
Abstract
Background: The evidence of the relationship between fiber intake and control of diabetes is mixed. The purpose of this study was to determine if an increase in dietary fiber affects glycosylated hemoglobin (HbA1c) and fasting blood glucose in patients with type 2 diabetes mellitus.
Methods: Randomized studies published from January 1, 1980, to December 31, 2010, that involved an increase in dietary fiber intake as an intervention, evaluated HbA1c and/or fasting blood glucose as an outcome, and used human participants with known type 2 diabetes mellitus were selected for review.
Results: Fifteen studies met inclusion and exclusion criteria. The overall mean difference of fiber versus placebo was a reduction of fasting blood glucose of 0.85 mmol/L (95% CI, 0.46–1.25). Dietary fiber as an intervention also had an effect on HbA1c over placebo, with an overall mean difference of a decrease in HbA1c of 0.26% (95% CI, 0.02–0.51).
Conclusion: Overall, an intervention involving fiber supplementation for type 2 diabetes mellitus can reduce fasting blood glucose and HbA1c. This suggests that increasing dietary fiber in the diet of patients with type 2 diabetes is beneficial and should be encouraged as a disease management strategy.
Diabetes mellitus is an ever increasing problem in the United States. As of 2010, the Centers for Disease Control and Prevention estimates that there are 18.8 million people affected with this disease in the United States with another 7 million people with undiagnosed diabetes.1 Furthermore, almost 2 million people older than the age of 20 were newly diagnosed with diabetes in 2010.1 Diabetes was estimated to cost more than $174 billion in 2007 in the United States when taking into account medical costs and loss of productivity.2 Diabetes increases mortality by almost 2-fold and increases mortality by cardiovascular disease by 2- to 3-fold.3
Lifestyle modification is an important part of the management of diabetes. One of the main strategies for this is known as “medical nutrition therapy.” The goals of medical nutrition therapy include improving control of blood glucose levels, lipid profiles, and blood pressure to reduce the risk of cardiovascular disease in patients with type 2 diabetes mellitus.4 Medical nutrition therapy has been shown to reduce glycosylated hemoglobin (HbA1c) by 1% to 2% in patients with type 2 diabetes mellitus.5 It also has been shown to cause improvements in low-density lipoprotein cholesterol, an important marker in controlling the risk of cardiovascular disease.6 The American Diabetes Association recommends a specific diet as part of medical nutrition therapy for secondary and tertiary prevention in patients with type 2 diabetes mellitus. This diet includes the consumption of fiber-rich foods.4
Fiber has been studied in the treatment of diabetes for many years because increased fiber content decreases the glycemic index of foods.7–9 The theory, then, is that the decreased glycemic index would lead to smaller increases in blood glucose, and thus reduced blood glucose and HbA1c levels. Although high fiber intake has been linked to a decreased risk of diabetes,10,11 the evidence on fiber intake and control of diabetes is mixed. Specifically, many of the studies focused on fiber intake and glycemic control are small and have conflicting results; some studies show an improvement in diabetes control and others show no improvement.12–17 Therefore, the purpose of this study was to perform a meta-analysis of these studies to determine to what extent an increase in dietary fiber affects HbA1c and fasting blood glucose in patients with type 2 diabetes mellitus.
Methods
Data Sources and Searches
A search of PubMed materials dated January 1, 1980, to December 31, 2010, was performed on February 9, 2011, using the keywords “dietary fiber” and “diabetes mellitus.” A search of OVID, the Cochrane Clinical Register of Controlled Trials, and Cumulative Index to Nursing and Allied Health Literature also was performed using the same keywords. The references within studies that met inclusion criteria were searched for any possible relevant articles that may have been missed by these queries.
Study Selection
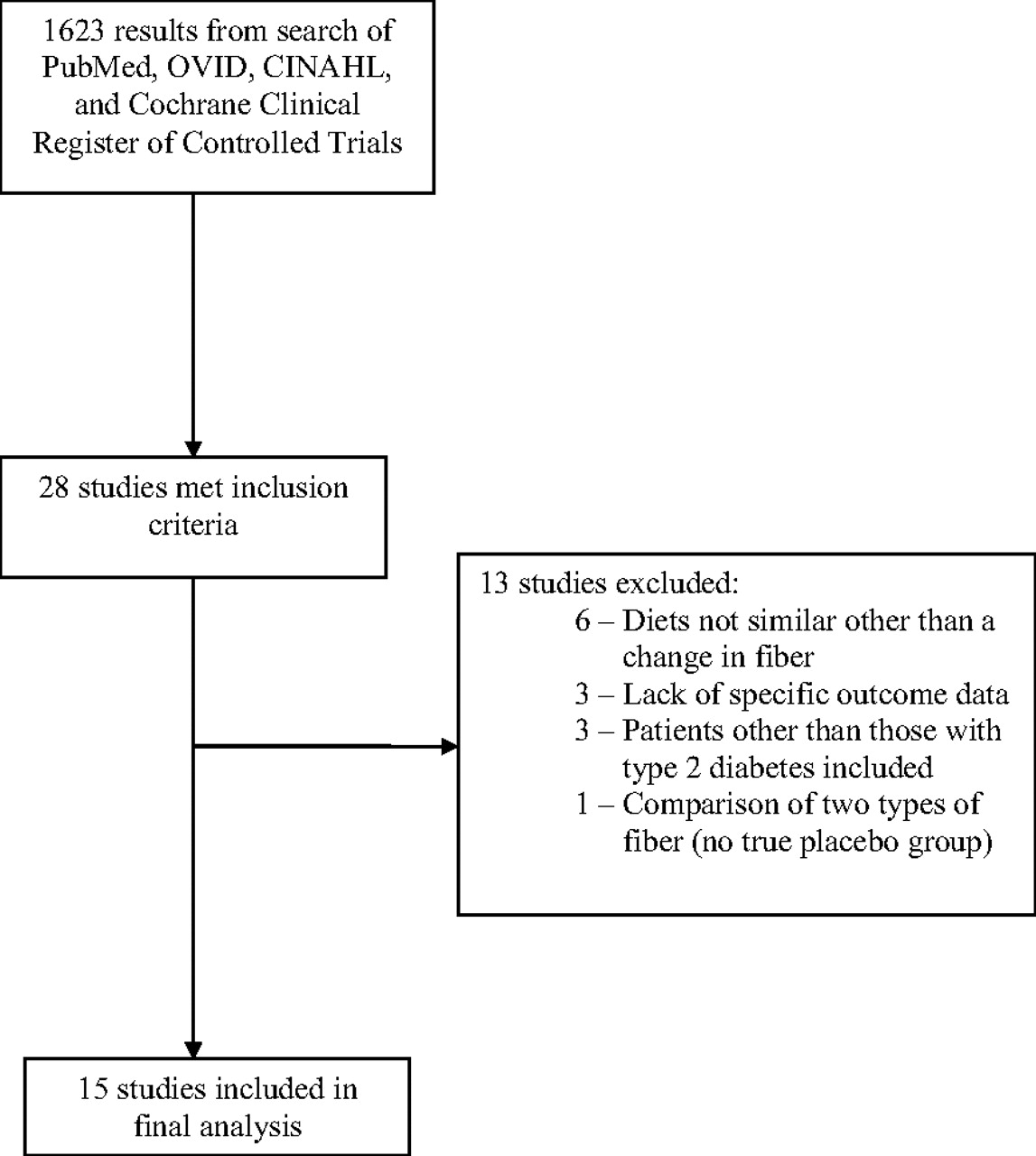
Inclusion criteria for this meta-analysis included randomized trials that involved an increase in dietary fiber intake as an intervention, evaluated HbA1c and/or fasting blood glucose as an outcome, used human participants with known type 2 diabetes mellitus, and was written in English. Exclusion criteria included are detailed in Figure 1.

Flow diagram for selection of studies for meta-analysis.
If a study included multiple arms, where one arm included diet and a medication versus another arm of just dietary intervention, then only the dietary intervention arm was included in the analysis. Patients in crossover trials, in which patients are their own controls, were treated as separate control and intervention arms for analysis.
Data Extraction
Data were extracted from each study and entered into an Excel spreadsheet (Microsoft, Corp., Redmond, WA). Demographic factors included sample population, mean age, mean body mass index, and sex distribution of the control and treatment groups. Outcome measures included final means for HbA1c and fasting blood glucose of the control and intervention groups. For studies that reported standard deviation of the mean, those data were used. For studies that reported standard error of the mean, standard error was multiplied by the square root of the sample population to obtain the appropriate standard deviations. If studies reported fasting blood glucose in units of mg/dL, this was converted to the standardized international unit of mmol/L by multiplying the fasting blood glucose value in mg/dL by 0.0555.
Study quality was assessed using the GRADE assessment as detailed in the Cochrane Handbook.18 This assessment takes into account the bias of studies as well as their methodology (eg, randomized vs observational) and their limitations to determine a quality grade of high, moderate, low, or very low.
Data Synthesis and Analysis
Meta-analysis for the mean differences was performed with Review Manager (version 5.0.23, The Nordic Cochrane Center, Copenhagen, Denmark). Separate analyses were performed for fasting blood glucose and HbA1c. Because measures of fasting blood glucose are on the same scale (mmol/L), and measures of HbA1c are on the same scale (percent of glycohemoglobin), a standardized mean difference was not necessary. The final means in the control and intervention groups were compared by computing a mean difference using the inverse variance method, where studies with less variance in their effect estimate are given more weight. Both fixed- and random-effects models were used for analysis. Comparison of final means is considered an appropriate analysis method in randomized trials because, in theory, the baseline data of the control and intervention groups in a randomized trial are not statistically different, and therefore final values for each trial arm would be representative of a change from a common baseline.18 A test of heterogeneity was performed to determine if results from a fixed-effect model could be considered valid. If the test of heterogeneity exhibited P < .05, then only the results of a random effect model would be considered valid. Forest plots each for fasting blood glucose and HbA1c were created. Funnel plots for each analysis to assess publication bias visually were created as well.
Results
Studies
The search initially yielded 1623 studies. Of these, 28 met inclusion criteria. Of these 28 studies, 13 were excluded for meeting one of the exclusion criteria, resulting in a total of 15 studies (Figure 1). Of the 15 included studies, 5 were randomized controlled trials19–23 and 10 were randomized crossover trials.24–33 Among these 15 articles, 13 contained data for fasting blood glucose that could be extracted and 10 contained data for HbA1c that could be extracted. Further details regarding the types of fiber and the specific interventions used in each study are listed in Table 1. Using the GRADE assessment, 11 of the studies were of high quality and 4 were of moderate quality.
Intervention Details of Included Studies
Demographics
Table 2 lists the demographic features of each study. The total number of participants for fasting blood glucose was 400 and for HbA1c was 324. Mean ages ranged from 52.1 to 69.1 years. The proportion of female participants ranged from 7.7% to 73.4%. Mean body mass index ranged from 23.4 to 32.5. Fiber interventions ranged from 4 to 40 g/d of additional fiber, with a mean increase in fiber for the intervention of 18.3 g/d. No studies reported any bias.
Demographics of included studies
Fasting Blood Glucose
Results for the meta-analysis of fasting blood glucose are shown in Figure 2. Because the test for heterogeneity was not statistically significant (P = .40), the fixed-effects model was considered valid for the analysis. Overall, fiber intervention was more effective than placebo in reducing fasting blood glucose. The overall mean difference was a reduction of fasting blood glucose by fiber of 0.85 mmol/L (95% CI, 0.46–1.25) more than the reduction from placebo. This is equivalent to a reduction over placebo of 15.32 mg/dL (95% CI, 8.29–22.52). The funnel plot for fasting blood glucose data are fairly symmetrical, with 7 studies favoring fiber and 6 favoring control, indicating low risk of publication bias for this data.
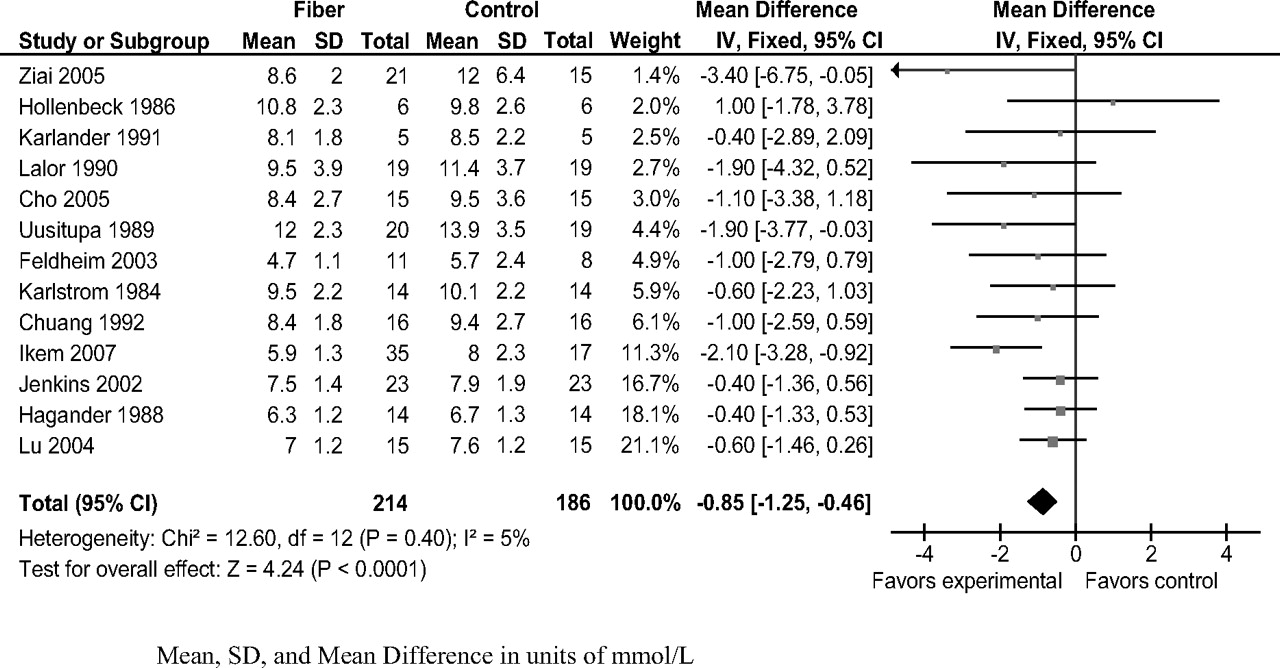
Forest plot for fasting blood glucose. Mean, SD, and mean difference are shown in units of mmol/L.
Glycosylated Hemoglobin
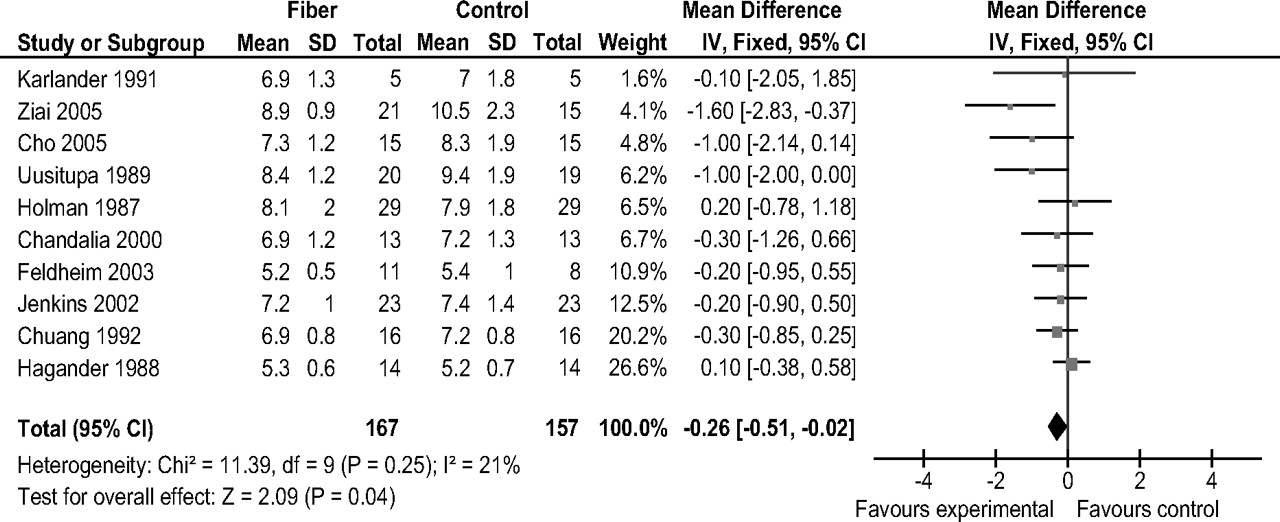
Results for the meta-analysis of HbA1c are shown in Figure 3. Because the test for heterogeneity was not statistically significant (P = .25), a fixed-effects model was considered valid for analysis. Overall, fiber intervention was more effective on HbA1c than placebo, with an overall reduction in HbA1c by fiber of 0.26% (95% CI, 0.02–0.51) more than the reduction from placebo. The funnel plot for HbA1c data is asymmetrical, indicating that there may be a risk of publication bias for this data.

Forest plot for glycosylated hemoglobin.
Discussion
The results of the meta-analysis show a statistically significant improvement in fasting blood glucose and HbA1c when an increase in dietary fiber was used as an intervention in patients with type 2 diabetes mellitus. However, the effect for HbA1c was more modest than that for fasting blood glucose. A possible cause for this is that the time period for 8 of the 10 interventions for HbA1c was less than 12 weeks, and HbA1c is representative of an overall glycemic control for a 12-week period. Therefore, most of the studies evaluating HbA1c were of a length less than the recommended testing period between HbA1c measurements. More studies evaluating HbA1c for a duration of longer than 12 weeks would be warranted.
Some may suggest that the effect on HbA1c, though statistically significant, my not be clinically significant. Metformin, one of the oral medications most commonly used to treat diabetes, has shown HbA1c reductions anywhere from the range of 0.2% to 2%.34 Comparatively, making a change in diet to reduce HbA1c by about 0.3% could be useful as an adjunctive therapy to medication as part of an overall treatment strategy for controlling diabetes. Again, this effect may be tempered by short follow-up durations of the majority of these studies, so fiber may truly have a larger affect on HbA1c than what is reported in this study.
These results suggest that increasing dietary fiber in the diet of patients with type 2 diabetes is beneficial and should be encouraged as a disease management strategy. High-fiber versions of traditionally low-fiber foods have been shown to be palatable for patients with type 2 diabetes.35 Consequently, this disease management strategy should not be particularly onerous for patients and may be easier to comply with than some other more intense lifestyle changes. The mean increase in fiber in the included studies was approximately 18 g/d. To implement this in one's diet would include eating a bowl of high-fiber cereal and adding a few more servings of vegetables a day.
The studies in this analysis used a variety of grams of fiber per day in their interventions, comprising a large range, from as little as an additional 4 g/d to as much as 40 g/d. The most commonly used fiber intervention dose was a 15-g/d supplement to usual diet. However, the American Diabetes Association recommends fiber consumption of at least 14 g/1,000 kcal/d or a range of 25 to 30 g/d, the values recommended by the United States Department of Agriculture,4 whereas the American Dietetic Association's position statement recommends 30 to 50 g of dietary fiber per day for patients with type 2 diabetes mellitus.36 Dietary fiber intake from a variety of sources has been associated with a significantly decreased risk of coronary events in epidemiologic studies in patients with and without diabetes. For example, in the Nurses Health Study, women with the highest fiber intake (median, 22.9 g/d) had an age-adjusted relative risk for major coronary events that was almost 50% lower than women in the group with the lowest fiber intake (11.5 g/d).37 Another study showed that fiber intake more than 20 g/d is associated with lower risk of coronary heart disease among women.38 Large epidemiologic studies have demonstrated an inverse relationship between fiber intake and cardiovascular disease rates in men as well.39,40 More studies of those specifically with type 2 diabetes mellitus with larger fiber doses as an intervention would aid in supporting or refuting recommendations for diabetics.
Limitations
The authors did not examine unpublished data, studies not in English, or any studies that were not published in peer-reviewed journals. One can argue that there is publication bias and that many negative studies are not published; however, many of the studies included in this analysis showed non-statistically significant effects. Also, the authors were trying to find studies of the highest quality, and these types of studies usually are published in English language, peer-reviewed journals. The studies exhibited a wide range of intervention amounts of fiber and lengths of time, but these differences are inherent in any meta-analysis.
Conclusions
Overall, an intervention involving fiber supplementation for type 2 diabetes mellitus can reduce fasting blood glucose and HbA1c. Further studies of more than 12 weeks' length are warranted for testing fiber's effect on HbA1c. Also, studies involving larger doses of fiber are warranted to help support current diabetes dietary fiber recommendations.
Notes
-
This article was externally peer reviewed.
-
Current affiliation: Virtua Family Medicine Residency, Voorhees, NJ (REP).
-
Funding: none.
-
Conflict of interest: none declared.
- Received for publication April 29, 2011.
- Accepted for publication August 9, 2011.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Bariatric surgery normalizes circulating glucocorticoid levels and lowers glucocorticoid action tissue-selectively in mice
- Vertical sleeve gastrectomy lowers kidney SGLT2 expression in the mouse
- Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report
- Plasma glucose and insulin responses after consumption of breakfasts with different sources of soluble fiber in type 2 diabetes patients: a randomized crossover clinical trial
- Addition of Orange Pomace to Orange Juice Attenuates the Increases in Peak Glucose and Insulin Concentrations after Sequential Meal Ingestion in Men with Elevated Cardiometabolic Risk
- High Fiber and Low Starch Intakes Are Associated with Circulating Intermediate Biomarkers of Type 2 Diabetes among Women
- Type and amount of dietary protein in the treatment of metabolic syndrome: a randomized controlled trial
- A High-Glycemic Index, Low-Fiber Breakfast Affects the Postprandial Plasma Glucose, Insulin, and Ghrelin Responses of Patients with Type 2 Diabetes in a Randomized Clinical Trial
- Nutrition Therapy Recommendations for the Management of Adults With Diabetes
- Nutrition Therapy Recommendations for the Management of Adults With Diabetes
- Content Usage and the Most Frequently Read Articles by Issue in 2012
- Answers to Common Clinical Questions