
Abstract
Objective: To conduct a systematic review of published literature regarding the effects of yoga, a promising mind-body therapy, on specific anthropometric and physiologic indices of cardiovascular disease (CVD) risk and on related clinical endpoints.
Methods: We performed a literature search using 4 computerized English and Indian scientific databases. The search was restricted to original studies (1970 to 2004) evaluating the effects of yoga on CVD or indices of CVD risk associated with the insulin resistance syndrome (IRS). Randomized controlled trials (RCTs), nonrandomized controlled trials, uncontrolled (pre and post) clinical trials, and cross-sectional (observational) studies were included if they met specific criteria. Data were extracted regarding study design, setting, population size and characteristics, intervention type and duration, comparison group or condition, outcome assessment, data analysis and presentation, follow-up, and key results, and the quality of each study was evaluated according to specific predetermined criteria.
Results: We identified 70 eligible studies, including 1 observational study, 26 uncontrolled clinical trials, 21 nonrandomized controlled clinical trials, and 22 RCTs. Together, the reported results of these studies indicate beneficial changes overall in several IRS-related indices of CVD risk, including glucose tolerance and insulin sensitivity, lipid profiles, anthropometric characteristics, blood pressure, oxidative stress, coagulation profiles, sympathetic activation, and cardiovagal function, as well as improvement in several clinical endpoints.
Conclusions: Collectively, these studies suggest that yoga may reduce many IRS-related risk factors for CVD, may improve clinical outcomes, and may aid in the management of CVD and other IRS-related conditions. However, the methodologic and other limitations characterizing most of these studies preclude drawing firm conclusions. Additional high quality RCTs are needed to confirm and further elucidate the effects of standardized yoga programs on specific indices of CVD risk and related clinical endpoints.
Cardiovascular disease (CVD) is the leading cause of death and disability in the United States and other industrialized nations,1–4 as well as in a growing number of developing countries.5–7 Leading to premature morbidity and mortality, and to preventable losses of employment, earnings, and quality of life, CVD is clearly of pressing clinical and economic significance, underscoring the need for effective primary prevention efforts that target common, modifiable risk factors. Prominent among these are the physiologic and anthropometric risk factors associated with the insulin resistance syndrome (IRS), and the neuroendocrine and psychosocial alterations that may both predispose to and result from these IRS-related abnormalities.
The IRS, also referred to as syndrome X or the metabolic syndrome, is a cluster of metabolic and hemodynamic abnormalities that both collectively and independently predict the development of atherosclerosis and CVD.4,8–11 Core features of the IRS are insulin resistance, glucose intolerance, atherogenic dyslipidemia, high blood pressure, and visceral adiposity.8,10–12 Other abnormalities associated with the IRS include impaired fibrinolysis and increased coagulability,10,13–15 chronic inflammation,10–12,15 endothelial dysfunction,10,16,17 and oxidative stress.16 Insulin resistance (ie, resistance to insulin-stimulated glucose uptake) is thought to be the primary underlying defect and a cardinal feature linking the IRS with CVD.8,15,16,18–20
Increased sympathetic activity, enhanced cardiovascular reactivity, and reduced parasympathetic tone have also been strongly implicated in the pathogenesis of IRS10,21–29 and in the development and progression of atherosclerosis27,28,30,31 and cardiovascular disease.21,25,28–36 In addition, recent research offers compelling evidence that chronic psychological stress and negative affective states contribute significantly to the pathogenesis and progression of insulin resistance,37–41 glucose intolerance,38 hypertension,42–46 dyslipidemia,38,41,47 and other IRS-related conditions28,37,48–55 and ultimately, increase risk for CVD morbidity and mortality.28,32,43,44,46,52,56–60
Not only can IRS-related conditions be exacerbated by lifestyle variables, such as smoking, lack of exercise, and poor diet, but these conditions can interact with one another in a destructive manner,61 likely accounting for their synergistic effect on CVD risk.9,62 Thus, a vicious cycle is initiated, which, as time goes on, becomes increasingly difficult to treat, highlighting the importance of early intervention. Given that IRS-related conditions affect a large percentage of the U.S. population,1,4,63 are now reaching epidemic proportions worldwide,1,64 and are powerful predictors of CVD morbidity and mortality,1,65 investigating potential cost-effective strategies for reducing IRS-related risk factors for CVD is clearly warranted.
In light of the strong influence of psychosocial factors on the development of both IRS and CVD, the role of sympathetic activation in the pathogenesis of insulin-resistant states, and the mutually exacerbating effects of these and other IRS-related risk factors, mind-body therapies may have considerable potential in the prevention and treatment of CVD. Of particular interest in this regard is yoga, an ancient mind-body discipline that has been widely used in India for the management of hypertension, diabetes, and related chronic insulin resistance conditions66,67–69 and may hold promise as a therapeutic intervention and health promotion measure for Western populations as well. Originating in India over 4000 years ago, the practice of yoga has been rising steadily in western industrialized countries during recent decades.70–72 Of the 7 major branches of Hindu yoga, Hatha (or forceful) yoga, Raja (or classical) yoga, and Mantra yoga are perhaps the best known and most widely practiced forms. Mantra yoga, emphasizing the use of specific sounds or chants to achieve mental and spiritual transformation, has been popularized in the West by Maharishi Mahesh Yogi, the founder of Transcendental Meditation (TM). Both Hatha yoga and Raja yoga emphasize specific postures (asanas), including both active and relaxation poses, as well as breath control (pranayama), concentration (dharana), and meditation (dhyana). Hatha yoga, the branch of yoga most commonly practiced in the Western industrialized world and which itself includes many different styles (eg, Iyengar, Kundalini, Ashtanga, Integral, and Bikram yoga), also incorporates mantras or chants, cleansing exercises (kriyas), and specific hand gestures (mudras).
Yoga is an economical, noninvasive practice that has become increasingly popular in the United States as a means of potentially relieving stress, enhancing health, and improving fitness.70–73 With no appreciable side effects and multiple collateral lifestyle benefits,70,72,74,75 yoga seems safe, is simple to learn, and can be practiced even by elderly, ill, or disabled individuals.76 Requiring little in the way of equipment or professional personnel, yoga also seems easy and inexpensive to maintain, with some studies indicating excellent long-term adherence,77–79 even in Western populations.79 Most importantly, there is a growing body of research suggesting that practice of yoga may reduce IRS-related risk factors for CVD, and may attenuate signs, reduce complications, and improve the prognosis of those with frank or underlying disease.67–72,75,78,80
However, despite yoga’s growing popularity and apparent promise as a safe and cost-effective intervention for populations with CVD or at risk for CVD, systematic reviews are lacking. In this article, we critically review the published scientific literature regarding the effects of yoga on IRS-related anthropometric and physiologic indices of CVD risk and on cardiovascular clinical outcomes, taking into account the major limitations and biases of these studies. We also briefly discuss mechanisms that may mediate the reported effects of yoga on CVD risk.
Methods
There seems to be mounting evidence that yoga may indeed reduce IRS-related indices of CVD risk and aid in the management of CVD and other IRS-related chronic disorders. To examine this evidence systematically, we first conducted a thorough search of the published medical literature. The search was restricted to English language articles published after 1970 and available in U.S. libraries, and to original studies specifically evaluating the effects of yoga (alone or in combination with other interventions) on cardiovascular disease or IRS-related risk factors for cardiovascular disease. Specifically, original studies were included in the review if they reported outcome data and evaluated the effects of yoga and yoga-based interventions on measures of insulin resistance, lipid profiles, body weight or composition, blood pressure, oxidative stress, coagulation/fibrinolytic profiles, or on markers of sympathetic activation and cardiovagal function. We also included studies assessing the influence of yoga and yoga-based programs on relevant clinical endpoints, including medication use, CVD-related events and hospitalizations, and measures of CVD progression.
Because this review is focused on the influence of yoga on physiologic and anthropometric indices of CVD risk, those studies exclusively evaluating psychosocial risk factors for CVD were excluded. Case studies, abstracts from conference proceedings, and anecdotal reports were also eliminated, as were studies with intervention group sizes of less than 4 subjects. Studies evaluating only the effects of TM programs on CVD risk profiles and clinical outcomes were likewise excluded (for a comprehensive review of research on the use of this intervention in the treatment and prevention of coronary heart disease, see King et al81). Articles were identified using MEDLINE, PubMED, and PsycINFO, 3 commercially indexed, scientific databases. Because the majority of studies investigating the effects of yoga therapy have been conducted in the Indian subcontinent and these databases offer only incomplete capture of articles published in Indian medical journals, IndMED, a bibliographic database of over 75 major Indian biomedical journals, was also searched. Search words included yoga, yogic, relaxation, mind-body, and meditation. In addition, the citation sections of all identified articles were scanned to identify relevant papers not indexed in PsycINFO, PubMED, MEDLINE, or IndMED.
Each eligible study (ie, each study identified that met our inclusion criteria) was classified into one of 5 design categories: randomized controlled trials, nonrandomized controlled trials, uncontrolled (pre and post) trials, cross-sectional (observational) studies, and studies assessing dynamic change in specific physiologic indices during 1 or 2 yoga sessions. In randomized controlled trials (RCT), a member of the investigative team randomly allocates a yoga or yoga-based program to one group (the experimental or yoga group) and no intervention, usual care, or another intervention to one or more other groups (controls). Both groups are then evaluated to determine change over time in specific indices of CVD risk. In nonrandomized controlled studies (controlled clinical trials [CCT]), a member of the investigative team allocates a yoga-based intervention to one group, and no intervention or another intervention to one or more other groups, but the allocation to a given treatment is not performed randomly. Both groups are again assessed to determine change over time in specific indices of CVD risk relative to baseline. In uncontrolled (pre and post) studies, all subjects participate in a yoga or yoga-based program, and change over time (baseline to post-intervention) in specific indices of CVD risk is evaluated. In cross-sectional (observational) studies, the investigator does not manipulate assignment of the intervention, but rather compares, at a single point in time, indices of risk between groups with varying experience in the practice of yoga. An additional study design category included studies that monitored temporary physiologic changes occurring during 1 or 2 yoga sessions; all but one of these studies82 included a comparison group and/or condition, although none were randomized.
We evaluated study quality using criteria based on those used in recent systematic reviews regarding the effects of another popular mind-body therapy.83,84 Criteria included (1) adequate sample size; (2) explicit eligibility criteria and/or adequate description of study population; (3) single, well-defined intervention; (4) appropriate control group(s) or comparison condition(s); (5) randomization of treatment allocation; (6) blinding of outcome assessment; (7) adequate accounting for confounders; (8) statistical methods well described and appropriate; (9) outcome measures well-defined and point estimates and measures of variability presented; (10) adequate follow-up/drop-out rate reported; and (11) conclusions supported by findings.
Outcomes evaluated were categorized into several different domains of CVD risk indices and clinical outcomes. For each domain, we summarized findings from relevant studies. Because of the heterogeneity of outcomes, study designs, settings, and interventions, we did not conduct a meta-analysis.
Results and Discussion
The literature search identified a total of 70 eligible studies on physiologic/anthropometric risk factors for cardiovascular disease and/or related clinical endpoints, including 1 cross-sectional study, 8 studies (7 controlled, 1 uncontrolled) examining changes occurring during 1 or 2 yoga sessions, 25 uncontrolled clinical trials, 15 nonrandomized controlled trials (including one study that also examined changes occurring during a single yoga session), and 22 RCTs (Table 1). The majority (63%) of identified studies were published between 1990 and 2004, and most were small in size, with over 40% having study populations numbering under 25 subjects. Almost 70% of the studies were conducted in India; in contrast, less than 5% of studies identified were performed in the United States. Yoga-based interventions used in these studies ranged in duration from 2 days to 12 months, and included a single (N = 18) or multiple components of yoga practice (N = 35), and comprehensive yoga-based programs that included a special diet, lifestyle education, nonyogic exercise, stress management, or other interventions (N = 17). The distribution of studies by study population and intervention (yoga alone versus multiple interventions) is given in Table 2. The majority of the studies identified for this review were conducted in healthy young to middle-aged adults (50%) or in adults with or at risk for cardiovascular disorders (30%). In contrast, few studies have evaluated the influence of yoga on CVD risk indices in populations with other chronic disorders (N = 9), or in healthy children (N = 3) or elderly adults (N = 2) (Table 2). Table 3 lists the characteristics of eligible studies identified. The findings of these studies regarding the effects of yoga-based interventions on specific physiologic and anthropometric indices of CVD risk and relevant clinical endpoints are reviewed below.
Characteristics of eligible studies investigating the effects of yoga and yoga-based programs on specific physiological and anthropometric indices of CVD risk and related clinical endpoints
Studies investigating the effects of yoga and yoga-based programs on specific physiologic and anthropometric indices of CVD risk and related clinical endpoints, by study population
Characteristics and relevant endpoints of eligible studies. Under endpoint categories, a plus indicates a beneficial change in at least one marker; a negative sign indicates no change in any of the markers in a specific category
Observed Effects of Yoga on Core Indices of the IRS
Since the 1970s, at least 51 eligible, published studies from 7 countries have investigated the potential influence of yoga and yoga-based programs on one or more core indices of the IRS, including measures of insulin resistance, lipid profiles, body weight and composition, and blood pressure. Our literature search identified 13 eligible studies examining the influence of yoga-based interventions on markers of insulin resistance (including 8 uncontrolled clinical trials, 2 nonrandomized controlled trials, and 2 RCTs), 14 studies evaluating the effects of yoga on lipid profiles (including 1 cross-sectional study, 5 uncontrolled clinical trials, 3 nonrandomized controlled trials, and 5 RCTs), and 18 studies assessing the influence of yoga on body weight or composition (including 9 uncontrolled trials, 3 nonrandomized controlled trials, and 6 RCTs. In addition, we identified 37 eligible studies evaluating the effects of yoga on blood pressure, including 1 cross-sectional study, 1 study examining changes during a single yoga session, 11 uncontrolled studies, 12 nonrandomized controlled studies, and 12 RCTs. Findings of these studies are summarized in Tables 4 and 6 and are discussed briefly below.
Summarized findings of studies (1970–2004) investigating the effects of yoga and yoga-based programs on insulin resistance, lipid profiles, and body size and composition, stratified by study design and intervention (yoga, including yoga-based meditation, alone vs. in combination with other interventions). Studies demonstrating beneficial effects are in bold type.
Markers of Insulin Resistance
Of the 13 studies evaluating the effects of yoga on markers of insulin resistance, most documented significant, postintervention improvement in one or more indices following the practice of yoga either alone or in combination with other therapies (Table 4). Interventions ranged in length from 40 days85,86 to 12 months,80,87 and all but one88 incorporated yoga asanas or postures. Seven of the 8 uncontrolled studies of healthy young adults,89,90 patients with type II diabetes mellitus (DM II)85,86,91,92 or hypertension68 reported significant improvement postintervention in indices of insulin resistance relative to baseline values. Documented changes included reductions in fasting68,80,85,86,88–90,92,93 and postprandial glucose,85,86,89,91,92 and in fasting glycohemoglobin;85–87 in the one uncontrolled study yielding negative results, a trend toward reduced glucose was observed in male subjects despite low baseline levels94 (Table 4). Likewise, nonrandomized controlled studies of healthy young adults88 and adults with coronary artery disease (CAD)80 reported reductions in fasting glucose among subjects receiving a yoga-based intervention versus controls receiving enhanced usual care80 or no active intervention88; descriptive findings of an additional small controlled study of healthy young men suggested similar improvement following a prescribed yoga program.93 In a small RCT of diabetic British adults, Monro et al demonstrated a decline in both fasting glucose and glycohemoglobin among participants attending structured yoga classes relative to usual care controls.95 Similarly, an RCT of American seniors demonstrated a substantial (19%) reduction in fasting insulin among high-risk subjects completing a comprehensive integrative medicine program including yoga meditation and asanas, although small sample sizes precluded statistical comparison with controls.87 Overall, yoga practice was associated with a 5.4 to 33.4% reduction in fasting glucose, 24.5 to 27.0% reductions in postprandial glucose, and 13.3 to 27.3% reduction in glycohemoglobin, with the percentages varying by study population and design (Table 5).
Observed percent change with yoga in selected physiologic and anthropometric indices of CVD risk*
Although the evidence for a beneficial effect of yoga on indices of insulin resistance is relatively consistent across studies, most studies (62%) had no comparison groups68,85,86,89–92,94 and many had small sample sizes68,85,86,89,90,93,95 or reduced power due to stratified analyses.87,92,94 Others lacked detailed information on eligibility criteria or study population characteristics,80,85,86,88,89,93 and blinding of the outcome assessment was reported in only one study.87 The study sample selection process was unclear in several studies,86,89,90,93 and in others, potential selection bias, differential loss to follow-up80 and uncontrolled confounding factors such as demographic, anthropometric, and lifestyle characteristics85,91–95 may have been important. The intervention was not well described88 or varied in duration91 in some studies; others included multiple interventions,68,80,87,92 rendering detection of the effect of a specific component difficult. Analytic methods were not well described in most studies68,85,86,88,90–95; no statistical analysis was presented in some,68,89,91,93 and many had methodological problems, including lack of adequate point estimates for key outcome measures,68,89,91,93 failure to adjust for multiple comparisons,68,87,88,90,91,94 confusing data presentation,68 and other potential analytic problems.87,88 Among controlled studies, additional limitations included lack of randomization,80,88,93 failure to describe treatment allocation methods,80 and or absence of intergroup comparisons.93
Lipid Profiles
Of the 14 identified studies that examined the potential effects of yoga on blood lipid concentrations, most offered evidence suggesting that the practice of yoga and yoga-based programs may improve lipid profiles. In a cross-sectional study of healthy middle-aged men with similar lifestyle characteristics, Vyas and colleagues found those with both short-term and long-term experience in Raja yoga meditation had reduced cholesterol and triglyceride levels relative to those with no yoga experience.96 Similarly, 4 of 5 uncontrolled studies68,89,90,97 and all 3 of the controlled, nonrandomized studies80,88,98 identified demonstrated significant positive changes in blood lipid levels following yoga-based interventions that ranged from 6 weeks97 to 12 months80 in duration. These studies included investigations of both healthy adults and patients with hypertension or CAD (Table 3). Observed changes included reductions in cholesterol and low density lipoprotein (LDL),68,80,88–90,97,98 and increases in high density lipoprotein (HDL) levels68 relative to baseline levels68,89,90,97 and/or control values.80,88,98 In agreement with these findings, several RCTs investigating the effects of yoga in combination with diet,78,80,99 education,79 stress management,79,80,100 and other therapies78,80,100 have likewise demonstrated significant improvement in lipid profiles relative to controls receiving enhanced usual care, exercise, and/or dietary interventions (Tables 3 and 4). Of the 5 RCTs identified, all adults with hypertension,101 CVD,78,100 or risk factors for CVD,79,99 3 documented improvement in all indices of dyslipidemia examined,78,79,99 and one reported significantly greater reductions in triglycerides, but not in cholesterol or LDL.100 In a follow-up of an earlier British study,102 Patel and colleagues reported maintenance of lipid profile changes at 8 months postintervention, but no differences between the yoga relaxation/meditation and the control groups at 4 years.79 Only one RCT, a study of 35 hypertensive Dutch adults (18 intervention group, 17 controls), reported no differences between the intervention and control groups.101 Of those studies demonstrating positive effects, yoga practice was associated with a 5.8% to 25.2% decrease in total cholesterol, 22.0% to 28.5% reduction in triglycerides, and a 12.8% to 26.0% reduction in LDL, with the observed magnitude of the effects differing by study population and design (Table 5).
Again, the vast majority of both uncontrolled and controlled studies suggest that the practice of yoga may have a positive influence on lipid profiles. However, many of the studies evaluated have methodological or other limitations that hinder interpretation of findings, including absence of comparison groups or conditions,68,89,90,94,97 low power because of small sample sizes68,89,90,97 or other factors,94,101 lack of evidence for blinded outcome assessment,68,79,80,88–90,94,96–101 possible uncontrolled confounding factors,94,96–101 potential selection bias,96,98,100 loss to follow-up,80 lack of randomization88,98 or information on the randomization process,78,79,99,100 unclear statistical analyses,68,79,88,90,94,97,98 and multiple68,78–80,99–101 or poorly defined interventions.88,97 Other methodological issues include lack of adequate point estimates,68,88,89,98 intergroup comparisons,100 or adjustment for multiple comparisons,68,88,90,94,98,100 possible floor effects,94 and inadequate description of study populations80,88,89,99,101 and of sampling or treatment allocation process.80,89,90
Body Weight and Composition
Between 1970 and 2004, 18 clinical trials in 6 countries examined the effects of yoga on anthropometric indices of CVD risk (Table 4). Six of the 8 uncontrolled clinical trials and 3 of the 4 nonrandomized controlled studies identified reported improvement in body weight80,89,91–93,98,103,104 or composition105 after yoga-based interventions ranging from 4 weeks103,105 to 12 months.80 Likewise, 5 of 6 randomized controlled trials, including 4 conducted in India78,99,106,107 and one completed in Thailand,100 demonstrated improvement in body weight and/or composition relative to usual care,78,100,107 diet and exercise,99 and no intervention controls.106 Studies reporting improvement in anthropometric characteristics included investigations of healthy populations,89,93,98,103–106 as well as those with hypertension107 and/or other CVD risk factors,99 CAD,78,80,100 or diabetes.91,92 Of those studies reporting improvement in anthropometric indices, yoga practice was associated with a 1.5% to 13.6% reduction in body weight (Table 5). All studies reporting a positive change in these indices used interventions incorporating active yoga asanas, whereas only one108 of those showing no effect, an uncontrolled 8-week study of 10 U.S. university students, included active postures as a central component in the intervention.
Limitations of these studies include lack of control groups,89,91,92,97,103–105,108 reduced power because of a low number of study subjects89,93,97,103,105,108,109 or other factors,92,101 possible selection bias98,105,108 or influence of uncontrolled confounding91–93,97–101,103,107,109 lack of appropriate statistical analyses or presentation,89,91,93,98 inadequate description of analytic methods,91–93,97,98,105,106 study population,* treatment allocation,80 or sample selection process,89,93,106 loss to follow-up,80,105,108 multiple comparisons,† failure to compare control and intervention groups,93,100,109 lack of randomization93,98,109 or description of randomization methods,78,99,100,106,107 and multiple interventions.78,80,92,99–101,104 In addition, only one study78 reported blinded outcome assessment.
Blood Pressure
Of the core indices of IRS, blood pressure is the endpoint that has been most extensively studied with respect to the influence of yoga-based interventions. Our search identified 37 studies from 6 countries, including 24 controlled studies. Over 75% of these studies report improvement in blood pressure with yoga or yoga-based interventions (Table 6). In a cross-sectional study of healthy mid-life men with similar lifestyle characteristics, Vyas and colleagues found those with both short-term and long-term experience in Raja yoga meditation had reduced diastolic blood pressure compared with those who were naïve to meditation.96 Of the 36 remaining studies evaluating change in baseline blood pressure with yoga and yoga-based programs, only 8 studies (22%) found no evidence of improvement, including a small German study of changes in healthy young female practitioners during a single yoga session,110 2 (20%) of the 10 uncontrolled studies,103,111 2 (17%) of the 12 nonrandomized controlled trials,112,113 and 3 (25%) of the 13 RCTs.101,114,115 Of the 4 uncontrolled and nonrandomized controlled trials with negative findings, all were small studies of healthy young Indian men that demonstrated no change in blood pressure, but an improvement in heart rate111,112 and/or other indices of cardiovascular function103,111,113; 2 of the 4 studies included active yoga asanas.103,112 RCTs yielding negative results included a 6-week study of healthy British elderly, and a 3-month study of healthy Indian boys that demonstrated no impact on blood pressure, but a significant reduction in heart rate and increase in heart rate variability (see below) in participants completing a yoga program compared with those receiving an aerobic exercise program114 or no intervention.115 In a third study of hypertensive Dutch elderly, the authors found a multimodal program that included training in yoga relaxation techniques to have no effect on 24-hour ambulatory blood pressure.101
Summarized Findings of Studies (1970–2004) Investigating the Effects of Yoga and Yoga-Based Programs on Blood Pressure, Stratified by Study Design and Intervention (Studies Reporting Beneficial Effects Are in Bold)
In contrast, 28 eligible intervention studies published between 1970 and 2004 reported a beneficial effect of yoga and yoga-based programs on blood pressure change (Table 6). These include 8 uncontrolled studies of healthy90,104,116,117and hypertensive adults,97,118,119 all but one of which97were conducted in India. Most of these studies were small, with only 3104,118,119 including 25 participants or more. Among nonrandomized controlled trials, 9 studies of healthy adults93,98 and adults with hypertension109,120–124 and/or CAD80 have demonstrated significant reductions in blood pressure among participants who completed a yoga-based intervention relative to controls receiving an exercise,125 enhanced usual care,109,121–123 or no intervention.98,125 Likewise, 11 RCTs of healthy adults125–128 and patients with hypertension or other CVD risk factors79,87,102,107,129–131 have demonstrated significant blood pressure declines among subjects receiving a yoga-based intervention versus controls receiving usual care,107,129 enhanced usual care with diet and exercise,87,128 social contact,131 placebo therapy,129,130 or no active intervention.107,127 In a study of 95 female Japanese university students, Cusumano and colleagues demonstrated comparable, significant reductions over time in blood pressure among women receiving 3 weekly training sessions in either Hatha yoga or progressive muscle relaxation.126 Overall, these studies demonstrated a 4.9% to 24.2% decline in diastolic blood pressure and a 2.6% to 21.3% decline in systolic blood pressure with yoga, with the magnitude of change varying with the study design and sample population (Table 5).
Yoga-based programs used in the 28 studies reporting positive findings ranged in duration from 30 days118 to 6 months119 in the uncontrolled studies, from 3 weeks120 to 6 months93,109,124 in the controlled nonrandomized studies, and from 8 days131 to 12 months87 in the RCTs. Interventions associated with blood pressure improvement included yoga routines both alone (N = 20) and in combination with other therapies (N = 8).‡ Of those studies using yoga alone, 10 incorporated active yoga asanas§ and 10 used relaxation postures alone117,119,123,131 or in combination with meditation.97,121,122,124,125,130
Collectively, the findings of both controlled and uncontrolled studies suggest that even the relatively short-term practice of yoga or yoga-based programs may reduce blood pressure. However, because of potential biases and limitations characterizing most of these studies, caution is nonetheless warranted in drawing firm conclusions. For example, interpreting the positive findings of many of these studies is hindered by absence of comparison groups,68,90,97,104,116–119 small sample sizes,‖ reduced power due to stratified analyses87,118,127 or other factors,101,131 possible selection bias or confounding by lifestyle or other factors,¶ absence of detailed information regarding the study population,** the intervention,97,121,124 statistical†† or randomization methods, treatment allocation,80,124 or subject selection process,90,93,117,119,123 potential uncontrolled variation in exposure to the intervention,96,118 or loss to follow-up.80,116,121,122 Few studies reported blinding of outcome assessment,87,128–130 and several studies used yoga in combination with other interventions,‡‡ making it difficult to detect an effect specific to yoga. Other methodologic limitations are lack of randomization93,98,109,121–125 and inadequacies in statistical analyses or presentation, including lack of appropriate point estimates,68,93,98 adjustment for multiple comparisons,§§ and appropriate comparisons between93,109,120,122,123,128,131 or within68,93,117,123 groups.
Observed Effects of Yoga on Indices of Coagulopathy and Oxidative Stress
Procoagulant changes and damage caused by oxidative stress are thought to mediate many of the atherosclerotic and thrombotic changes that are associated with IRS13,14,132–134 and to play a pivotal role in the development and progression of CVD13,132–134 and diabetes.135 Although few published studies have examined the possible effects of yoga and yoga-based interventions on coagulation profiles or oxidative stress, findings of these studies, summarized in Table 7, suggest that yoga may be instrumental in improving these important indices of CVD risk. An uncontrolled Indian study of 7 healthy young men naive to yoga demonstrated a significant decline in fibrinogen and a significant increase in fibrinolytic activity following a 4-month yoga training course, in addition to a pronounced, although nonsignificant increase in platelet aggregation and activated partial thromboplatin time, and a rise in blood platelets.136 Likewise, in a nonrandomized controlled study of healthy German adults, Schmidt et al documented a significant fall in fibrinogen among participants completing a 3-month residential Kriya yoga program relative to community controls matched on age, gender, and baseline fibrinogen levels (N = 76 subjects, including 38 controls).98 Although limited, these data suggest that yoga may foster beneficial changes in the coagulation and fibrinolytic systems, at least in healthy adults.
Cross-Sectional Studies and Clinical Trials Investigating the Effects of Yoga and Yoga-Based Programs on Coagulation Profiles and Indices of Oxidative Stress, Stratified by Study Design and Intervention: Summarized Findings (Studies Reporting Beneficial Effects Are in Bold)
We identified 5 eligible studies investigating the influence of yoga on measures of oxidative stress, including 2 uncontrolled clinical trials, 2 nonrandomized controlled clinical trials, and one RCT (Table 7). All but one of these studies100 were conducted in India, and all provide evidence that yoga may reduce oxidative stress in both healthy populations and those with chronic IRS-related disorders. In uncontrolled studies of Indian adults with uncomplicated diabetes mellitus,85 or hypertension,68 investigators demonstrated significant reductions in malonyldialdehyde (MDA), a circulating product of lipid peroxidation, following a 40-day yoga training course85 and a 12-week yoga lifestyle intervention,68 respectively. In agreement with these findings, nonrandomized controlled trials have shown significant reductions in MDA137 and other markers of oxidative stress137,138 in healthy young men completing a 10-week137 to 5-month138 yoga training program relative to matched untrained controls. Observed changes in other oxidative stress indices include increases in antioxidants138 and antioxidative enzymes,138 and reductions in free radicals.137 Offering further support for a direct effect of yoga on oxidative stress, Sharma et al documented significant improvement in several of these indices among trained participants during a single yoga session when compared with controls during rest138(Table 7). Similarly, in an RCT of 44 Thai patients with CAD, Jatuporn et al found those receiving a 4-month yoga-based lifestyle modification program but no medication showed significant increases in blood antioxidants relative to usual care controls, although MDA levels did not differ between groups.100
Together, the 7 studies reviewed above offer support for a possible beneficial influence of yoga on oxidative stress and coagulation profiles, at least in certain populations. Limitations of these studies include lack of appropriate comparison groups,68,85,136 small sample sizes,68,85,136,138 possible selection bias or uncontrolled confounding by lifestyle and other factors,85,98,100,136–138 lack of randomization,98,137 inadequate information regarding the study population,85,138 subject selection,136,138 intervention,138 or analytic methods,68,85,98,100,137 multiple interventions,68,100 and problems with data analysis or presentation.68,98,100,137 In addition, blinding of outcome assessment was not well-reported in any of the 7 studies identified.
Effects of Yoga on Markers of sympathetic/parasympathetic activation and cardiovagal function
Since 1970, numerous studies have investigated the effects of yoga on markers of sympathetic/parasympathetic activation and cardiovagal function. Our search identified a total of 42 studies from 6 countries, including 2 cross-sectional studies, 15 uncontrolled clinical trials, 16 nonrandomized controlled trials, and 9 RCTs. Findings of these studies are summarized in Table 8. Although some studies have yielded inconsistent results, over 85% offer some evidence that yoga promotes a reduction in sympathetic activation, enhancement of cardiovagal function, and a shift in autonomic nervous system balance from primarily sympathetic to parasympathetic. Key changes, reviewed briefly below, include significant reductions in respiratory and heart rate, in cortisol concentrations, catecholamine levels, and renin activity, in skin conductance, and in cardiovascular response to stress, as well as significant increases in heart rate variability and baroreflex sensitivity.
Cross-Sectional Studies and Clinical Trials Investigating the Effects of Yoga and Yoga-Based Programs on Markers of Sympathetic Activation and Reactivity, Cardiovagal Function, and Cardiovascular Recovery from Stress, Stratified by Study Design and Intervention: Summarized Findings (Studies Reporting Beneficial Effects Are in Bold)
Of the 27 studies investigating the effect of yoga on heart and/or respiratory rate, only 2 studies showed no change in either index, including a nonrandomized controlled study of 10 young athletes113 and an RCT of healthy young men.128 However, both of these latter studies demonstrated improvement in other indices of cardiovascular function. In contrast, 25 eligible intervention studies reported a beneficial effect of yoga and yoga-based programs on baseline respiratory rate, baseline heart rate, and/or heart rate after exercise (Table 8). Seven studies (of 8 total) have documented a 3.8% to 60.3% reduction in respiratory rate with yoga relative to baseline103,104,116,139,140 and/or controls receiving usual care123 or an aerobic exercise program141(Table 5). These investigations include studies in healthy adults103,104,116,139,140 and children,141 as well as in hypertensive adults.123 Similarly, 21 of 24 total clinical trials reported a 4.3% to 38.8% decline in heart rate relative to baseline,‖ ‖ engagement in a relaxing, nonyogic activity104,142–145 and/or controls receiving usual care,123 an aerobic exercise program,141 or no intervention.98,115,125,127 These trials included studies of healthy¶¶ and hypertensive adults107,123 and of healthy children.115,141 In addition, in a cross-sectional study of healthy middle-aged men, Vyas and colleagues found those who had been practicing yoga meditation for 5 years or more to have significantly lower baseline heart rates than those who with no meditation experience.96 Of those clinical trials demonstrating positive effects, yoga practice was associated with a 3.8 to 60.3% reduction in respiratory rate and a 4.3 to 38.8% decline in heart rate (Table 5).
Although findings regarding the effects of yoga on cortisol levels have been inconsistent, probably due in part to differing collection times and measurement methods, those regarding the influence of yoga on other neuroendocrine indices of sympathetic activation have been remarkably consistent overall (Table 8). Of the 13 studies investigating the influence of yoga practice on catecholamine levels, renin activity, and/or basal skin conductivity, 11 have demonstrated significant reductions in these markers of sympathoadrenal activation. These studies include investigations of healthy populations98,104,125,143,145 and those with hypertension68,102,117,120,124 or epilepsy.146 Only 2 small uncontrolled studies of healthy Indian adults, conducted by the same group of investigators in the 1970s, have yielded contradictory results.93,147 With respect to catecholamine levels, 4 of the 6 eligible studies identified demonstrated significant declines in 24 hour urinary catecholamines among yoga program participants when compared with baseline68 or to controls receiving usual care,146 sham yoga,146 or no intervention.98 Studies evaluating the possible effects of yoga on renin activity and basal skin conductance have yielded even more consistent findings; of the 3 studies examining the former, and 7 studies investigating the latter endpoints, all documented significant reductions in these markers with yoga practice alone*** or in combination with lifestyle education.68,102
Consistent with these results, findings from several studies suggest that yoga practice can lead to improvement in both cardiovascular reactivity to stress and cardiovascular recovery from stress (Table 8). Cardiovascular reactivity to stress, a factor strongly associated with insulin resistance148,149 is also a major independent predictor of hypertension, stroke, myocardial infarction, and cardiovascular mortality31; cardiovascular recovery from stress is a marker of vagal rebound that has likewise been strongly associated with CVD risk.150 Documented changes associated with the practice of yoga and yoga-based programs in the 7 eligible studies identified include: (1) significantly reduced blood pressure and heart rate responses to stress relative to baseline105,151 or controls receiving nonyogic exercise,112 usual care,152 or no intervention127,153; and (2) accelerated cardiovascular recovery time from stress compared with nonyoga resting poses144 or controls receiving usual care152 or no intervention.153
Finally, 7 recent studies in Indian111,115,120,140 and European36,114 populations suggest that participating in yoga and yoga-based programs can improve heart rate variability and baroreflex sensitivity in both healthy36,111,114,115,140,143 and hypertensive populations120 (Table 8). Low heart rate variability (HRV) and baroreflex sensitivity reflect impaired cardiovagal adaptability and suggest excessive sympathetic and/or insufficient parasympathetic tone.60,154,155 These alterations are, in turn, strong independent predictors of cardiovascular morbidity and mortality21,29,36 and are thought to mediate in part the effect of IRS-related abnormalities on these outcomes.21,156 In contrast, high HRV and baroreflex sensitivity are generally considered to indicate good cardiovagal adaptability and sympathovagal balance,155 permitting greater responsivity and sensitivity to changing environmental demands.
Collectively, this research suggests that even the short-term practice of yoga may produce marked reductions in sympathoadrenal activation, enhance cardiovagal tone, and promote sympathovagal balance. Several studies have demonstrated pronounced changes in markers of sympathetic/parasympathetic activity within a single yoga session (Table 8); others have documented significant beneficial alterations in baseline measurements in as little as 2 days in uncontrolled trials,140 3 weekly sessions in nonrandomized controlled trials,126 and 8 days131 in RCTs. Interventions associated with improvement in markers of sympathetic/parasympathetic activity and cardiovagal function include yoga routines both alone (N = 29) and in combination with other therapies (N = 10); of those studies using yoga alone, 16 incorporated active yoga asanas, 7 used relaxation postures alone or in combination with meditation, and 5 used meditation or breathing exercises alone (Table 3).
Although evidence for a beneficial influence of yoga on sympathovagal balance is remarkably consistent overall across this diverse array of studies, many studies have limitations that hinder conclusive interpretation of findings. Many had no comparison groups,††† small sample sizes‡‡‡ and/or comparison groups that differed in baseline characteristics.96,98,110,120,142,146,153 Over 50% of the studies identified had 25 or fewer subjects, and over 20% had less than 15. Others lacked detailed information on eligibility criteria and population characteristics,§§§ treatment allocation,113,124 and analytic methods,‖ ‖ ‖ and blinding of the outcome assessment was well reported in only a few studies.115,128 In others, loss to follow-up,105,114,116,146,157,158 variable exposure to or experience with the intervention,82,96,110–112,118,142–144 potential selection bias,¶¶¶ and uncontrolled confounding factors****may have been important. The yoga intervention was not well described in some studies,112,124,147,152 and several used multiple interventions.†††† Other methodological problems included lack of randomization‡‡‡‡ or description of the randomization process,§§§§ inadequate data analysis or presentation,68,89,93,98,112,117,123 multiple comparisons,‖‖‖‖ or absence of appropriate intergroup comparisons.¶¶¶¶.
Effects of Yoga on Clinical Endpoints
Several studies in Indian,68,78,80,91,92,109,119 European,79,95,121,122,129,130 and American populations87 have suggested that yoga may also be helpful in the management of CVD and other IRS-related chronic conditions. Our search identified a total of 14 eligible studies evaluating the influence of yoga and yoga-based interventions on clinical endpoints, including 4 uncontrolled trials, 4 nonrandomized controlled studies, and 6 RCTs (Table 9). In uncontrolled Indian studies of adults with hypertension68,119 and/or diabetes,68,91,92 completion of a simple91,119 or comprehensive yoga program68,92 was associated with a markedly reduced need for medication relative to baseline. In agreement with these findings, controlled studies of adults with hypertension109,121,122,130 risk factors for CVD79 and/or CAD,80 and diabetes95 showed a decline in need for drug therapy among those enrolled in a yoga-based intervention compared with controls receiving usual care,95 enhanced usual care,79,109,121,122 usual care plus a diet and exercise program,80 or placebo therapy.130 Controlled studies in Indian,78 British,79 and American87 populations also suggest that yoga-based programs may attenuate signs, reduce complications, and improve the prognosis of those with frank or underlying disease. For example, in an RCT of Indian men with CAD, those enrolled in a 12-month comprehensive yoga program showed retardation of coronary atherosclerosis, increased regression and reduced progression of vascular lesions, and reduced anginal episodes relative to usual care controls78; another, nonrandomized controlled study of CAD patients yielded similar results.80 In a group of generally healthy American seniors, those completing a 12-month comprehensive yoga-based program demonstrated a decline in carotid intimal media thickness, an indicator of carotid atherosclerosis, relative to those receiving usual care or a comprehensive medical, diet, and exercise intervention87; the decline was correlated inversely with adherence, suggesting a direct relation between the practice of this program and atherosclerotic change. There is also some evidence that the clinical benefits observed following yoga-based programs might persist long term. In a 4-year follow-up of an earlier RCT in hypertensive adults, Patel et al found that those who had participated in an 8-week comprehensive yoga relaxation program were less likely than usual care controls to be receiving treatment for CVD-related complications, to have experienced a serious coronary event, or to have electrocardiographic evidence of ischemia.79
Clinical Trials (>2 Sessions) Investigating the Effects of Yoga and Yoga-Based Programs on Clinical Outcomes, Stratified by Study Design and Intervention (Yoga, Including Yoga-Based Meditation Alone vs. in Combination with Other Interventions) (Studies Reporting Beneficial Effects Are in Bold)
Although promising, several of these studies have methodologic and other limitations, including absence of control groups,119,68,91,92 small sample sizes,68,95,109,119 lack of randomization,109,121,122 loss to follow-up,80,121,122 possible uncontrolled confounding factors,91,92,95,109,119 unclear statistical analyses,68,91 or absence of intergroup comparisons,109,122 multiple comparisons,68,87,91,109 apparent lack of blinded outcome assessment,***** and multiple interventions.68,78–80,87,92,129,130 Several lacked adequate descriptions of the study population,80,91,109,119,121,130 sample selection process,119 intervention,121 treatment allocation,80 or statistical methods.††††† In addition, reporting bias may have resulted in omission of negative findings, possibly inflating the apparent positive effect of yoga on clinical endpoints.
Yoga, Psychosocial Risk Factors for CVD, and Possible Underlying Mechanisms
Although methodologic and other limitations of many studies preclude drawing firm conclusions, the almost 70 investigations reviewed above nonetheless offer evidence that yoga may have a beneficial influence on many IRS-related risk factors for CVD, may improve clinical outcomes, and may aid in the management of CVD and other IRS-related conditions. In addition, a growing number of studies from both Western and non-Western countries suggest that yoga therapy may be effective in reducing psychosocial risk factors for CVD as well. For example, yoga has been reported to decrease perceived stress109,159,160 and reactivity to stressors,110 enhance stress-related coping,161 reduce symptoms of depression127,128,162–165 and anxiety,66,127,161,162,166,167 and decrease anger,162,168 tension, and fatigue.162,169 Likewise, recent studies in India66,159,170 and the United States171 have indicated that yoga practice may improve sleep in both healthy66,159 and chronically ill populations.170,171
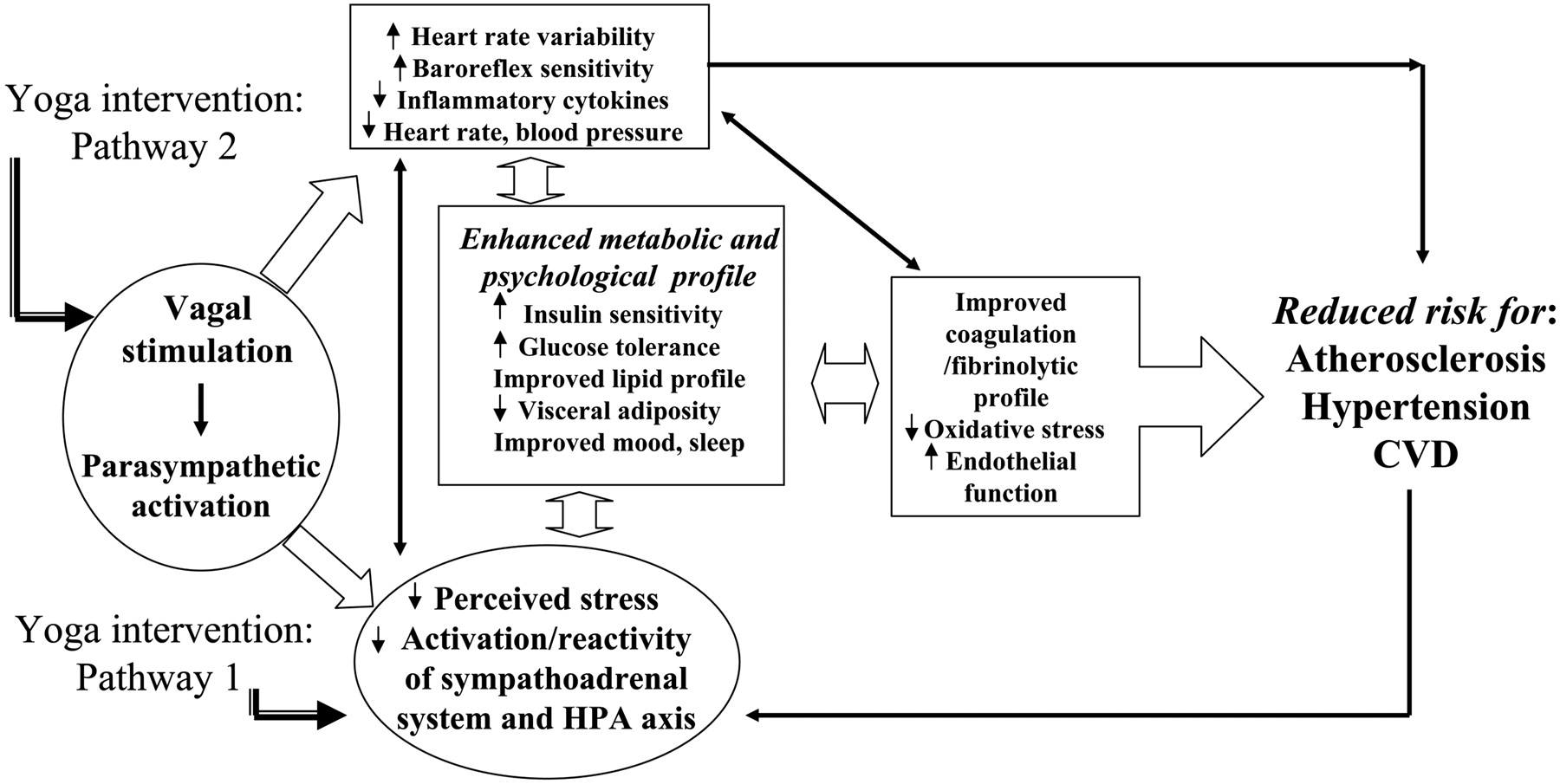
Although the mechanisms underlying the putative beneficial effects of yoga therapy on cardiovascular risk profiles are not yet well understood, the observed changes probably occur primarily through 2 pathways. First, by reducing the activation and reactivity of the sympathoadrenal system and the hypothalamic pituitary adrenal (HPA) axis and promoting feelings of well-being, yoga may alleviate the effects of stress and foster multiple positive downstream effects on neuroendocrine status, metabolic function and related inflammatory responses (Figure 1, pathway 1). Second, by directly stimulating the vagus nerve, yoga may enhance parasympathetic output and thereby shift the autonomic nervous system balance from primarily sympathetic to parasympathetic, leading to positive changes in cardiac-vagal function, in mood and energy state, and in related neuroendocrine, metabolic, and inflammatory responses (Figure 1, pathway 2). Yoga may also provide a positive source of social support, a factor strongly associated with CVD risk,32,38 may aid in improving health-related attitudes and lifestyle choices, in part by enhancing psychological well-being,38 and in this way may play an important role in CVD prevention and health promotion.38

Hypothesized Pathways by Which Yoga Intervention May Enhance Cardiovascular Risk Profiles
Summary and Conclusions
In summary, a substantial body of published research suggests that yoga may be instrumental in improving core indices of the IRS, including glucose tolerance and insulin sensitivity, lipid profiles, anthropometric characteristics, and blood pressure in a both healthy populations and those with chronic IRS-related conditions. In addition, more limited data indicate that yoga may improve coagulation profiles, at least in healthy populations, and reduce oxidative stress in both healthy adults and populations with serious chronic disorders. There is also mounting evidence to suggest that yoga may reduce sympathetic activation and enhance cardiovagal function, factors strongly associated with both IRS and CVD risk. In addition, findings from several studies, including several recent controlled trials,78,80,87 indicate that yoga may be useful in the management of CVD and related conditions, and in the prevention of CVD in those at risk.
However, despite the growing popularity and apparent therapeutic potential of yoga in the prevention and management of CVD, and the now considerable body of published literature on this topic, relatively few rigorous, controlled studies have been conducted on the effects of yoga on physiologic and anthropometric indices of cardiovascular risk; even fewer have been conducted in western populations. Since 1970, approximately 70% of clinical trials investigating the effects of yoga practice on CVD disease risk and clinical outcomes have been conducted in Indian populations, for whom yoga is an integral part of a long-standing cultural and spiritual tradition. Interpretation of many existing studies is also limited by small sample sizes, lack of appropriate control groups, inadequate description of methods, selection bias, failure to adjust for lifestyle characteristics and other potential confounders, exposure to multiple interventions, inadequacies in statistical analysis and presentation, or other methodological problems. In many of the controlled trials, treatment allocation was not randomized, and direct statistical comparisons were not made to control groups, potentially biasing the findings. In addition, the large variation in the nature, duration, intensity, and delivery methods of the yoga-based interventions used, even among studies using yoga practice alone, renders comparison across studies difficult. Publication bias may also play a role in the selective reporting of positive results,172 particularly in non-Western countries, where yoga is more widely embraced and more likely to be incorporated into medical treatment. Although existing RCTs have yielded results consistent overall with those of nonrandomized and uncontrolled studies, suggesting that the positive findings of these latter studies do not simply reflect bias because of poor study design, clearly, additional high quality RCTs are warranted. Specifically, rigorous, well-designed studies are needed to elucidate the effects of standardized yoga programs on IRS-related indices of CVD risk and related clinical endpoints, especially in American and other Western populations that remain underrepresented in the current literature.
Acknowledgments
We thank Dr. Ada Jacox for very helpful comments on an earlier draft of this article.
Notes
Funding: This work was made possible by grant S-T32-AT00052 from the National Center for Complementary and Alternative Medicine (NCCAM). The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of the NCCAM, or the National Institutes of Health.
Conflict of interest: none declared.
↵* See References 80, 89, 91, 93, 99, 101, 104, 106, 107, 109.
↵‖ See References 68, 90, 93, 97, 109, 116, 117, 119, 120, 124, 125.
↵¶ See References 93, 96–98, 101, 107, 109, 118–120, 124–127.
↵** See References 80, 93, 101, 104, 107, 109, 117, 119, 121, 123, 130, 131.
↵†† See Refernces 68, 79, 90, 93, 97, 98, 102, 116–119, 121–123, 125, 131.
↵‡‡ See References 68, 79, 80, 87, 101, 102, 104, 118, 129, 130.
↵§§ See References 68, 87, 90, 98, 104, 109, 116, 123, 125, 127.
↵¶¶ See References 90, 93, 98, 104, 111, 114, 116, 117, 125–127, 142–145.
↵††† See References 68, 82, 89, 90, 103–105, 111, 116–118, 139, 140, 147, 151, 157, 158.
↵‡‡‡ See References 36, 68, 82, 89, 90, 93, 103, 105, 110, 111, 113, 115–117, 120, 124, 125, 142, 145, 147, 151, 153.
↵§§§ See References 82, 89, 90, 93, 104, 107, 112, 115, 117, 123, 139–142, 147, 151–153.
↵‖ ‖ ‖ See References 68, 82, 90, 93, 98, 102, 105, 111–113, 116–118, 123, 125, 144, 147.
↵**** See References 93, 96, 98, 103, 107, 110–113, 115, 118, 120, 124–127, 139, 153, 157.
↵‡‡‡‡ See References 93, 98, 110, 112, 113, 120, 123–125, 153.
↵‖‖‖‖ See References 68, 90, 98, 104, 105, 110, 111, 113, 115, 116, 123, 125, 127, 139, 140, 142, 144, 151, 152, 157, 158.
↵¶¶¶¶ See References 93, 112, 114, 115, 120, 123, 128, 141, 143, 153.
↵***** See References 68, 79, 80, 91, 92, 109, 119, 121, 122.
- Received for publication January 5, 2005.
- Revision received May 20, 2005.
- Accepted for publication March 31, 2005.




{kind=link}