
Abstract
Purpose: Exercise stress testing (EST) is a screening test for coronary artery disease. Previous studies from the cardiology literature show an overall sensitivity of 67% and specificity of 72% with variable predictive values depending on pretest probability. The purpose of the current study was to evaluate the predictive value of EST in a family medicine population in eastern North Carolina.
Methods: This is a retrospective case series of 339 ESTs performed in a family medicine center from July 2001 to April 2005. EST results were classified as positive, negative, or equivocal. Outcomes studied from a review of outpatient and inpatient electronic medical record data and telephone follow-up included myocardial infarction, cardiac catheterization with angioplasty and stenting, coronary artery bypass grafting, a new diagnosis of coronary artery disease, and cardiac death. Mean duration of follow-up was 47 months, with a range of 27 to 72 months.
Results: Nearly all patients had low to intermediate risk pretest probability. Five tests were positive, 32 were equivocal, and 302 were negative. There were 2 false-positive tests, both in female patients. There were 2 false-negative tests, both of which were treated with good outcomes. Two of 32 equivocal results had cardiac outcomes. Considering equivocal tests as positive, the overall sensitivity in this series was 71.4%; specificity was 90.4%. The positive predictive value was 13.5% and the negative predictive value was 99.3%.
Conclusions: The high negative predictive value for EST in this outpatient family medicine population is noteworthy and reassuring. EST is a cost-effective strategy for triaging the common complaint of chest pain in low- to intermediate-risk patients in primary care practices and should be included in the services offered to family medicine patients.
Coronary artery disease (CAD) is the leading cause of death in the United States and accounted for 479,305 deaths in 2003 and nearly 1,200,000 myocardial infarctions per year.1 White men and African-Americans of both sexes have the highest incidence of CAD. Death rates have declined 26.5% from 1993 to 2003, primarily because of improved risk factor modification and better treatments.
Chest pain is the most common presenting complaint indicating CAD and is seen frequently by primary care physicians. Exercise stress testing (EST) is often used to decide which patients need further work-up and referral to a cardiologist. In 2005, only 12.8% of family physicians were doing EST in their offices, up from 7.9% in 1990.2,3 Family physicians in rural locations were more likely to offer this service than those in suburban locations.4
There is a surprising paucity of studies about the use of EST by family physicians for the diagnosis of CAD, with only 3 small case series noted from 1979 to 1985.5–7 Eberly5 in 1979 reported a series of 140 patients undergoing EST with high pretest probability. Thirty-seven percent had a positive EST and 14% had a false-negative test. This study was limited because outcomes were not prespecified.5 Zoller and Boyd6 reported on 275 cases in 1985; 22.5% had positive studies, 75.6% had negative studies, and 1.8% had equivocal results. Follow-up ranged from 1 month to 6 years. They reported a 9.3% false-positive rate and a 12.5% false-negative rate but did not report predictive values for the test. There were 2 complications involving persistent electrocardiographic (EKG) changes and hospitalization but both had good outcomes.6 Harmon7 reported his series of 309 stress tests from South Carolina in 1988. Follow-up was from 1 to 5 years. There was correlative cardiac catheterization data in 56 patients (18%), which was the only outcome studied. For patients with symptomatic chest pain there was a 26% false-positive rate (38% for women) and a 2% false-negative rate.
Many studies, including those cited above, have documented the safety of ESTs performed in the office by family physicians. Mead8 reported a series from Seattle in 1979 of 2490 tests without morbidity or mortality. Ilia and Gueron9 reported a series in 1997 of 24,153 tests performed by family physicians from a community practice in Israel with very low morbidity and no mortality. There are countless studies available in the cardiology literature on EST and its use in evaluating CAD, with a mean sensitivity of 67% and a mean specificity of 72%.10
However, these cardiology studies have significant work-up and referral bias because they come from a specialty practice. Froelicher et al11,12 reported a series of 814 patients with chest pain from the Veteran's Administration System who underwent both EST and cardiac catheterization with limited work-up bias; they found a sensitivity of 45% and a specificity of 85% for EST. Morise and Diamond13 reported that the accuracy of EST for the diagnosis of CAD is lower in women than in men, and the difference is not explained by referral bias.
The predictive value of EST for diagnosing CAD depends heavily on pretest probability of CAD. One large study of 5103 patients reported positive predictive values (PPVs) of 21%, 62%, and 92% in low, intermediate, and high pretest probability groups, respectively. Negative predictive values (NPVs) were 94%, 72%, and 28% in the same low, intermediate, and high pretest probability groupings.14 Thus, NPV increases with lower pretest probability of disease whereas PPV decreases. This situation would be typical of a primary care population presenting for exercise testing without the referral bias seen in cardiology studies of EST. Another series of 1010 patients presenting to an emergency department, reported by Gibler,15 found EST in the chest pain unit to have a PPV of 44.4% and an NPV of 98.7%.
The purpose of this study was to evaluate the predictive value of EST in a family medicine outpatient population in eastern North Carolina. There are no studies that report this in the family medicine literature and studies from cardiology are limited by referral and work-up bias, as noted above. In addition, our study evaluated well-defined, prespecified, patient-oriented outcomes, which was not consistently done in previous family medicine case series.
Methods
This is a retrospective case series of 339 patients in whom outpatient EST was performed in the Family Medicine Center at Brody School of Medicine at East Carolina University from July 2001 to April 2005. The cases were selected by searching billing records for CPT code 93015 and represented all patients who had an outpatient EST during this interval. The only exclusion criteria was known preexisting CAD (5 patients).
Three board-certified physician faculty who were trained during residency to do EST performed the tests. A Quinton model Q 55 treadmill (Cardiac Science Corp., Bothell, WA) was used with either the standard Bruce or modified Bruce protocol, the selection dependent on predicted exercise capacity. Patients were asked to exercise to their maximum capacity with the goal of reaching 85% of their maximum predicted heart rate. The study received approval from the Brody School of Medicine Institutional Review Board. All data sheets were kept without names or other identification to protect patient confidentiality. Medical records of these patients were reviewed and abstracted by a trained data specialist. Data collected on each patient included age; sex; ethnicity; indication for the test; risk factors for CAD; exercise time; percent of maximum predicted heart rate achieved; symptoms of angina (graded as 0 = none, 1 = mild, and 2 = exercise limiting); Duke treadmill score (DTMS); baseline blood pressure; and blood pressure at peak exercise. The result of the test was recorded as negative, equivocal, or positive. Positive tests were defined as showing ≥1 mm of flat or down-sloping ST depression in any of the standard EKG leads. Equivocal tests were defined as not meeting the positive test criteria but showing concerning change (eg, symptoms of chest pain without EKG change of ischemia or inadequate exercise time or inability to achieve target heart rate). ST depression was interpreted by the Quinton Q 4500 treadmill computer system (Cardiac Science Corp.) with confirmation by the supervising physician (RJN and MD). A DTMS16 was calculated in each case as follows: DTMS = time of exercise –4x (Angina Index graded as 0 to 2) –5x (mm of ST depression). The DTMS was then correlated with cardiac outcome. Any complications of the test were also recorded. All EST data were abstracted from a standard EST template routinely used in our electronic medical record system. Patients with equivocal or positive tests were referred to our cardiology group for exercise sestamibi study, adenosine sestamibi stress testing, or directly for cardiac catheterization.
Outcome data were obtained from careful review of the outpatient electronic medical record and the university hospital records on each patient. Two trained data specialists each independently reviewed these records for outcomes (EJ). Follow-up intervals ranged from a minimum of 27 months to a maximum of 72 months (mean duration, 47 months). Outcomes studied included documented myocardial infarction, cardiac catheterization with angioplasty and stenting, coronary artery bypass grafting (CABG), a new diagnosis of CAD, and cardiac death. The university hospital is the primary site of hospitalization for all family medicine patients and provides all levels of cardiac care. To ensure complete outcome data capture, a phone follow-up survey was conducted in July and August 2007 by a trained technician (EJ). We were able to obtain phone follow-up data for 71% of patients.
Descriptive statistics were used to characterize the study population with respect to demographics, cardiac risk factors, test indications, and EST results. We then evaluated the relationship between EST results and any chart-documented cardiovascular outcomes by calculating sensitivity, specificity, PPV, NPV, and positive and negative likelihood ratios using standard formulas from a 2 × 2 table.17 Confidence intervals were also calculated for each of these values. DTMS was correlated with cardiac outcome.
Results
Patient demographics of the 339 patients are presented in Table 1. Fifty-two percent were men and 48% were women. Forty-five percent of patients were white, 52% were African-American, and 3% were other races. The age range was from 24 to 91 years with a mean age of 50 years.
Characteristics of the Exercise Stress Testing Study Population
The most common indications for EST were chest pain (59%), preexercise evaluation (8%), shortness of breath (4%), multiple cardiac risk factors (3.8%), and screening (2.3%). No indications were listed in the EST template in 23% of patients. The study population had a significant number of cardiac risk factors, as noted in Table 1. There were no risk factors reported in 69 patients (20.1%).
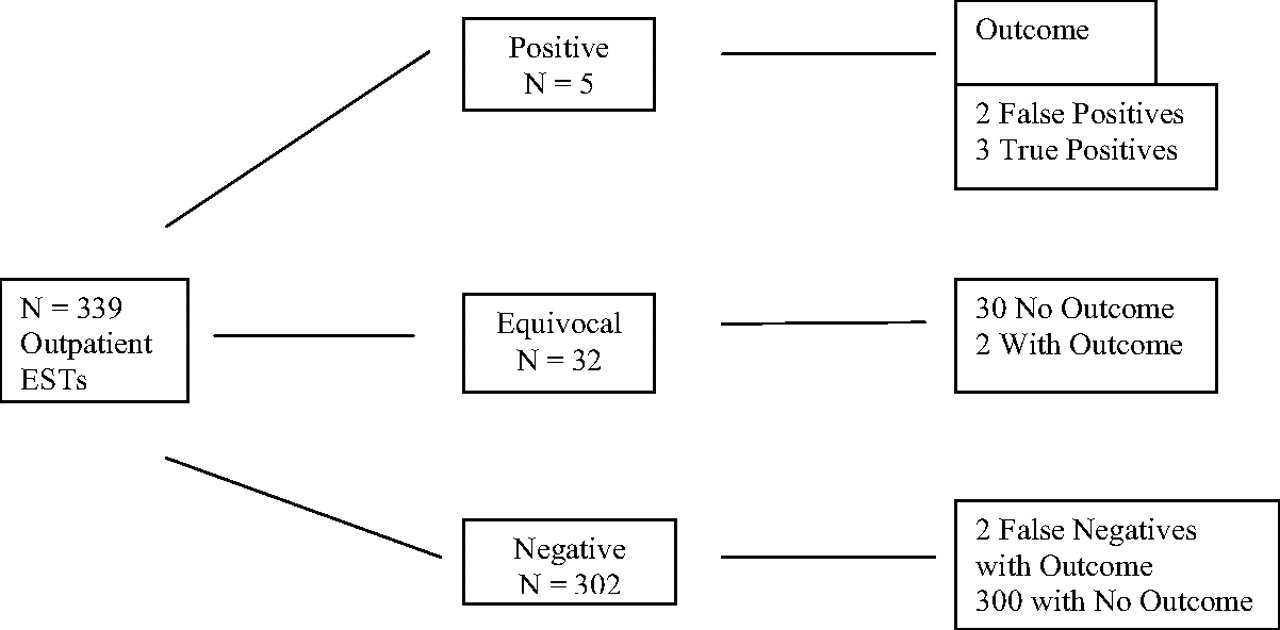
Table 2 shows a standard 2 × 2 analysis of EST for the cardiac outcomes studied. For the purposes of this analysis, equivocal results were counted as positive results. There were a total of 5 positive studies, 2 of which were false-positives as demonstrated by subsequent radionuclide stress testing or cardiac catheterization. Both of the false-positive studies were in female patients. There were 32 equivocal studies, 2 of which subsequently showed a cardiac outcome. Two studies were false-negative tests with a high DTMS. Figure 1 summarizes the outcomes sorted by EST result.
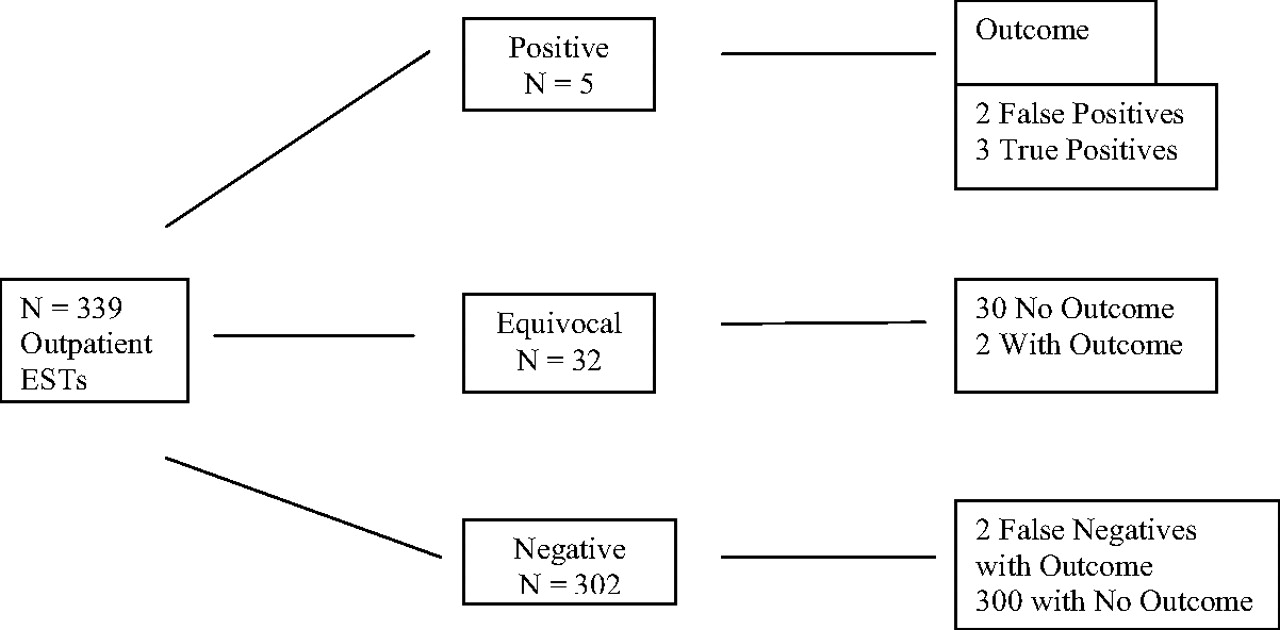
Summary of exercise stress testing results.
Exercise Stress Testing Outcomes*
A total of 7 patients, as summarized in Table 3 had outcomes of myocardial infarction, cardiac catheterization with angioplasty and stenting, CABG, or a new diagnosis of CAD. Three cases were true positives with a positive EST and an outcome event within 10 months of the test, all demonstrating CAD at the subsequent cardiac catheterization. One of these patients had a negative radionuclide stress test immediately after an EST performed in the office, but subsequently developed an acute myocardial infarction 10 months later. Catheterization showed 2-vessel CAD with stenting and a good outcome. Two patients with equivocal results had documented CAD at catheterization within 6 weeks of the EST. Of the 2 patients with false-negative results, one had a myocardial infarction within 2 months of the EST. Catheterization showed single-vessel disease, which was stented with excellent outcome. The other patient with a false-negative result had an initial negative test with DTMS of 13 in May 2004, then had a positive stress echo for new symptoms in October 2006. Catheterization in October 2006 showed multivessel disease and the patient underwent CABG with good outcome. All 7 cardiac outcomes were in male patients and occurred within 16 months of the EST. A total of 3 patients underwent CABG.
Patients with Positive Cardiac Outcomes
Six patients died over the follow-up period, none of cardiac causes. Causes of death included alcoholic cirrhosis, laryngeal cancer, gastric cancer, systemic sclerosis, Alzheimer's disease, and an adverse drug reaction to a psychotropic medication.
Applying standard formulas17 to the data in Table 2 yields a sensitivity of 71.4% and specificity of 90.4% from the ESTs performed in this outpatient family medicine population. The PPV was 13.5% for EST in our Family Medicine Center whereas NPV was 99.3%. For our study, the positive likelihood ratio was 7.4 and negative likelihood ratio was 0.32. Confidence intervals for these results are shown in Table 2.
DTMS was calculated for all ESTs performed in this series. The DTMS did correlate with the likelihood of having a cardiac outcome; thus, 3 of 56 patients (5.4%) with a DTMS ≤5 had a cardiac outcome. There were only 4 cardiac outcomes of 283 studies (1.4%) in which the DTMS was >5.
There were no serious complications in this study. Two patients had hypotension after EST and 64 had minor arrhythmias (premature atrial contractions, premature ventricular contractions, and 1 case of atrial fibrillation) with good outcomes. There were no myocardial infarctions or deaths resulting from EST and no significant morbidity resulted from the test.
Discussion
The high NPV of EST for subsequent patient-oriented cardiac outcomes in this outpatient family medicine population with low to intermediate pretest probability is very reassuring. The high NPV, relative to cardiology studies, probably reflects the lower pretest probability in a family medicine population compared with a cardiology clinic population with referral bias. This study's strength is that it is one of the few from family medicine outpatient populations, and the only one to study predictive values of EST for patient-oriented outcomes in this population of patients. Our study differs from other reported family medicine studies in that there were far fewer positive EST results. This result probably reflects our practice of admitting patients with high pretest probability when they presented with chest pain and studying these patients in the hospital. In addition, a decline in the incidence of CAD has occurred since these earlier studies. One limitation of our study is the variable follow-up times, which ranged from 27 to 72 months. It is also possible that some patients had a cardiac event in another location than those we sampled. However, our medical center is the only referral center for a large region and we verified our records review with telephone follow-up. Further research with data from multiple family medicine outpatient practices is needed to verify our findings.
A strong case can be made to include EST in the services offered to family medicine patients. There are many indications for EST in primary care practice, including evaluation of chest pain and dyspnea, following the course and severity of CAD, preexercise screening in patients with multiple cardiac risk factors, and determining functional capacity to write an exercise prescription.18,19
Table 4 is a suggested format for selecting patients for EST evaluation in a primary care setting. Table 5 shows the method of predicting pretest probability of CAD based on age, sex, and the description of chest pain. Guidelines from the American College of Cardiology and the American Heart Association recommend EST as a class I indication for the evaluation of the common clinical situation of adult patients with intermediate pretest probability of CAD.10 Table 6 lists suggested exclusion criteria for EST in a primary care setting and Table 710 lists contraindications to the procedure. Consideration should be given to doing stress echocardiogram in women with higher pretest probabilities because this test has fewer false positives in women.
Selection of Patients for Exercise Stress Testing in a Primary Care Setting
Pretest Probability of Coronary Artery Disease by Age, Gender, and Symptoms*
Suggested Exclusion Criteria for Exercise Stress Testing in a Primary Care Setting
Contraindications to Exercise Stress Testing
Standard techniques for performing EST have been well described, and these should be followed rigorously to ensure safety and standardization of the procedure.20 Appropriate training through residencies or courses such as those offered annually by the American Academy of Family Physicians should be undertaken with a period of proctoring or mentoring by a clinician experienced in performing ESTs.
The EST result can be classified as either positive, negative, equivocal, or indeterminate.21 As in this series, the majority of patients with a negative EST and good exercise time can be reassured, but should be instructed to report persistent symptoms and to continue risk factor modifications. One population-based study from Minnesota showed that longer exercise capacity on the treadmill was protective of cardiac events and mortality.22 Conversely, a recent study of 9191 patients referred for an EST showed that reduced exercise capacity was associated with increased risk for cardiovascular events.23 Patients with positive, equivocal, or indeterminate results should be referred for additional study. Patients with high pretest probability and a positive EST can be referred directly for cardiac catheterization. The DTMS can be used for risk stratification and to determine the urgency of cardiology referral, with those having a low score (≤5) being referred for prompt evaluation.24
Cardiologists have moved away from using a standard EST to evaluate patients as more sophisticated and expensive tests with higher reimbursement have become available.25 The continued use of standard EST by primary care physicians to triage chest pain patients as described above has the potential to create tremendous health care cost savings. Specifically, at our institution the billing for a standard EST is $483 compared with an exercise sestamibi study, which is billed at $3283. This 7-fold increase in cost is hardly justified in the case of a low-risk patient with atypical chest pain who can be reassured safely with a negative EST. The following quote from Victor Froelicher, a cardiologist and noted authority on EST summarizes this nicely: “As George Bernard Shaw said 80 years ago, ‘the doctor does the test he is paid (the most) for.’ By attempting to decrease medical expenditures by targeting high frequency procedures, the EKG and standard exercise test have been devalued. Unfortunately, that drives practice to the more expensive modalities that increase in volume and cause even greater increases in health care costs.”25
The above gives a strong case for including EST in the services offered by primary care physicians and has important implications for residency training. Estimates range from 31% to 50% of family medicine residencies are currently offering EST training.26,27 Only 12.8% of family physicians offer this procedure in their offices, and lack of training and the cost of the equipment were cited as the major barriers to performing ESTs.2 Residency programs in both family medicine and internal medicine should be encouraged to offer a competency-based curriculum for ESTs. By increasing the number of primary care physicians offering this procedure, maintaining quality of care with tremendous health care cost savings can be realized.
Conclusion
We have shown that EST can be safely and successfully performed in an outpatient family medicine setting in patients with low to intermediate pretest probability of disease. This study demonstrates high NPVs that are reassuring to both patients and providers and suggests that EST can be a cost-saving procedure in primary care.
Acknowledgments
We would like to acknowledge the University of North Carolina Department of Family Medicine Faculty Development Fellowship Faculty; Trena Carmon, BS; and Brian Burkhart, MPH.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication November 20, 2007.
- Revision received March 3, 2008.
- Accepted for publication March 10, 2008.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Appropriately testing patients with intermediate risk for coronary artery disease: how well are we doing?
- Violence risk assessment as a medical intervention: ethical tensions
- Coronary Computed Tomography Angiography After Stress Testing
- Coronary Computed Tomography Angiography After Stress Testing: Results From a Multicenter, Statewide Registry, ACIC (Advanced Cardiovascular Imaging Consortium)
- Re: Predictive Value of Exercise Stress Testing in a Family Medicine Population
- Optimism: A Good Theme for Family Medicine
- Chronic Disease: Increasing Prevalence Yet Better Control