
Article Figures & Data
Figures
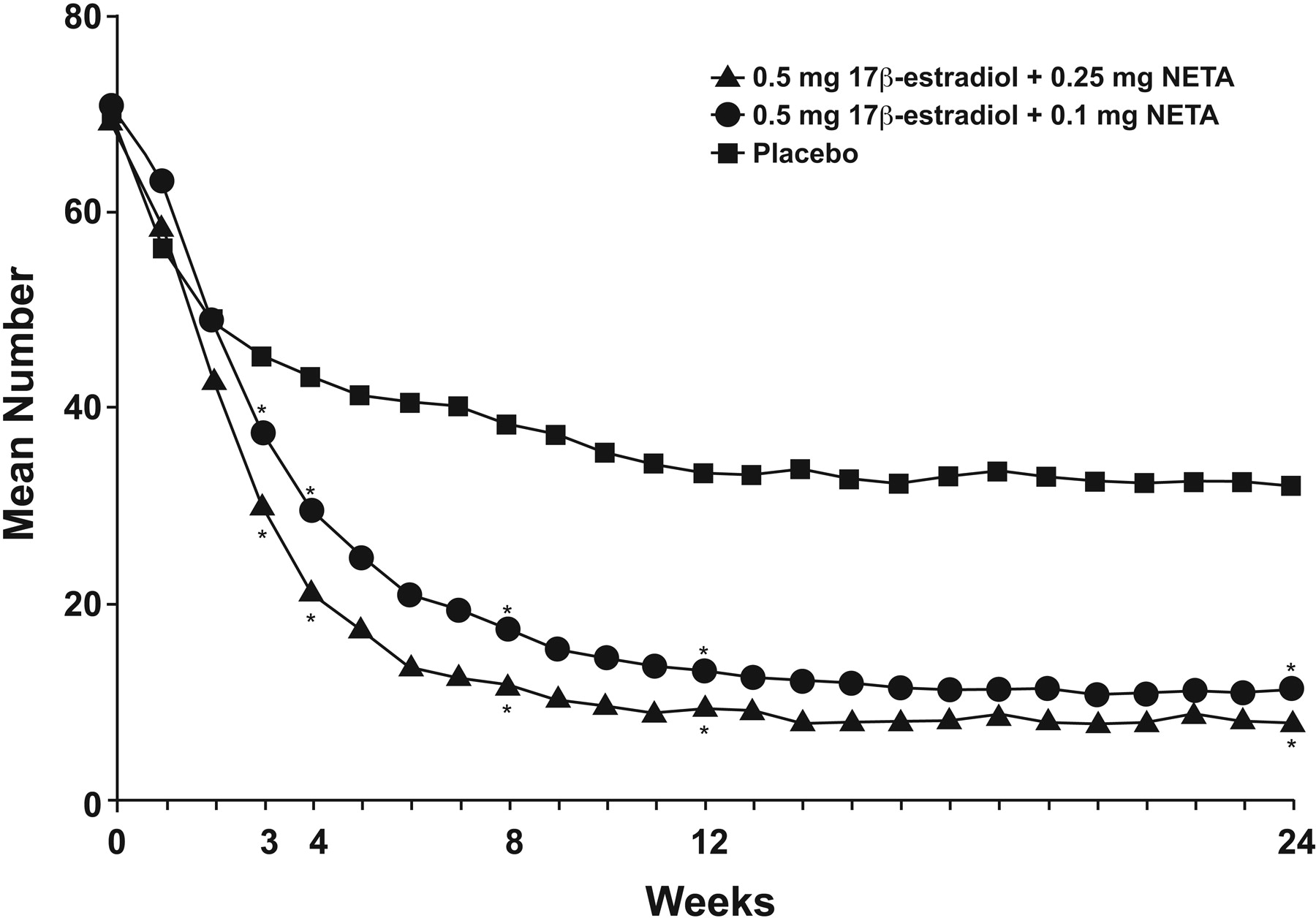
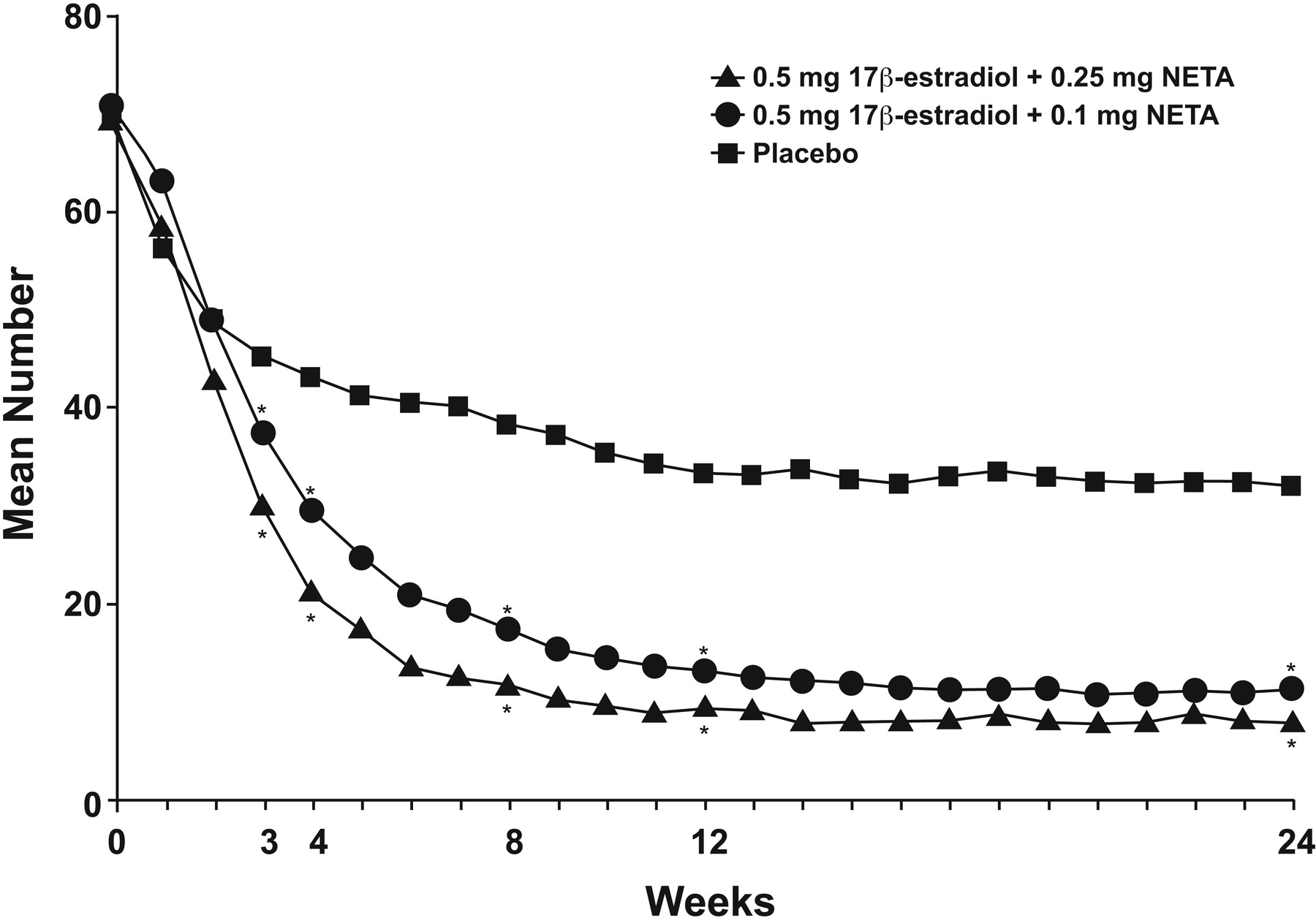
- Figure 1.
The number of moderate-to-severe hot flashes, by week, with low-dose E2 0.5/NETA 0.25 mg, E2 0.5/NETA 0.1 mg, and placebo. *Significantly different from placebo (P = .001). NETA, norethindrone acetate. (Reproduced with permission from Panay N, et al. Ultra-low-dose estradiol and norethisterone acetate: effective menopausal symptom relief. Climacteric 2007;10:120–31.28)
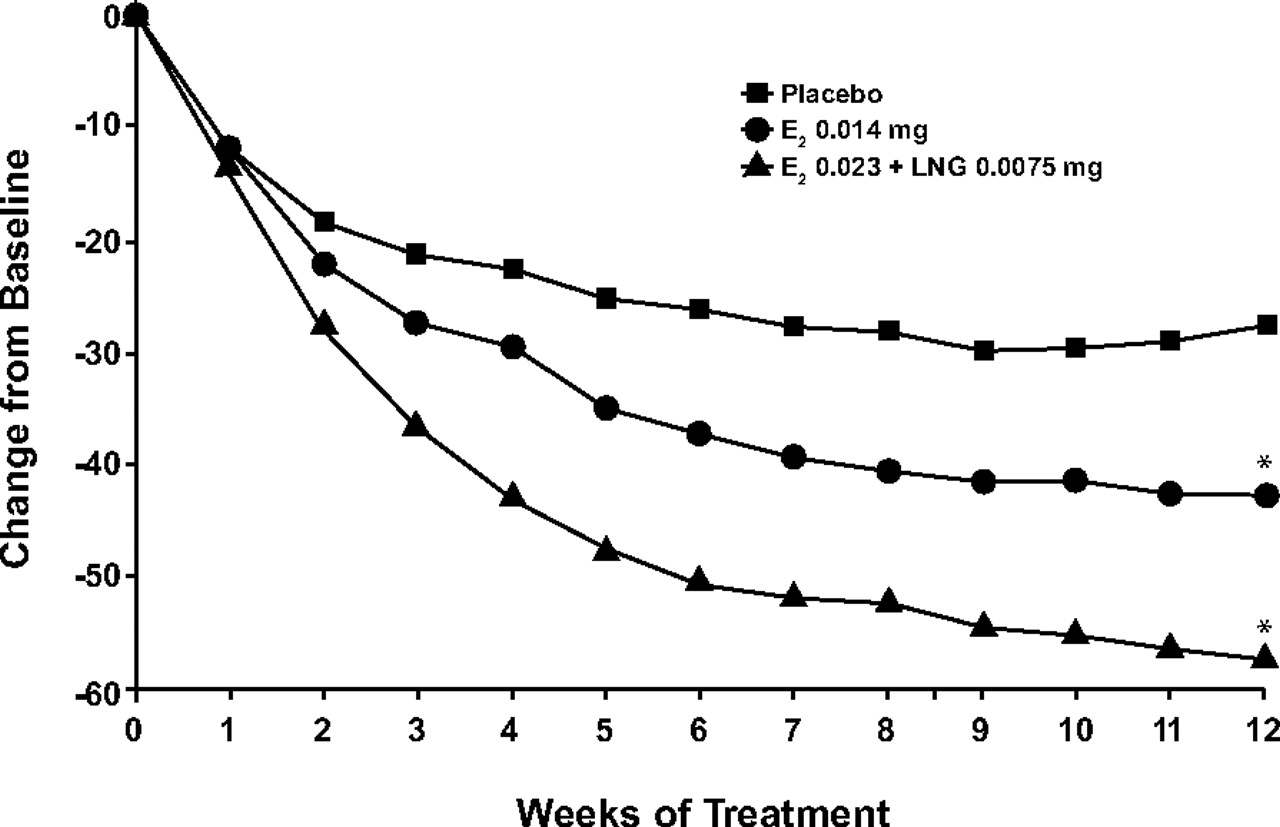
- Figure 2.
Change from baseline in the mean weekly frequency of moderate-to-severe hot flushes with transdermal E2 0.014 mg/d, transdermal E2 0.023 mg/d plus levonorgestrel (LNG) 0.0075 mg/d, and placebo. *P < .001 vs placebo. (Reproduced with permission from Bachmann G, et al. Lowest effective transdermal 17β-estradiol dose for relief of hot flushes in postmenopausal women: a randomized controlled trial. Obstet Gynecol 2007;110:771–9.22)
Tables
- Table 1.
Relative Risks of Clinical Events with Estrogen-Progestin Therapy Compared with Placebo in The Women's Health Initiative Randomized Trial2,4–10
Event (Reference) Overall Hazard Ratio Nominal 95% CI Adjusted 95% CI Coronary heart disease (4) 1.23 0.99 to 1.53 NR Stroke (4, 5) 1.31 1.03 to 1.68 0.93 to 1.84 Venous thromboembolism (6) 2.06 1.57 to 2.70 NR Breast cancer, invasive (7, 8) 1.24 1.01 to 1.54 0.94 to 1.33 Colorectal cancer (9) 0.56 0.38 to 0.81 0.33 to 0.94 Hip fracture (10) 0.67 0.47 to 0.96 0.41 to 1.10 Any fracture (10) 0.76 0.69 to 0.83 NR NR, not reported.
- Table 2.
Relative Risks of Clinical Events with Unopposed Estrogen Therapy Compared with Placebo Among Patients Without an Intact Uterus in The Women's Health Initiative Randomized Trial3,4,11–13
Event (Reference) Overall Hazard Ratio Nominal 95% CI Adjusted 95% CI Coronary heart disease (4) 0.95 0.78 to 1.16 NR Stroke (3, 4) 1.33 1.05 to 1.68 0.97 to 1.99 Venous thromboembolism (11) 1.32 0.99 to 1.75 NR Breast cancer, invasive (13) 0.80 0.62 to 1.04 NR Colorectal cancer (12) 1.12 0.77 to 1.63 NR Hip fracture (3) 0.61 0.41 to 0.91 0.33 to 1.11 Any fracture (3) 0.70 0.63 to 0.79 0.59 to 0.83 NR, not reported.
Dose (mg) Oral Formulations Conjugated equine estrogens 0.45 0.3 17β-estradiol (E2) 0.5 Ethinyl estradiol 0.025 Esterified estrogens 0.45 0.3 Transdermal Formulations E2 0.0375 0.025 0.014 - Table 4.
Placebo-Controlled Trials of Low-Dose Estrogen Preparations in Hot Flash Relief22–30
Author, Year (Reference) Patients Interventions Duration Outcomes Bachmann, 2007 (22) 425 menopausal women with ≥7 hot flashes per day or ≥50 hot flashes per week Transdermal E2 0.023/levonorgestrel (LNG) 0.0075 mg/d or transdermal E2 0.014 mg/d versus placebo 12 weeks Reduced 74%, P < .001 for E2/LNG; 55% P = .039 for E2 alone, 39% with placebo Diem, 2006 (23) 417 largely asymptomatic menopausal women aged 60 to 80 years Transdermal E2 0.014 mg/d versus placebo 2 years Only 16% reported hot flashes at baseline; no significant difference in hot flash improvement versus placebo Notelovitz, 2000 (29) 333 menopausal women with ≥56 hot flashes per week Oral E2 0.5 mg/d or 1 mg/d versus placebo 12 weeks Reduced, with E2 0.5 mg/d (P = .007) and 1 mg/d (P < .001) versus placebo; more patients on E2 1 mg/d responded Panay, 2007 (28) 575 menopausal women with ≥50 hot flashes per week Oral E2 0.5/NETA 0.1 mg/d, E2 0.5/NETA 0.25 mg/d, or placebo 24 weeks Reduced 81% with 0.5/0.1 mg/d; 86% with 0.5/0.25 mg/d; 52% with placebo (P ≤ .001 for both treatment groups); significant reduction at week 3 maintained through week 24 Rebar, 2000 (24) 204 menopausal women EE 0.3 mg/d versus placebo 12 weeks Reduced total symptoms score and Kupperman index versus placebo (P < .05) Speroff, 1996 (27) 324 menopausal women with 56 to 140 hot flashes per week Transdermal E2 0.02 mg/d or 0.04 mg/d versus placebo Two 12-week studies Reduced by 84%; with 0.02 mg/d at weeks 2 to 11 and with 0.04 mg/d at weeks 2 to 12 in Study 1. In Study 2, decrease was significant versus placebo with 0.02 mg/d at weeks 2 to 12 and with 0.04 mg/d at weeks 4 to 12 Speroff, 2000 (30) Study 1: 219 women with ≥10 hot flashes per week EE/NETA 0.01/0.2 mg/d, 0.025/0.5 mg/d, 0.05/1 mg/d, or 0.1/1 mg/d versus placebo Study 1: 16 weeks Reduced by week 4 in Study 1 and by week 5 in Study 2 (P < .05). Study 2: 266 women with ≥56 hot flashes per week Study 2: 12 weeks (did not include the 0.01/0.2-mg dose) Reductions were dose-related. Utian, 1999 (26) 196 menopausal women with ≥56 hot flashes per week Transdermal E2 0.025 mg/d, 0.05 mg/d, or 0.1 mg/d versus placebo 12 weeks Reduced at 12 weeks by 86% with E2 0.025 mg/d and 97% with both E2 0.05 mg/d and E2 0.1 mg/d versus 55% with placebo (P < .05 for all groups) Utian, 2001 (25) 241 menopausal women with ≥7 hot flashes per day or ≥50 hot flashes per week CEE 0.625 mg/d, 0.45 mg/d, 0.3 mg/d, CEE/MPA 0.625/2.5 mg/d, 0.45/2.5 mg/d, 0.45/1.5 mg/d, 0.3/1.5 mg/d, placebo 1 year Reduced with CEE 0.625/MPA 2.5 mg/d and all lower combination doses; CEE 0.625 mg/d reduced hot flashes more than CEE 0.45 mg/d or 0.3 mg/d alone (P < .05). Significant reductions versus placebo over 12 weeks starting at week 2 (0.625 mg/d, 0.45 mg/d, 0.625/2.5 mg/d, 0.45/2.5 mg/d) or week 3 (0.3 mg/d, 0.45/1.5 mg/d, or 0.3/1.5 mg/d) E2, 17β-estradiol; NETA, norethindrone acetate; EE, esterified estrogen; CEE, conjugated equine estrogen; MPA, medroxyprogesterone acetate; LNG, levonorgestrel.




{kind=link}
{kind=link}