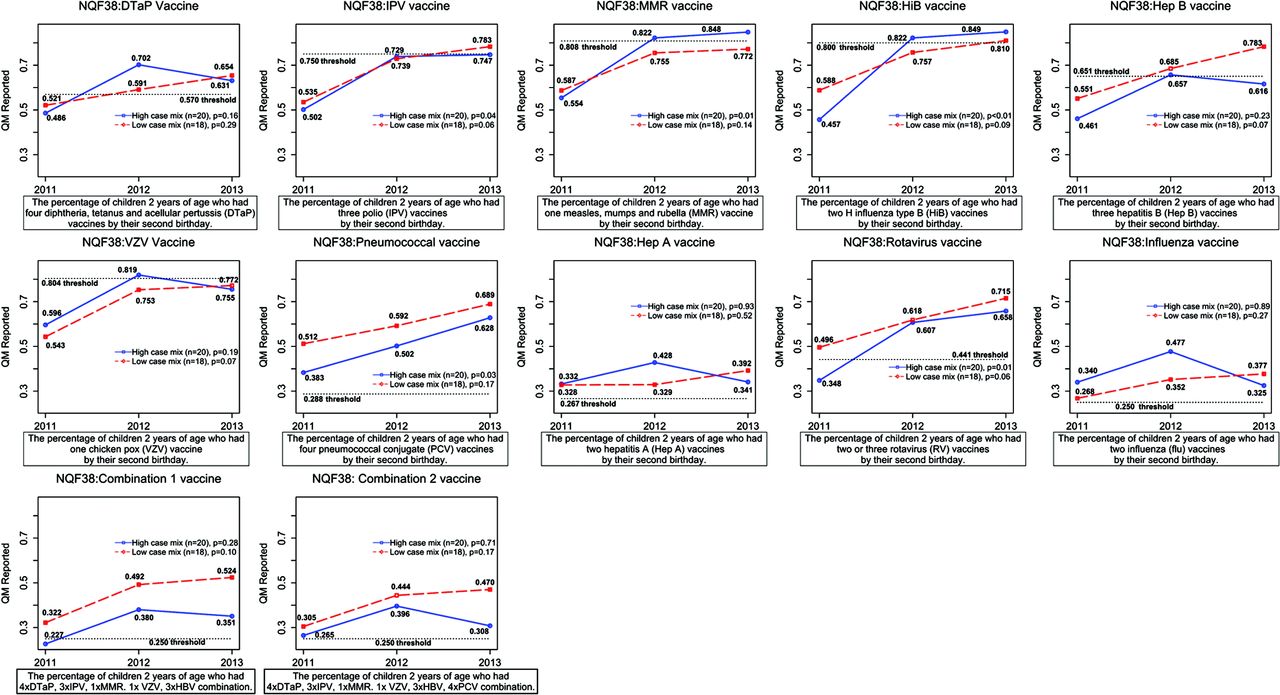
- Appendix Figure 3.
Preventive care domain (children's vaccinations): average National Quality Forum (NQF) quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.
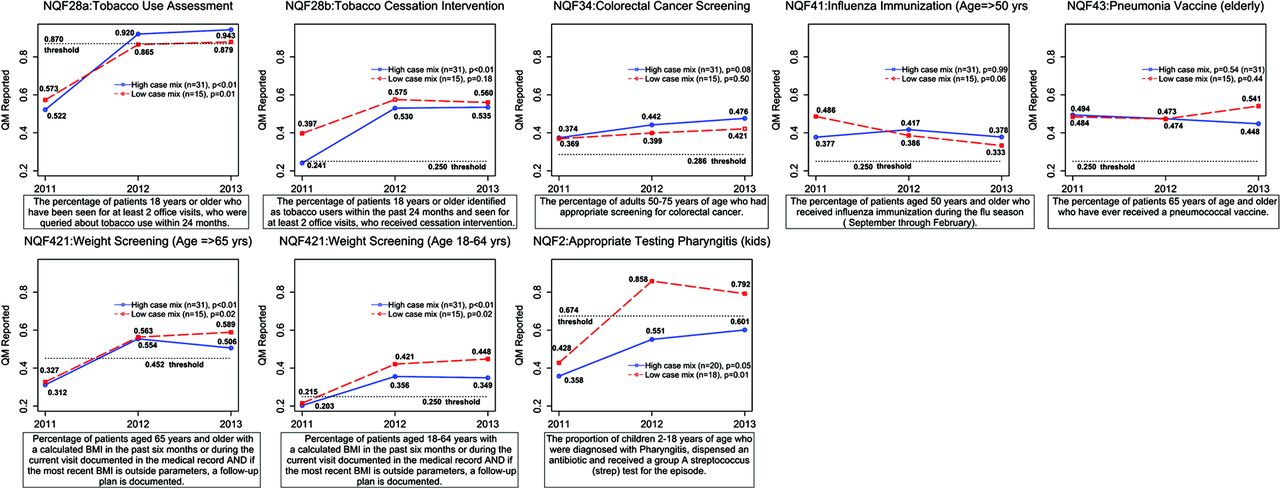
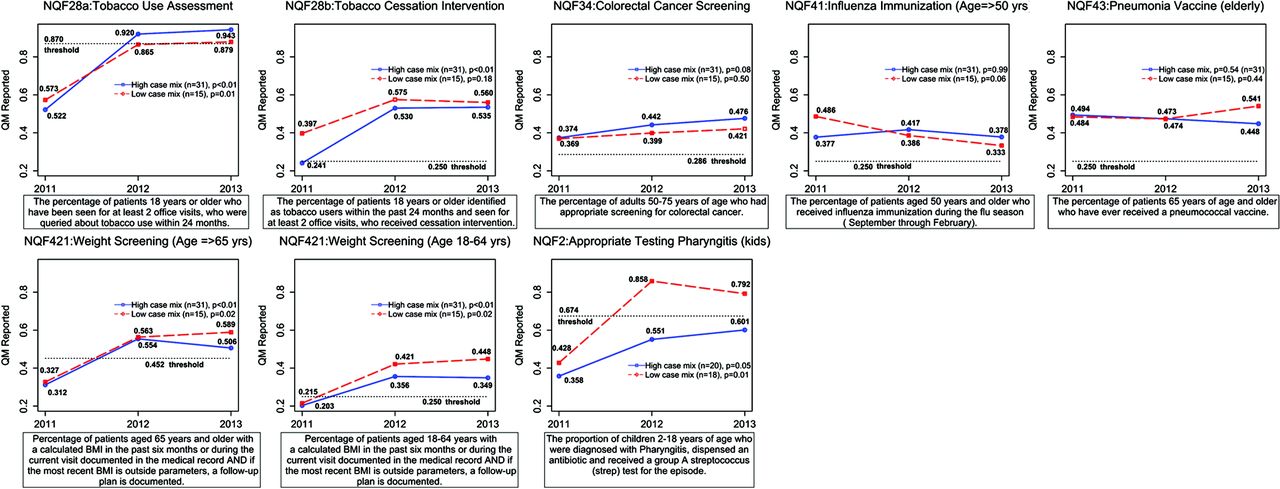
- Appendix Figure 4.
Preventive care domain (remaining metrics): average National Quality Forum (NQF) quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.
- Appendix Figure 5.
Health care domain: average quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.



Tables
- Table 1. Description of National Quality Forum Quality Metric Measures Reported By Patient Centered Medical Homes Practices (n = 52)*
Domain Designation Measure Number Measure Description† Type of Practice Reporting Chronic disease NQF 1 Percentage of patients aged 5–40 years with asthma seen for at least 2 office visits and who were evaluated within 12 months for the frequency of asthma symptoms Adult/pediatric/mixed NQF 13 Percentage of visits for patients >18 years old with hypertension seen for at least 2 office visits, with BP recorded Adult/mixed NQF 18‡ Percentage of patients 18–85 years of age who had a diagnosis of hypertension and whose BP was adequately controlled during the years Adult/mixed NQF 36 Percentage of patients who were identified as having persistent asthma, were appropriately prescribed medication, and of the ages: N1D1: 4–10 years
N2D2: 11–49 years
N3D3: 4–49 years
Adult/pediatric/mixed NQF 47 Percentage of patients aged 5–40 years with mild, moderate, or severe persistent asthma who were prescribed inhaled corticosteroid or an acceptable alternative Adult/pediatric/mixed NQF 59‡ Percentage of patients 18–75 years of age with diabetes (type 1 or type 2) who had HbA1c >9.0% Adult/mixed NQF 61 Percentage of patients 18–75 years of age with diabetes (type 1 or type 2) who had BP <140/90 mm Hg Adult/mixed NQF 67 Percentage of patients with coronary artery disease, ≥18 years old, who were prescribed an oral antiplatelet agent Adult/mixed NQF 75 Percentage of patients with ischemic vascular disease, ≥18 years old, who: N1D1: were tested for complete lipid profile
N2D1: have LDL <100 mg/dL
Adult/mixed NQF 81 Percentage of patients with heart failure, ≥18 years old, and prescribed an ACE inhibitor or ARB therapy Adult/mixed NQF 575‡ Percentage of patients 18–75 years of age with diabetes (type 1 or type 2) who had HbA1c <8.0% Adult/mixed Preventive care NQF 24 Percentage of patients aged 2–16 years of age who had outpatient visit with a PCP or OB/GYN and had evidence of: N1D1: BMI percentile documentation
N2D1: nutrition counseling
N3D1: physical activity counseling
N1D2: BMI percentile documentation (age 2–10 years)
N2D2: nutrition counseling (age 2–10 years)
N3D2: physical activity counseling (age 2–10 years)
N1D3: BMI percentile documentation (age 11–16 years)
N2D3: nutrition counseling (age 11–16 years)
N3D3: physical activity counseling (age 11–16 years)
Pediatric/mixed NQF 0028a‡ The percentage of patients, who are ≥18 years of age, have been seen for at least 2 office visits, and who were queried about tobacco use within 24 months Adult/mixed NQF 0028b‡ The percentage of patients, who are ≥18 years of age, have been seen for at least 2 office visits, and who received cessation intervention Adult/mixed NQF 34 Percentage of adults 50–75 years of age who had appropriate screening for colorectal cancer Adult/mixed NQF 38 The percentage of children 2 years of age who had the following vaccines and/or their combinations by their 2nd birthday: N1D1: diphtheria, tetanus, acellular pertussis (4× DTaP)
N2D1: polio (IPV)
N3D1: measles, mumps, rubella (MMR)
N4D1: H influenza type B (2× HIB)
N5D1: hepatitis B (3× HBV)
N6D1: chicken pox (VZV)
N7D1: pneumonococcal conjugate (4× PCV)
N8D1: hepatitis A (2× Hep A)
N9D1: rotavirus vaccines (2/3× RV)
N10D1: influenza vaccines (2)
N11D1: combination 1 (4× DTaP, 3× IPV, 1× MMR, 1× VZV, 3× HBV)
N12D1: combination 2 (4× DTaP, 3× IPV, 1× MMR, 1× VZV, 3× HBV, 4× PCV)
Pediatric/mixed NQF 41 Percentage of patients aged ≥50 years old who received influenza immunization during the flu season (September through February). Adult/mixed NQF 43 Percentage of patients ≥65 years old who have ever received a pneumococcal vaccine Adult/mixed NQF 421 Percentage of patients aged 18 to ≥65 years with a calculated BMI in past 6 months or during the current visit documented AND, if the most recent BMI is outside parameters, a follow-up plan is documented Adult/mixed NQF 2 Percentage of children 2–18 years of age who were diagnosed with pharyngitis, dispensed an antibiotic, and received a group A streptococcus (strep) test for the episode. Pediatric/mixed Mental health NQF 105 Percentage of patients ≥18 years old who were diagnosed with a new episode of major depression and dispensed antidepressant medication for: N1D1: ≥84 days after diagnosis
N2D1: ≥180 days after diagnosis
Adult/mixed ↵* The 52 practices comprised 6 pediatric, 14 adult, and 32 mixed practices.
↵† In the descriptions, the N represents the numerator and D, the denominator. In these measures the denominator typically consists of patient characteristics such as age and, occasionally, a diagnosed disease condition, whereas the numerator indicates access to a health care service (eg, screening, counseling, prescription of medication) or treatment success.
↵‡ This National Quality Forum (NQF) quality metric was measured by practices under the Million Hearts initiative.
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BMI, body mass index; BP, blood pressure; LDL, low-density lipoprotein; OB/GYN, obstetrician/gynecologist; PCP, primary care physician.
- Table 2. Maryland Multi-Payor Patient Centered Medical Home Program Practice Characteristics, 2011 (n = 52)
Practices No. % Practice type Adult 14 26.92 Mixed 32 61.54 Pediatric 6 11.54 Case mix High 32 61.54 Low 20 38.46 NCQA practice level Deemed level I 43 82.69 Level III 9 17.31 Shared savings eligibility 30% share 10 19.23 40% share 22 42.31 50% share 20 38.46 Rural (federal designation) No 48 92.31 Yes 4 7.69 Telemedicine (rural) No 32 61.54 Yes 20 38.46 Health information exchange No 9 17.31 Yes 43 82.69 Practice size 1 to 5 providers 23 44.23 6 to 10 providers 22 42.31 11 or more providers 7 13.46 Patient age, years (mean) 0–18 25.90 19–49 43.09 ≥50 33.59 Medicaid patients (mean) 27.65 Male patients (mean) 41.29 Fixed transformation payment (mean) 4.70 Inpatient length of stay/1000 (median) 225.5 Emergency visits/1000 (median) 220.0 Readmission visits (30 day)/1000 (median) 3.8 NCQA, National Committee for Quality Assurance.
- Table 3. Univariate Analysis of Effect of Practice Characteristics on Reported National Quality Forum Metrics Scores, Controlling for Measurement Year
Characteristics Chronic Care Domain (n = 52) Preventive Care Domain (n = 52) Mental Health Care Domain (n = 46) Coefficient P Value Coefficient P Value Coefficient P Value Case mix High (ACG ≥2.5) −0.007 .84 −0.007 .83 0.039 .61 Low (ACG <2.5) Reference Reference Reference Practice type Pediatric 0.10 .16 0.07 .31 −0.07 .35 Mixed −0.05 .19 0.03 .52 — Adult Reference Reference Reference NCQA practice level Deemed level I 0.03 .46 −0.06 .15 0.21 .03 Level III Reference Reference Reference Shared savings eligibility 30% share −0.16 <.0001 −0.01 .74 −0.09 .10 40% share −0.12 .001 −0.03 .39 −0.08 .33 50% share Reference Reference Reference Rural (federal designation) Yes −0.05 .06 −0.10 .02 −0.07 .31 No Reference Reference Reference Rural (use of telemedicine) Yes 0.04 .26 −0.02 .62 0.08 .22 No Reference Reference Reference Health information exchange Yes 0.03 .49 0.02 .70 0.09 .42 No Reference Reference Reference Practice size (no. providers) 1–5 0.00 .98 −0.14 .02 −0.02 .85 6–10 0.01 .82 −0.06 .30 0.01 .94 ≥11 Reference Reference Reference Age ≥50 (mean %) High (top quartile: 0.444< and ≤0.722) 0.08 .06 −0.01 .86 0.20 .04 Medium (intermediate quartiles: 0.238< and ≤0.444) 0.00 .97 −0.02 .69 0.08 .41 Low (bottom quartile: ≤0.238) Reference Reference Reference Medicaid patients (mean %) High (top quartile: 0.422< and ≤0.938) −0.02 .70 0.03 .63 −0.18 .08 Medium (intermediate quartiles: 0.08< and ≤0.422) −0.06 .16 −0.03 .51 −0.17 .02 Low (bottom quartile: ≤0.08) Reference Reference Reference Male patients (mean %) High (top quartile: 0.470< and ≤0.586) 0.04 .36 0.04 .37 −0.04 .69 Medium (intermediate quartiles: 0.3674< and ≤0.470) 0.02 .50 0.01 .80 0.00 .95 Low (bottom quartile: ≤0.3674) Reference Reference Reference Fixed transformation payment (2011) High (>4.68) −0.03 .46 0.06 .15 −0.21 .03 Low (≤4.68) Reference Reference Reference Inpatient length of stay (2011) High (top quartile: 280< and ≤622 per 1000) −0.05 .23 0.02 .62 0.00 .97 Medium (intermediate quartiles: 148< and ≤280 per 1000) −0.06 .13 −0.03 .40 0.09 .14 Low (bottom quartile: ≤148 per 1000) Reference Reference Reference Emergency department visits (2011) High (top quartile: 302.5< and≤702) 0.06 .17 −0.003 .95 0.09 .29 Medium (intermediate quartiles: 190< and ≤302.5 per 1000) 0.03 .40 −0.01 .75 0.00 .97 Low (bottom quartile: ≤190 per 1000) Reference Reference Reference Readmission visits (2011) High (top quartile: ≤2.56 per 1000) −0.06 .12 0.05 .10 0.05 .60 Medium (Intermediate quartiles: 2.56< and ≤7.321 per 1000) −0.06 .07 −0.01 .85 0.00 .98 Low (bottom quartile: 7.321< and ≤20.4 per 1000) Reference Reference Reference ACG, adjusted clinical group; NCQA, National Committee for Quality Assurance. Bold values denote statistically significant values, at the 0.05 level.
- Table 4. Multivariate Fixed Effects Analysis of Determinants of Reported National Quality Forum Scores By Maryland Multi-Payor Patient Centered Medical Home Program Practices
Chronic Care Domain (n = 52) Preventive Care Domain (n = 52) Mental Health Care Domain (n = 46) Change P Value Change P Value Change P Value Change from 2011–2012 0.14 <.0001 0.15 <.0001 0.34 <.0001 Change from 2012–2013 0.03 .06 0.04 .05 0.07 .12 Practice type Pediatric 0.12 .04 0.08 .13 — — Mixed 0.03 .22 0.04 .33 0.11 .22 Adult Reference Reference Reference Shared savings eligibility 30% or 40% (vs 50%) −0.11 .01 −0.06 .15 −0.04 .48 Patients aged ≥50 years (mean %) High (vs medium/low) 0.07 .02 — — 0.19 .04 Practice size ≥6 providers (vs <6) — — 0.09 .05 — — Rural (federal designation) −0.11 .03 −0.07 .09 −0.09 .26 Medicaid patients (2011) (%) High/medium (vs low) — — — — −0.14 .05 Readmission visits per 1000 (2011) High (vs. medium/low) −0.03 .24 0.06 .03 — — “High” designates the top quartile of variable distribution; “medium” designates the interquartile range (Q25–Q75) of the variable distribution; and “low” designates the bottom quartile of variable distribution. Bold values denote statistically significant values, at the 0.05 level.
—, Variable is not included in the model.
- Appendix Table 1. Maryland Multi-Payor Patient Centered Medical Home Program Practice Characteristics By High and Low Case Mix
High Case Mix (n = 32) Low Case Mix (n = 20) P Value No. % No. % Practice type Adult 12 37.5 2 10.0 Mixed 19 59.4 13 65.0 .01 Pediatric 1 3.1 5 25.0 Rural (federal designation) No 30 93.8 18 90.0 .63 Yes 2 6.3 2 10.0 Use of telemedicine No 19 59.4 13 65.0 .77 Yes 13 40.6 7 35.0 NCQA Practice level Deemed level I 26 81.3 17 85.0 .73 Level III 6 18.8 3 15.0 Shared savings eligibility 30% share 6 18.8 4 20.0 .57 40% share 12 37.6 10 50.0 50% share 14 43.8 6 30.0 Health information exchange No 4 12.5 5 25.0 .28 Yes 28 87.5 15 75.0 Practice size (no. providers) 1–5 15 46.9 8 40.0 .65 6–10 12 37.5 10 50.0 ≥11 5 15.6 2 10.0 Medicaid patients (mean %) 13.0 24.6 .04 Mean age, years (%) 0–18 17.1 40.0 .01 19–49 45.7 39.0 .20 ≥50 37.2 26.3 .02 NCQA, National Committee for Quality Assurance.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}