
Abstract
Background: We present data on quality of care (QC) improvement in 35 of 45 National Quality Forum metrics reported annually by 52 primary care practices recognized as patient-centered medical homes (PCMHs) that participated in the Maryland Multi-Payor Program from 2011 to 2013.
Methods: We assigned QC metrics to (1) chronic, (2) preventive, and (3) mental health care domains. The study used a panel data design with no control group. Using longitudinal fixed-effects regressions, we modeled QC and case mix severity in a PCMH.
Results: Overall, 35 of 45 quality metrics reported by 52 PCMHs demonstrated improvement over 3 years, and case mix severity did not affect the achievement of quality improvement. From 2011 to 2012, QC increased by 0.14 (P < .01) for chronic, 0.15 (P < .01) for preventive, and 0.34 (P < .01) for mental health care domains; from 2012 to 2013 these domains increased by 0.03 (P = .06), 0.04 (P = .05), and 0.07 (P = .12), respectively. In univariate analyses, lower National Commission on Quality Assurance PCMH level was associated with higher QC for the mental health care domain, whereas case mix severity did not correlate with QC. In multivariate analyses, higher QC correlated with larger practices, greater proportion of older patients, and readmission visits. Rural practices had higher proportions of Medicaid patients, lower QC, and higher QC improvement in interaction analyses with time.
Conclusions: The gains in QC in the chronic disease domain, the preventive care domain, and, most significantly, the mental health care domain were observed over time regardless of patient case mix severity. QC improvement was generally not modified by practice characteristics, except for rurality.
Patient-centered medical homes are an important building block for health care reform and a mechanism for achieving quality improvement.1,2 Patient-centered interactions with optimal utilization of health information technology and primary care teams have potential for enhancing chronic disease management and the delivery of preventive care.3⇓–5 Patient-centered care management has been demonstrated to enhance the quality of care (QC) delivered and chronic disease management.6,7 Patient-centered medical home (PCMH) capacity enhancements lead to potential impacts on the behavioral health care of patients overall and, in particular, on patients with high utilization and with a high probability for the coexistence of anxiety and depression.8
Quality improvements are critical to advanced primary care models within PCMHs and are frequently linked to shared savings and lowering the total costs of care.9 Impact on quality may vary by practice characteristics, including a practice's ability to change, the population served, and the disease burden among the population served.10 For example, research on multimorbidity has identified the patient case mix as one of the measures for testing their validity in relation to expected patient association characteristics and outcomes.11,12 There are, however, gaps in the literature on whether quality improvement in a PCMH varies by patient and practice characteristics, as well as which characteristics most strongly influence quality. To explore the link between patient and practice characteristics and QC delivered, this study was conducted in the 52 PCMHs (14 adult, 32 mixed adult and pediatric, and 6 pediatric practices) that are located in community settings and that volunteered to participate in the Maryland Multi-Payor Program (MMPP).13,14
Each PCMH is recognized by the National Commission on Quality Assurance (NCQA), has established primary care teams and care management procedures, and the majority are linked to the state-designated health information exchange to receive data on patient utilization of hospital and emergency departments. All PCMHs annually self-report quality metrics to the MMPP through a Web-based portal, and they benefit from linked shared savings based on the achievement of quality thresholds.15 Practices also receive learning support provided by the Maryland Learning Collaborative to create a forum for collaborating, sharing evidence-based practices, supporting quality improvement, disseminating the state's advanced primary care model, and assisting data extraction by conducting electronic health record user groups to optimize NQF metric extraction using preset specifications.13,14,16 In addition, quality improvement and health care utilization formed the basis for each practice's eligibility for shared savings from commercial and public insurance carriers.15 This article presents observations in quality improvement in the 52 primary care practices that are recognized as PCMHs, and conducts an exploratory analysis of patient and practice characteristics that determine quality improvement.
Methods
The study uses a panel data design with no control group. Data on 45 quality metrics were available for 52 practices for the years 2011 (baseline), 2012, and 2013. We categorized the quality metrics into 3 domains: (1) chronic care domain (metrics related to asthma assessment and appropriate use of medications, blood pressure and heart disease measurement and management, diabetes control); (2) preventive care domain (in children and adolescents: body mass index assessment, nutrition counseling, physical activity counseling, and vaccinations; in adults: tobacco use assessment and cessation intervention, vaccinations, colorectal cancer screening, and weight screening); and (3) mental health care domain (2 metrics related to antidepressant use among adults) (Table 1). Not all 52 practices reported measurement of each individual quality care metric because metrics were applicable to different types of patient populations served by primary care practices (pediatric, adult, or mixed). Quality metrics reported by practices annually over a period of 3 years were analyzed for each of the chronic disease, preventive, and mental health care domains, as well as by each individual metric.
All practice characteristics were measured in the baseline year 2011 and included practice type (adult, pediatric, or mixed) and size, NCQA 2008/2011 PCMH level, level of shared savings eligibility, location in a rural versus urban region, use of telemedicine, participation in the state's health information exchange, and the patient distribution at each practice (by age, sex, and source of insurance). In addition, we examined the amount of fixed transformation payment (determined by a variety of factors, such as size of practice, number of patients, and NCQA level), as well as health care utilization, calculated per 1000 patients, for inpatient length of stay, emergency visits, and 30-day readmission visits.
The case-mix severity of each practice population was calculated using the well-established Johns Hopkins Adjusted Clinical Groups (ACG) Case-Mix System.11,12,17 Using available 2010 administrative claims data for primary and specialty ambulatory care, inpatient care, and pharmacy for each patient assigned to a practice, 1 of approximately 90 ACGs was assigned to each individual, reflecting morbidity burden and expected resource use. These mutually exclusive categories then were combined into 1 of 5 broad “resource use bands” (RUBs), which ranged from “healthy” (1) to “very high risk” (5).17 A practice case-mix score was calculated based on the distribution of patients assigned to each PCMH within each of these 5 ACG-based RUB categories. Thus the lowest possible score was 1 and the highest 5.
Statistical Analysis
We broke down the distribution of continuous practice characteristics into categorical variables approximating the empirical quartile or half points of the distribution. For example, practices were categorized into low and high case-mix severity practices according to whether their ACG case-mix value fell below or above the median ACG-based RUB case-mix score determined by the morbidity mix of the individual patients assigned to the practice.
In descriptive analyses the overall average change from 2011 to 2013 was calculated and tested for statistical significance using Student t test. When examining changes by individual quality care metrics, we additionally compared quality metric scores by the achievement threshold criterion, defined as the 25th percentile for performance among the MMPP practices. In univariate analyses, using longitudinal fixed-effects regressions controlling for the measurement year (Proc Mixed procedure in SAS version 9.2; SAS Institute, Cary, NC), we modeled the association between practice characteristics and the annual calculated score for each of the 3 quality health care domains (Online Appendix Table 1).
Selecting only those variables that were significant at P ≤ .20, we conducted multivariate, longitudinal, fixed-effects regression for each quality health care domain and determined the best model fit using the Akaike information criterion. Using interaction terms with the follow-up measurement years (2012 to 2013), we examined whether the change in quality score from 2011 was modified by practice characteristics. Given the small sample size of the practices included, we considered findings with P ≤ .05 to be statistically significant, whereas .05 < P ≤ .10 represented some evidence of an association.
Results
More than three quarters of practices were deemed NCQA practice level I in 2011. By 2012, each practice was recognized as a PCMH: 15 practices were NCQA level 2 and 37 practices were NCQA level 3. About 8% of practices were rural, 83% participated in the state's health information exchange, and 13.5% were large practices with ≥11 providers each (Table 2). The practices' average ACG-based RUB case-mix score ranged from 1.14 to 2.96 for the practices with a “low” case mix, and from 2.97 to 3.83 for those with a “high” case mix. The average proportion of patients on Medicaid (vs commercial insurance) was 27.7%, which correlated with a higher proportion of patients ≤18 years of age in the practice. Based on quality improvement, reduction of utilization and total costs of care, one fifth of practices were eligible for 30% of shared savings, with the remaining proportion of practices equally distributed between 40% and 50% shared savings eligibility in 2011.
We observed significant increases in the reported QC metrics for all 3 QC domains (Figure 1). For the chronic care domain, the average NQF quality metrics score increased from 0.417 to 0.568 for practices with a high case mix (δ = 0.150; P = .01) and from 0.401 to 0.596 for practices with a low case mix (δ = 0.195; P = .01). Similarly, for the preventive care domain, practices with high and low case mixes exhibited an increase from 0.330 to 0.540 (δ = 0.210; P = .01) and 0.386 to 0.553 (δ = 0.167; P = .02), respectively. Positive overall change was also observed with respect to the mental health care domain in practices with a high case mix (from 0.268 to 0.698; δ = 0.429; P < .01) and a low case mix (from 0.271 to 0.649; δ = 0.377; P = .01). Please refer to Online Appendix and Appendix Figures 1 through 5 for a discussion of results regarding change in quality by individual NQF metrics.

Average National Quality Forum quality care metrics (QM) scores reported over the period 2011 to 2013 for the chronic care (left), preventive care (middle), and mental health care domains (right), stratified by practices with high and low case mix. P values designate statistical significance of the average total change from 2011 to 2013.
In univariate regression analyses controlling for measurement year (Table 3), lower levels of shared savings eligibility (for the chronic care domain), rural practices (for the chronic care and preventive care domains), a medium to high number of readmission visits (for the chronic care domain), practices of small size (for the preventive care domain), practices with a medium to high proportion of patients on Medicaid and with a high fixed transformation payment (for the mental health care domain) were associated with average lower QC scores. Higher QC scores correlated with a high proportion of patients 50 to 65 years of age (for the chronic care and mental health care domains), a high number of readmission visits (for the preventive care domain), and NCQA PCMH practice level I (for the mental health care domain). Burden of illness as measured by the dichotomous (high/low) case-mix designation was not associated with differential QC based on domains.
In multivariate analyses controlling for various practice characteristics (Table 4), the reported quality score increased from 2011 to 2012 by 0.14 (P < .01), 0.15 (P < .01), and 0.34 (P < .01) for the chronic care, preventive care, and mental health care domains, respectively. However, to a smaller extent, the quality score improved even more from 2012 to 2013 by 0.03 (P = .06), 0.04 (P = .05), and 0.07 (P = .12) for the chronic care, preventive care, and mental health care domains, respectively. A higher proportion of older patients was associated with higher QC scores for the chronic care and mental health care domains, whereas larger practices correlated with a trend for higher QC scores in the preventive care domain. Interestingly, practices with a higher proportion of readmission visits were associated with a lower reported quality for the chronic care domain but higher quality for the preventive care domain.
In an analysis including interaction terms with time, despite having a 0.16 lower quality score in the baseline year (2011) than urban practices (for the chronic care domain), rural practices trended toward an average of 0.05 (P = .08) higher annual quality increase over 2011 to 2013 for the chronic care domain. Interaction terms between time and rurality were not significant in analyses for the preventive care domain (0.06; P = .28) and mental health care domain (0.04; P = .35). We did not detect differential quality improvement with respect to other practice characteristics.
Discussion
In this 3-year study of 52 PCMH sites, 35 of 45 quality metrics reported by the 52 PCMHs demonstrated improvement. Importantly, case-mix severity did not affect the achievement of quality improvement. The gains in quality occurred in the chronic disease domain, the preventive care domain, and, most significantly, in the mental health care domain.
There is limited literature on the impact of patient population on quality gains. Quality improvement in a PCMH includes enhanced management of diabetes, heart disease, and other chronic and mental diseases, which are relevant to care transitions and prevention of readmissions.7,8 Enhanced prevention of disease is expected to affect patients downstream by lowering the severity of chronic disease and reducing utilization. Our report is consistent with recent reports from primary care practices transformed to PCMHs, which report gains in access, quality, and chronic disease metrics.18,19 Our results also are consistent with small primary care practices that report gains in efficiency of the practice in addition to quality gains.20 Other published reports have presented equivocal data on quality gains and cost savings.10
Limitations
One of the limitations noted was the small number of participating practices and the notable lack of a control group. Although a control cohort was identified by the MMPP using propensity matching to compare overall utilization, there was no collection of quality metrics by control practices. Thus, this article does not include an analysis using the same control practices. This is consistent with reports from other state-level programs where the use of control practices was used in various formats but not consistently across each domain.21,22 Another limitation is the limited observation period, from 2011 to 2013, which may include the period when practices were transforming to an NCQA-recognized PCMH and actual quality gains may be just starting to manifest. All NCQA-level achievement observations in the tables are from 2011/2012 in year 1, and ACG observations are also from 2011 data. Time-varying change in case-mix severity is not reflected in these observations. Since quality gains were used in calculation of shared savings for practices, it is possible that this may have motivated practices to consistently report quality data and for improvements in practice workflows. Although practice coaching was provided in addition to electronic health record user groups, the quality data were self-reported by practices, with limited support.
Quantification of case-mix severity of PCMH populations in this study used the ACG methodology to correlate to quality gains. Although the ACG system has been used in predictive modeling for future morbidity and health care utilization, the same ACG procedures provided the robust basis for the correlation of patient characteristics with PCMH quality improvement.
Practices that were measured for quality in this study were participating in the MMPP, where each practice had transformed to a PCMH and had been recognized by the NCQA. All practices participated in the Maryland Learning Collaborative, where local best practices were highlighted and each practice received limited practice coaching. In addition, practices had opportunities to teleconference with experts, had opportunities to learn evidence-based guidelines via webinars, and were recipients of disseminated Maryland health care policy. Practices did become eligible for shared savings if quality metrics and overall utilization and costs demonstrated containment. Thus practices may have been dually motivated to enhance quality through a reinvigorated focus on patient centered care and the opportunity for shared savings.15
Conclusion
Our study suggests that quality improvement consistently occurs in a PCMH with team-based care, care coordination, enhanced access, and efficiency, regardless of the patient case-mix severity burden. Patient factors summarized in case-mix severity do not affect the achievement of quality improvement in the majority of quality metrics for a PCMH. Thus becoming a PCMH is a robust systematic change in primary care practices to achieve higher QC delivery.
Acknowledgments
The authors gratefully acknowledge the editorial review and guidance provided by Johnathan Weiner, D.Ph. Professor of Health Policy & Management and Health Informatics, Johns Hopkins Bloomberg School of Public Health and Jill Marsteller, PhD, MPP, Assoicate Professor of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health in revision of this manuscript. As well, the authors acknowledge the efforts in all aspects of the submission, revisions and resubmission process of Priyanka Gaitonde, Doctoral Candidate in Pharmaceutical Health Services Research Department at the University of Maryland School of Pharmacy. The Maryland Health Care Commission (MHCC) established the Maryland Multi-Payor Patient Centered Medical Home Program in 2011 as required by Health-General Article §19-1A-01, et sequentes. The law required MHCC to develop a 3-year pilot, which aims to improve the health and satisfaction of patients and slow the growth of health care costs in Maryland, while supporting the satisfaction and financial viability of primary care providers in the state. The five largest commercial insurance carriers—CareFirst BlueCross BlueShield, United HealthCare, Aetna, Coventry, and CIGNA—are required to participate under the enabling legislation. TRICARE, a health care program for uniformed services members, also participates in the program. Maryland's Medicaid agency, the Health Care Financing Administration, supports reimbursement to Medicaid managed care organizations subject to existing budget constraints.
Appendix
In the chronic care domain, 8 of 14 metrics exhibited statistically significant increases in reported quality from 2011 to 2013 (Appendix Figure 1). Most metrics met the respective quality achievement threshold by the last year of measurement, with the exception of NQF67 (oral antiplatelet therapy for adult patients with coronary artery disease) and NQF81 (angiotensin-converting enzyme inhibitor or angiotensin receptor blocker therapy for adult patients with heart failure), for which we observed nonsignificant change over time. Furthermore, 8 quality metrics that had started below the achievement thresholds in the baseline year achieved or surpassed the threshold by year 2013 (blood pressure measurement, ischemic vascular disease patients with complete lipid profile and low-density lipoprotein cholesterol <100 mg/dL, and all metrics related to asthma assessment and medications).
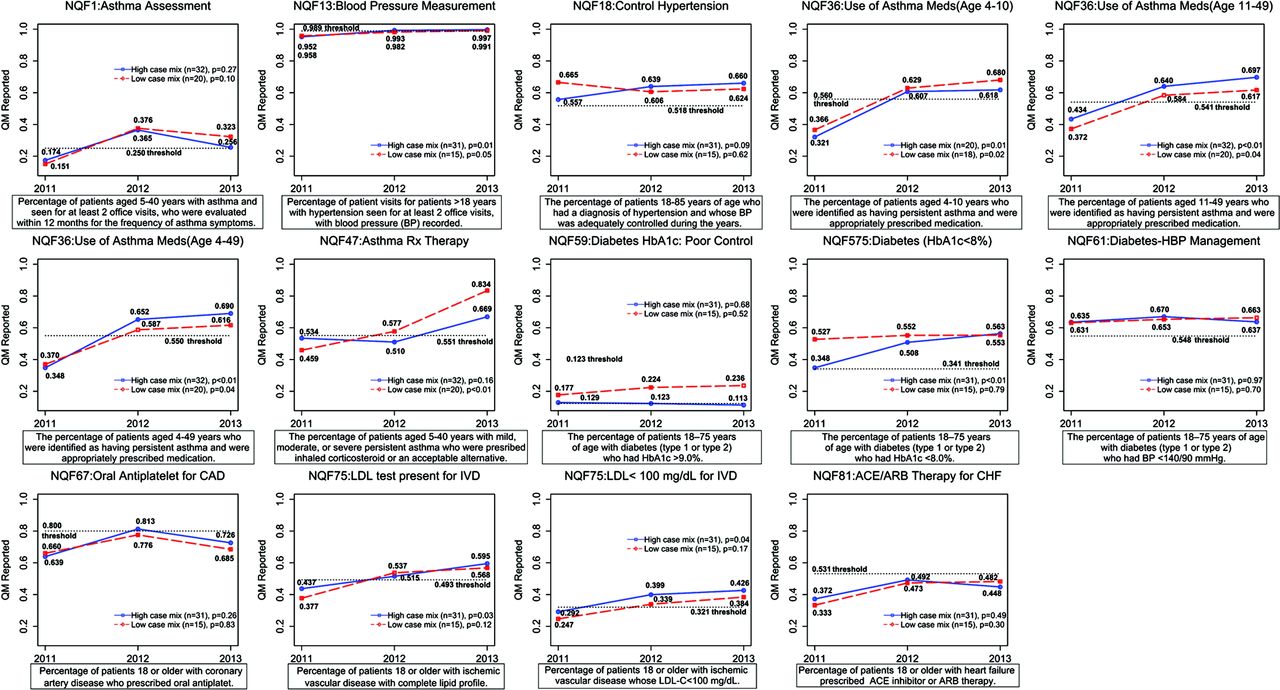
Chronic care domain: average National Quality Forum (NQF) quality metrics (QM) scores reported for 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the mean total change from 2011 to 2013.
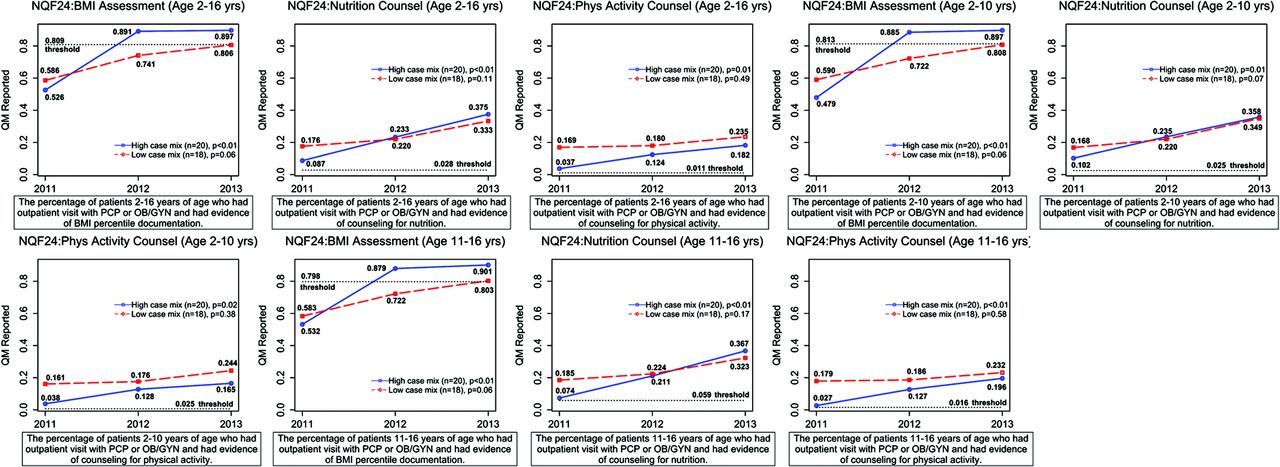
In the metrics belonging to the preventive care domain and related to body mass index assessment and nutrition and physical counseling for children and adolescents (Appendix Figure 2), we observed significant increases for all 9 metrics among practices with a high case mix (all 9 metrics above threshold by 2013) and for 4 of 9 metrics among practices with a low case mix (but again, all 9 were above the threshold or within an acceptable range by 2013).

Preventive care domain (body mass index assessment, physical activity counseling, and nutrition counseling for children): average National Quality Forum (NQF) quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.
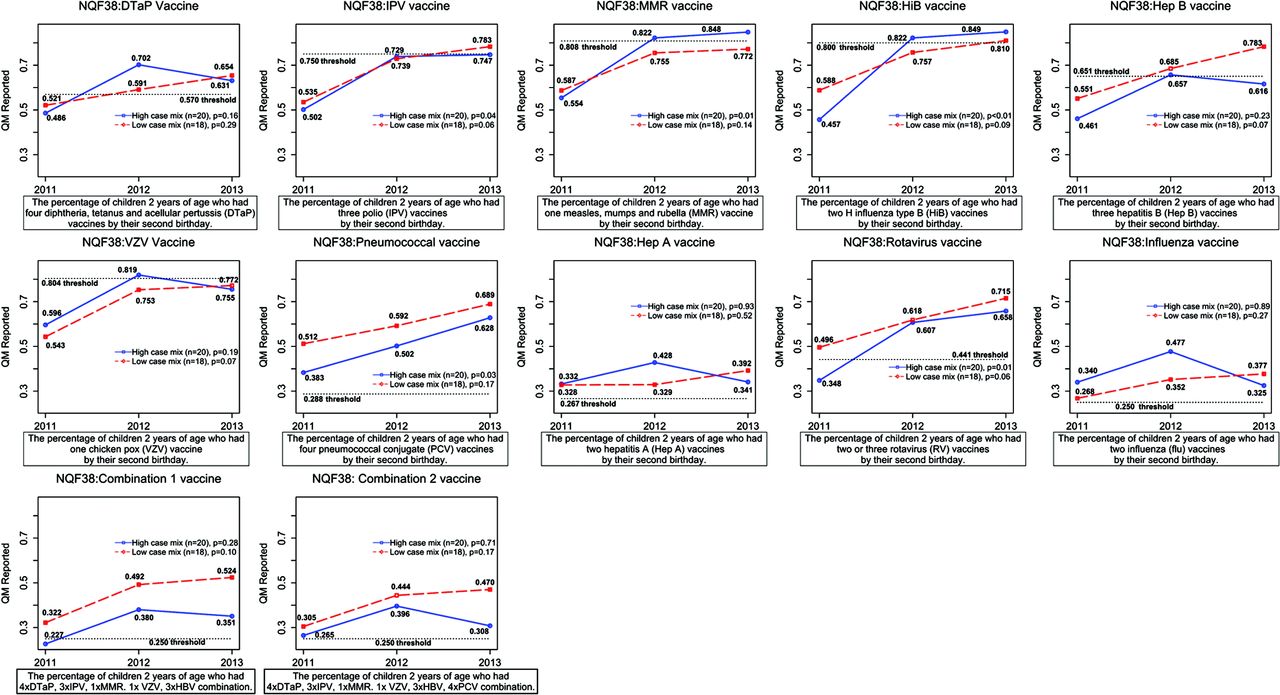
For pediatric vaccination metrics belonging to the preventive care domain (Appendix Figure 3), practices with a high and low case mixes had significant increases in 5 of 12 and 6 of 12 reported metrics, respectively: chicken pox, hepatitis B, combination 1 (low case-mix practices only); measles, mumps, and rubella and pneumococcal conjugate (high case-mix practices only); and polio, Haemophilus influenza type B, and rotavirus (all practices). All metrics, with 6 starting below the achievement threshold in the baseline year, had values surpassing or within an acceptable range of the achievement threshold by 2013.
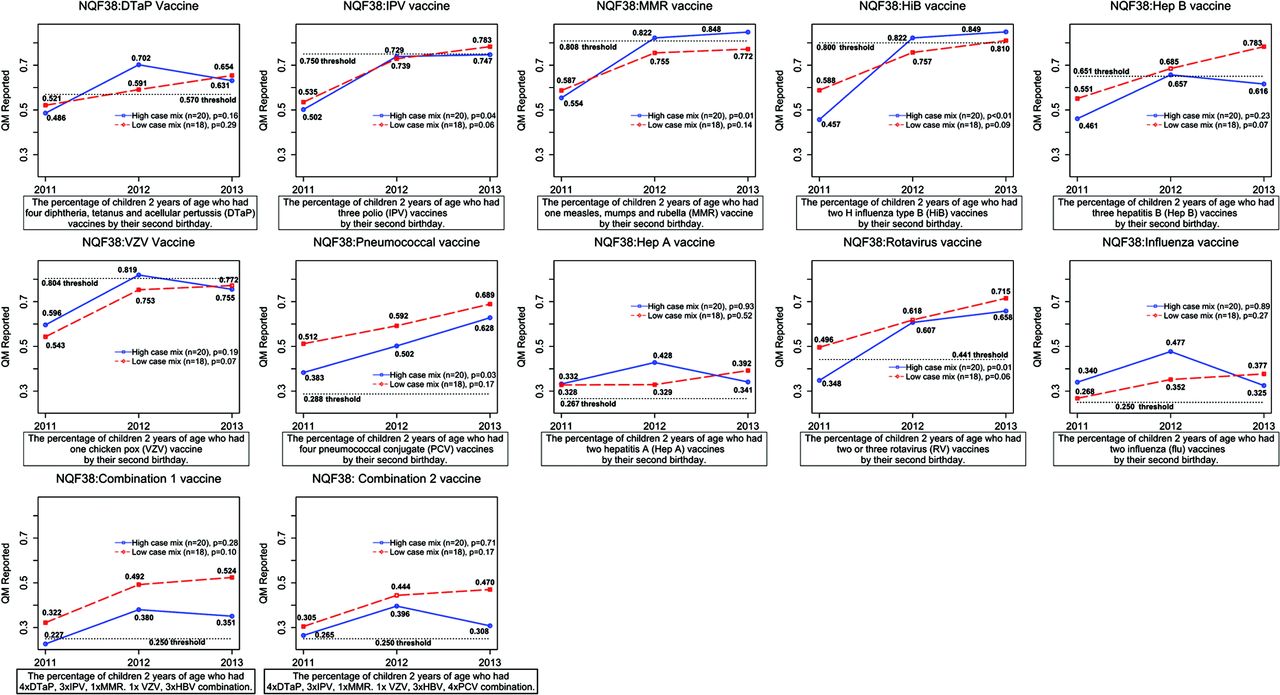
Preventive care domain (children's vaccinations): average National Quality Forum (NQF) quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.
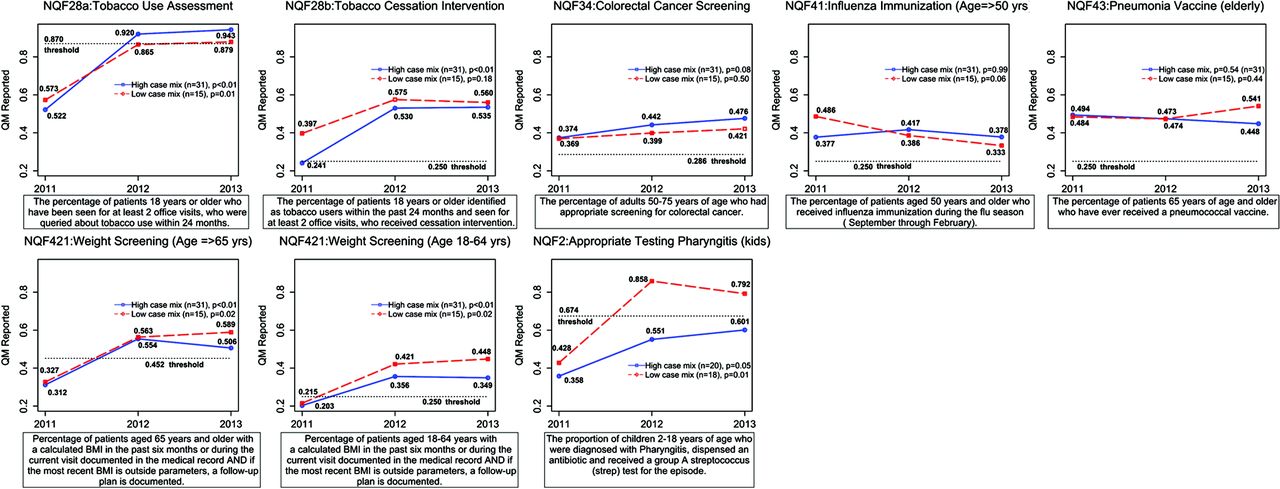
Of the remaining 8 quality metrics from the preventive care domain most relevant to adults (Appendix Figure 4), the following had an increase among practices with a high and low case mix: tobacco cessation intervention, colorectal cancer screening (high case-mix practices only), tobacco use assessment, weight screening for those ages 18 to 64 years, weight screening for those ≥65 years old, and appropriate testing for pharyngitis in children (all high and low case-mix practices). All metrics had surpassed or were within an acceptable range of the quality achievement range by 2013. Interestingly, we observed a significant trend for lower reported rates of influenza immunization among practices with a low case mix.
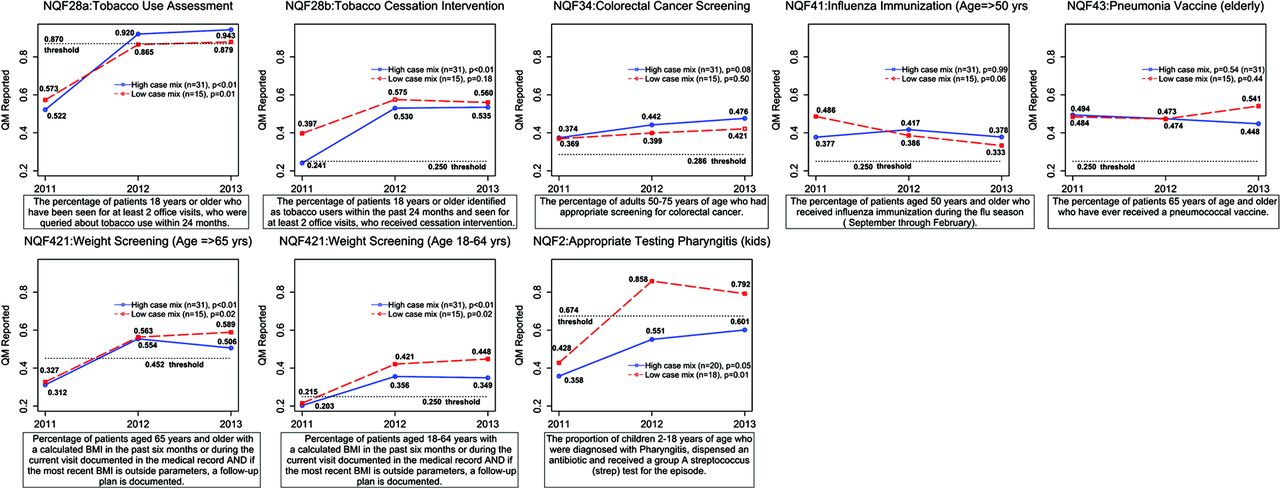
Preventive care domain (remaining metrics): average National Quality Forum (NQF) quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.
The mental health care domain (Appendix Figure 5) had the largest significant increase over the measurement period; both practices with a high case mix and those with a low case mix starting in the baseline year well below the achievement threshold for antidepressant treatment rates at 84 and 180 days after the diagnosis of major depression surpassed the threshold criterion by 2013.

Health care domain: average quality metrics (QM) scores reported over the years 2011 to 2013, stratified by practices with high and low case mixes. P values designate statistical significance of the average total change from 2011 to 2013.
Notes
This article was externally peer reviewed.
Funding: This publication was supported by Cooperative Agreement no. 3U58DP004812-02S1 from the Centers for Disease Control and Prevention through the Maryland Department of Health and Mental Hygiene's Center for Chronic Disease Prevention and Control. (See Acknowledgment.)
Conflict of interest: none declared.
Disclaimer: The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Maryland Department of Health and Mental Hygiene.
- Received for publication February 15, 2015.
- Revision received September 11, 2015.
- Accepted for publication September 21, 2015.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}