
Article Figures & Data
Figures
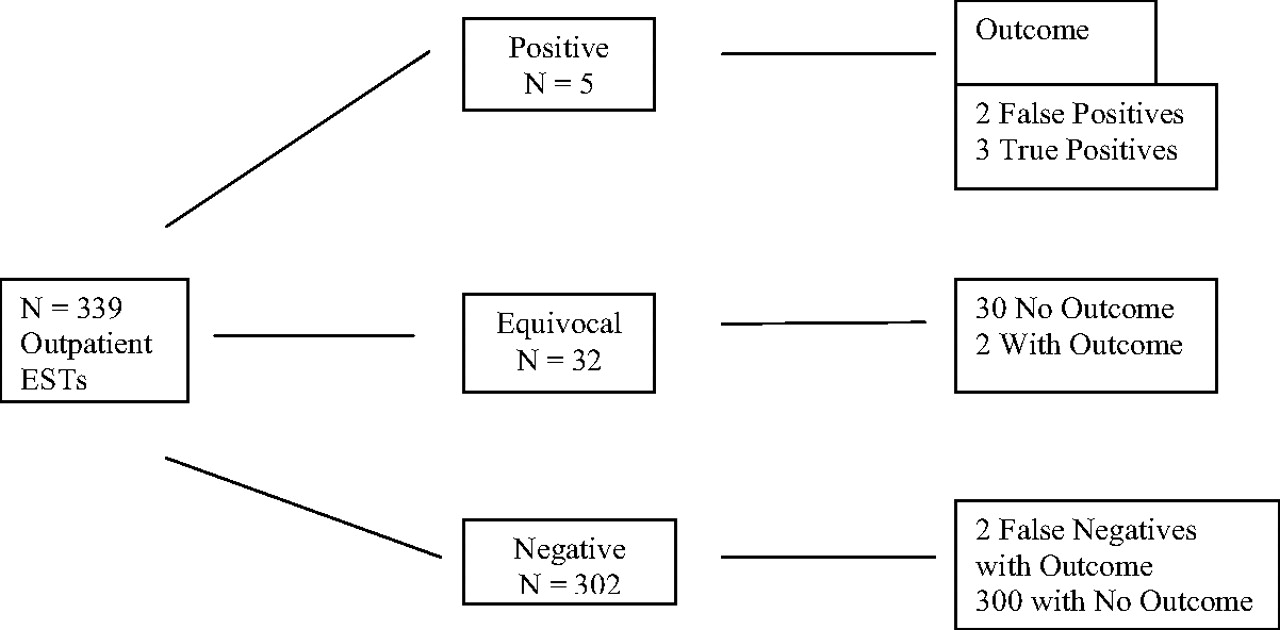
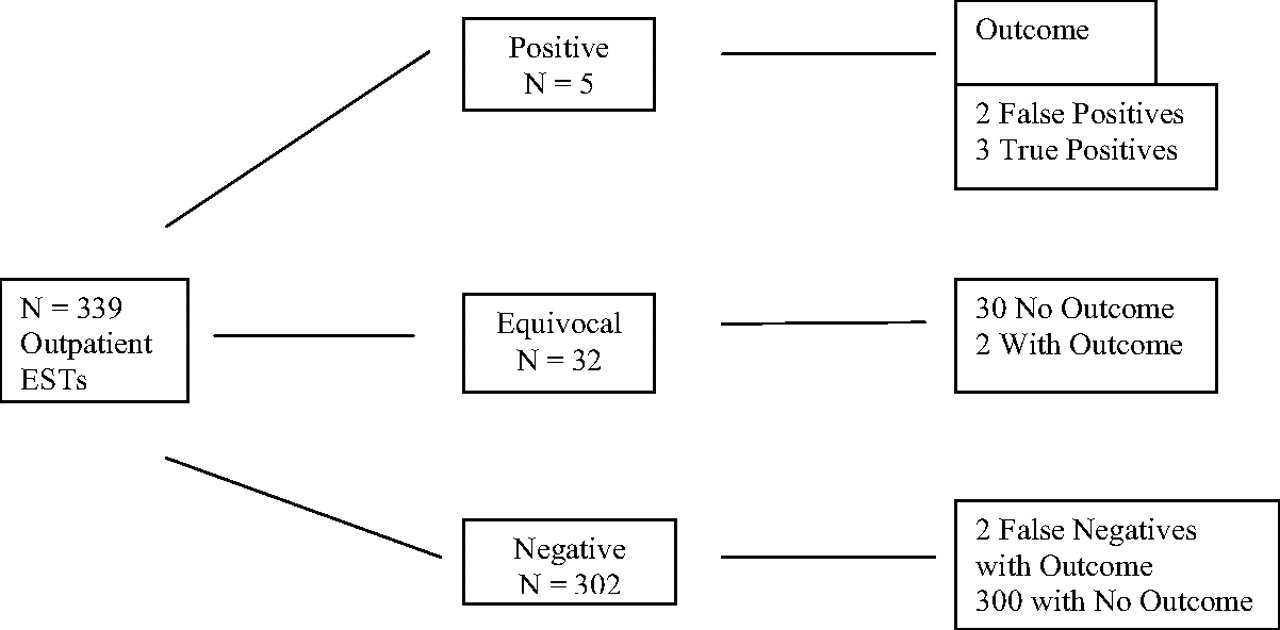
- Figure 1.
Summary of exercise stress testing results.
Tables
Age (years) Mean (range) 50.0 (24–91) SD ±10.66 Sex (%) Men 52 Women 48 Race (%) African-American 52 White 45 Other 3 Risk Factors (% [n]) Hypertension 59 (201) Hypercholesterolemia 29 (99) Diabetes Mellitus 23 (78) Smoker, previous or current 21 (70) Family history of CAD 8 (27) None reported 20 (69) CAD, coronary artery disease.
Cardiac Outcomes† Treadmill Result Yes No Total Value CI Positive‡ 5 32 37 Negative 2 300 302 Total 7 332 339 Sensitivity 0.7143 0.3589–0.9178 Specificity 0.9036 0.8671–0.9309 PPV 0.1351 0.0591–0.2797 NPV 0.9934 0.9762–0.9982 Positive likelihood ratio 7.4110 4.1800–13.1400 Negative likelihood ratio 0.3160 0.0980–1.0210 Probability of disease 0.0260 0.0100–0.0419 Overall accuracy 0.8997 0.8631–0.9286 * Calculations were based on formulas from http://faculty.vassar.edu/lowry/prop1.html. Formulas for confidence intervals from Newcome RG. Two sided confidence intervals for the single proportion; comparison of seven methods. Stat Med 1998;17:857–72.
† Cardiac outcomes included myocardial infarction, cardiac catheterization with angioplasty and stenting, coronary artery bypass graft, new diagnosis of coronary artery disease, and cardiac death.
‡ Equivocal results are included as positive tests.
Patient Number EST Result Cardiac Outcome Time to Outcome Descriptive Data Age (yr) Race/Sex Risk Factors 74 Positive Acute MI; catheterization; stenting 2 vessels 10 months 65 African-American male HTN, DM, hypercholesterolemia 128 Negative Acute MI; catheterization; stenting single vessel 2 months 51 African-American male HTN, smoker, hypercholesterolemia 157 Equivocal Catheterization; stenting 2 vessels; subsequent CABG 5 weeks 57 African-American male DM, HTN, Hypercholesterolemia 176 Positive Catheterization; stenting 2 vessels 2 months 42 White male FH, CAD, hypercholesterolemia 230 Negative Catheterization; 3-vessel CAD; CABG 29 months 49 White male HTN, negative EST (May 2004), positive stress echo (October 2006) 271 Equivocal Catheterization; stenting single vessel 5 weeks 44 White male Smoker, HTN 298 Positive Catheterization; 3-vessel CAD; CABG 1 week 54 White male HTN, DM, hypercholesterolemia EST, exercise stress test; MI, myocardial infarction; HTN, hypertension; DM, diabetes mellitus; CAD, coronary artery disease; CABG, coronary artery bypass graft.
ACC/AHA Class 1. Symptomatic patients—adults with chest pain with intermediate pretest probability of CAD (see Table 5)* I 2. Generating an exercise prescription 3. Determining functional capacity 4. Evaluating antianginal therapy† I 5. Evaluating patients after MI for risk stratification† I 6. Establishing severity and prognosis of CAD –Duke Score assessment† I 7. Evaluating dysrhythmias II 8. Asymptomatic patients (limited indications) A. Diabetics before starting moderate- to high-intensity exercise and age >35 years; type 2 DM for >10 years; type 1 DM for >15 years; presence of other cardiac risk factors, microvascular complications, or macrovascular complications IIA B. Men >45 years old, women >55 years old who plan to start a vigorous exercise program; high-risk public safety occupations; high risk for CAD with multiple other CAD risk factors IIB Modified from refs. 10 and 28.
* This is the most common indication.
† Some primary care physicians may choose to refer these patients with known CAD for exercise sestamibi study.
ACC/AHA, American College of Cardiology/American Heart Association ; CAD, coronary artery disease; MI, myocardial infarction; DM, diabetes mellitus.
Age (years) Gender Typical Angina Pectoris Atypical Chest Pain Nonanginal Chest Pain Asymptomatic 30–39 Men Intermediate Intermediate Low Very low Women Intermediate Very low Very low Very low 40–49 Men High Intermediate Intermediate Low Women Intermediate Low Very low Very low 50–59 Men High Intermediate Intermediate Low Women Intermediate Intermediate Low Very Low 60–69 Men High Intermediate Intermediate Low Women High Intermediate Intermediate Low Modified from refs. 10 and 28.
* High indicates >90%; intermediate, 10% to 90%; low, <10%; very low, <5%. Intermediate pretest probability is an ACC/AHA Class I indication for exercise stress testing.
- Table 6.
Suggested Exclusion Criteria for Exercise Stress Testing in a Primary Care Setting
1. Contraindications (see Table 7) 2. Patients who cannot walk ≥2 flights of stairs or 2 city blocks; refer for adenosine or dobutamine sestamibi study 3. Patients with resting EKG abnormalities: right or left bundle branch block, ST segment depression at rest; refer for ESS 4. Women with high pretest probability (see Table 4); refer for stress echocardiography 5. Men with high pretest probability (see Table 4); refer for ESS 6. Patients on digoxin; refer for ESS 7. Patients with Wolf-Parkinson-White Syndrome; refer for ESS 8. Patients with paced rhythm; refer for ESS 9. In general, patients with known CAD should undergo ESS, although valuable information can be gained from exercise stress test Modified from refs. 10 and 28.
EKG, electrocardiogram; ESS, exercise sestamibi study; CAD, coronary artery disease.
Absolute Acute myocardial infarction (within 2 days) High-risk unstable angina Uncontrolled cardiac arrhythmias Symptomatic severe aortic stenosis Uncontrolled symptomatic heart failure Acute pulmonary embolus or pulmonary infarction Acute myocarditis or pericarditis Acute aortic dissection Relative Left main coronary stenosis Moderate stenotic valvular heart disease Electrolyte abnormalities Severe arterial hypertension (>200/110) Tachyarrhythmias or bradyarrhythmias Hypertrophic cardiomyopathy and other forms of outflow tract obstruction Mental or physical impairment leading to inability or willingness to exercise adequately High-degree atrioventricular block Modified from ref. 10.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Appropriately testing patients with intermediate risk for coronary artery disease: how well are we doing?
- Violence risk assessment as a medical intervention: ethical tensions
- Coronary Computed Tomography Angiography After Stress Testing
- Coronary Computed Tomography Angiography After Stress Testing: Results From a Multicenter, Statewide Registry, ACIC (Advanced Cardiovascular Imaging Consortium)
- Re: Predictive Value of Exercise Stress Testing in a Family Medicine Population
- Optimism: A Good Theme for Family Medicine
- Chronic Disease: Increasing Prevalence Yet Better Control