
Abstract
Background: Choosing which issues to discuss in the limited time available during primary care visits is an important task for complex patients with chronic conditions.
Design, Setting, and Participants: We conducted sequential interviews with complex patients (n = 40) and their primary care physicians (n = 17) from 3 different health systems to investigate how patients and physicians prepare for visits, how visit agendas are determined, and how discussion priorities are established during time-limited visits.
Key Results: Visit flow and alignment were enhanced when both patients and physicians were effectively prepared before the visit, when the patient brought up highest-priority items first, the physician and patient worked together at the beginning of the visit to establish the visit agenda, and other team members contributed to agenda setting. A range of factors were identified that undermined the ability of patient and physicians to establish an efficient working agenda: the most prominent were time pressure and short visit lengths, but also included differing visit expectations, patient hesitancy to bring up embarrassing concerns, electronic medical record/documentation requirements, differences balancing current symptoms versus future medical risk, nonactionable items, differing philosophies about medications and lifestyle interventions, and difficulty by patients in prioritizing their top concerns.
Conclusions: Primary care patients and their physicians adopt a range of different strategies to address the time constraints during visits. The primary factor that supported well-aligned visits was the ability for patients and physicians to proactively negotiate the visit agenda at the beginning of the visit. Efforts to optimize care within time-constrained systems should focus on helping patients more effectively prepare for visits. Physicians should ask for the patient's agenda early, explain visit parameters, establish a reasonable number of concerns that can be discussed, and collaborate on a plan to deal with concerns that cannot be addressed during the visit.
Primary care has become increasingly complex. With the overall aging of the primary care population, many patients have multiple concurrent conditions including social or economic stressors that affect their health.1,2 In parallel with this trend of greater patient complexity, an increasing focus on practice guidelines and performance measurement has significantly added to the number of items that primary care physicians (PCPs) are expected to address during time-limited visits.3,4 In this context of too much to do in too little time, the ability of patients and their physicians to work together to identify and align priorities for a visit may represent a critical, underdeveloped skill necessary for effective primary care.5 Such effective collaboration is of particular importance for complex patients due to the many different questions and concerns these patients may have about their health care.
Prior studies have found that complex patients and their physicians agreed on the top visit priorities up to two thirds of the time.6,7 When patients and physicians differed, patients typically prioritized discussing their current symptoms whereas physicians prioritized guideline-based prevention and chronic disease management.7 Research on patients with diabetes has shown that when patient-physician communication is suboptimal, patients have worse adherence and poorer clinical outcomes.8⇓–10 To date, there has been little research investigating how patients and physicians prepare for, prioritize, and align visit agendas.
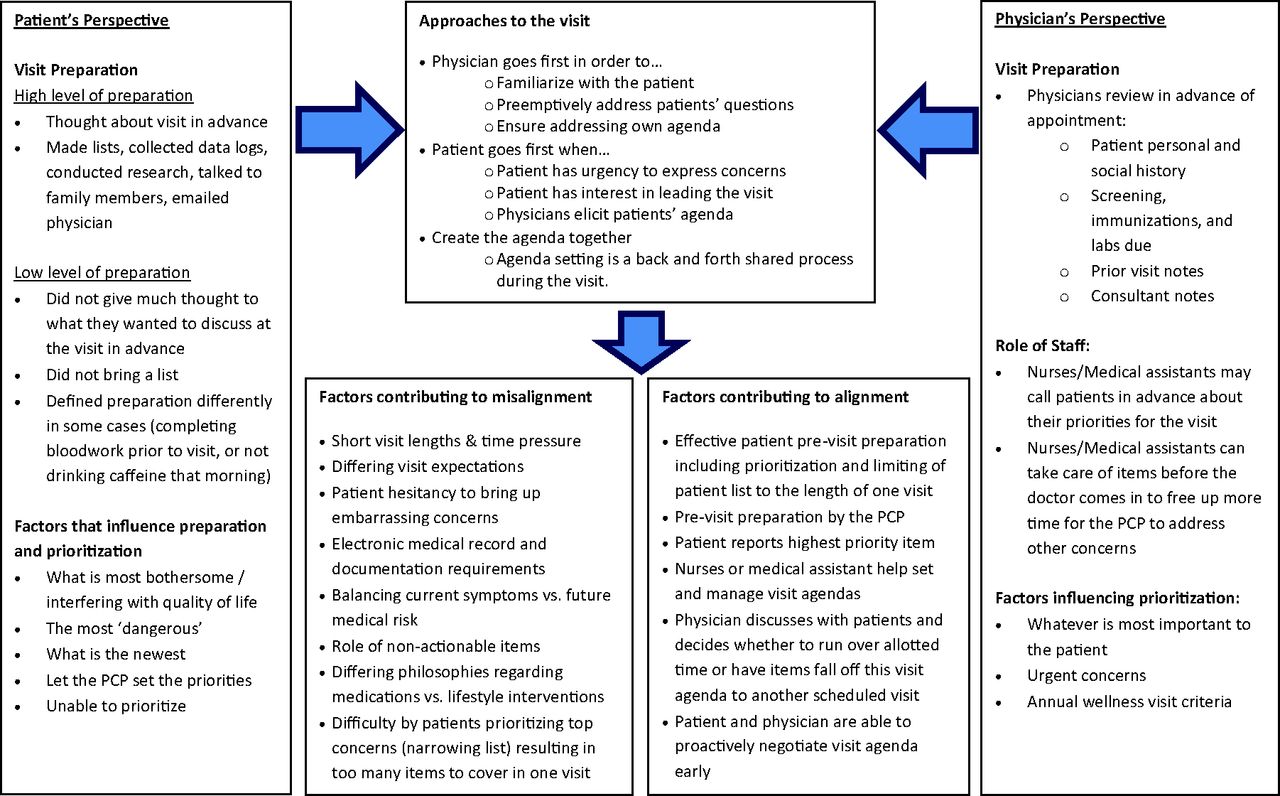
Given that effective primary care requires collaboration between patients and physicians, further insight into the barriers and facilitators to aligning patient and physician visit priorities may be helpful for efforts to improve communication during time-limited visits. To address this need, we separately interviewed complex patients and their PCPs to: 1) examine how patients and physicians prepared for upcoming visits; 2) gain further insight into how agendas are set during visits; and 3) identify factors that facilitate or impede alignment of visit agendas. We also developed a conceptual model (Figure 1) to better understand the factors that influence patient and provider visit alignment.

Schematic diagram of factors influencing patient-provider visit agenda alignment. PCP, primary care physicians.
Methods
Study Sample and Design
We conducted a longitudinal, qualitative study in 3 geographically diverse health care settings: Kaiser Permanente–Northern California; Kaiser Permanente–Colorado; and University of Michigan–Ann Arbor. Study sites included both hospital-based and community-based practices serving a wide range of patient populations. Data were collected between January and December 2015. In-person interviews lasted approximately 45 minutes. Each interview was digitally recorded and transcribed verbatim. Institutional review boards from each of the 3 sites provided approval for this study.
PCPs (11 internal medicine and 6 family medicine) were recruited from each of the clinics and asked to identify and approve subsequent recruitment of their complex adult patients, defined as having 2 or more chronic conditions. Patients from each physician panel and the physicians themselves were continually recruited until qualitative data discovery had reached saturation.
The interviews proceeded sequentially in a longitudinal design with patient then PCP then patient again; patient priorities were shared with the PCP after the PCP listed their priorities for each patient. The interviews with the patients were most often collected in the weeks before a scheduled visit or in the clinic on the same day of their visit before being seen. Discussions with physicians occurred after the patient's visit, generally the same day or in the weeks following. We reinterviewed patients several weeks later to explore with them their thoughts about how their provider's priorities may have differed from their own.
Conceptual Model
Our patient interview guide was developed collaboratively across the 3 study sites and included the following qualitative domains: patient involvement with decision making about their care; patient strategies used for visit preparation; process of agenda selection; structure of the last primary care visit, including the ebb and flow of the visit and content covered; barriers to addressing patient agenda items; and identification of the patients' top 3 priorities for their upcoming PCP visit. After the interviews were completed we developed a conceptual framework (Figure 1) based on the interview data in which patients and physicians come in to the visit with their own unique perspectives for what occurs during the visit.
We developed the physician interview guide based on a review of the literature for physician and patient communication and prioritization. The guide included the following domains identified before the interviews: process of eliciting patient concerns and priorities; barriers to covering all patient concerns; barriers and facilitators to alignment of priorities; and top 3 priorities for upcoming visits. We also obtained permission from each patient to share their upcoming visit priorities with their PCPs. We then elicited the PCP's own priorities for that patient's visit to gain more specific insight into how patients and their physicians differed in their perceived visit priorities.
Qualitative Methods
We analyzed transcripts from the patient and physician interviews using data-derived directed content analysis.11⇓–13 After each interview, interviewers (PhD researchers with expertise in qualitative methods [CK, NC, CL] working in collaboration with physician researchers trained in primary care [MH, EAB, RWG]) created detailed qualitative summaries based on the interview content. Then, each team member read through the summaries and using an iterative process, we developed a preliminary coding schema. Data analysis started with immersion in the data to obtain a sense of the whole, followed by making labels for initial codes that emerged as reflective of more than 1 key thought. Subsequently each team member independently coded transcripts, and then met as a group to discuss and reconcile codes, identify emergent themes, and resolve discrepancies through consensus.
Each interviewer coded their own transcripts and produced comprehensive coding reports for each of the key themes. The main coding team (CK, DBM, NC), consisting of 1 researcher from each site, met biweekly to review and compare coding reports and key quotes across sites. The overall research team, including all the authors, met monthly over a period of 12 months to discuss and finalize the themes. Any disagreements were resolved through consensus discussion and by returning to the original data for confirmation. The themes were then compared within and between sites to better understand similarities and differences.
Results
We interviewed 40 patients (23 women, 17 men; mean age, 69.4 years, range, 37–92 years) and 17 physicians (12 women, 5 men) across the 3 study sites. Four of the 17 physicians had 1 patient in the study, 6 had 2 patients, 2 had 3 patients, and 4 physicians had 1 patient. Patients had a wide range of health conditions including diabetes, heart disease, depression, and arthritis.
Patient and Physician Preparation for Upcoming Visits
The majority of patients reported some form of previsit preparation, including written lists of concerns (eg, handwritten, smart phone), emails to physicians, information seeking about conditions or medications, or discussion of priorities with family members/spouses. In addition to lists, well-prepared patients brought data logs (eg, blood pressure readings, glucose levels) in printouts or as data in an electronic device such as a tablet or cell phone.
Patients commonly noted 2 main reasons for previsit preparation. The first was to ensure they did not forget or were not too intimidated to mention something (Quote 1, Table 1). A second reason was to make sure that their agenda was incorporated into the discussion with PCPs so that mutually developed strategies were employed to work toward patient health goals. Other patients did not prepare for their visits with PCPs, most commonly because they felt that the physician's agenda should drive the visit or due to the perception that there was not much wrong with their health.
Illustrative Quotes from a Qualitative Study of Preparation, Prioritization, and Agenda Setting by Complex Patients and their Physicians during Primary Care Visits
Most PCPs reported a uniform method of previsit preparation for all patient encounters; they reviewed their patient's previous clinical notes in advance and recent specialist notes and labs to remind them about what was discussed and what items the patient may be due for (eg, vaccines, lab screenings, mammograms) or that require followup. Physicians spent time preparing so that they would have more time to listen to patients and build rapport (Quote 2).
Physicians generally appreciated when the patient was organized and prepared with a list, but with caveats around list length and expectation setting (quote 3). Physicians also expressed concern about patients with very lengthy lists (quote 4). Physicians preferred that the patient bring up items during a visit, as opposed to contacting them afterward about a forgotten item. Conversely, some PCPs worried about unmet expectations, stating that just because an item is on a patient's list does not mean it will get covered.
Insights into Agenda Setting
Patient agenda-setting strategies typically fell into 3 types: 1) letting the provider set the priorities (Quote 5); 2) prioritizing based on symptoms, sometimes expressed as what was interfering the most with their quality of life (Quote 6); and 3) prioritizing based on creating a mutual agenda (Quote 7).
Three key themes emerged regarding how PCPs set their visit agendas: 1) prioritizing the most important of the patient's listed concerns, 2) prioritizing items they considered urgent and/or dangerous, and 3) acknowledging that “realistic prioritizing” meant some items would “fall off” the agenda. One PCP described joint prioritization of visit topics and agenda setting as an interaction that gets easier in time, but can be very difficult in the beginning (Quote 8). Another PCP described how his view of patient lists has changed over the years (Quote 9).
Factors that Facilitate or Impede Alignment of Visit Agendas
Both patients and physicians acknowledged that effective patient and physician previsit preparation was an important facilitator contributing to alignment. Both also agreed that both the need to prioritize topics for discussion and early joint-agenda setting were important facilitators (see Quotes 3, 7, 8, and 9). To help prevent patient delays in raising stigmatizing concerns, some physicians thought it would be useful to reassure patients about that safety of raising such concerns (Quote 10).
Patients noted 2 major barriers to alignment of priorities: 1) short visit lengths, and 2) difficulty in raising sensitive concerns. While some patients described having enough time with their PCPs to address their needs, others felt that short visit lengths made it difficult for them to communicate their priorities. For example, 1 patient described a list of 5 things that she wanted to address in the visit but could not (Quote 11). Similarly, another patient described not asking about an immediate health concern due to lack of time with the PCP (Quote 12).
Potentially embarrassing or stigmatizing concerns were another source of misalignment that affected visit flow because patients described waiting until the very end of the visit to raise these. Examples of these types of concerns provided by our patients included sexual dysfunction, blood in stool, anxiety, panic attacks, depression, suicidal ideation, and housing issues. Sometimes such concerns did not get addressed at all (quote 13).
Physicians described short visit lengths, added burden of computer documentation, differences in relative ranking of condition importance (and mismatched views about the number of concerns that can be addressed in a single visit), nonactionable items, patient hesitancy to bring up embarrassing or stigmatizing concerns, and differences related to medications versus lifestyle management as important barriers to aligning priorities with their complex patients.
Physicians agreed with patients on the challenges of limited visit times and the need to establish priorities from longer lists of potential concerns. Many physicians described experiencing stress surrounding the process for setting priorities and time limitations in an increasingly complex primary care patient population (Quote 14).
Despite the reported time constraints, several physicians reported that they went over the allotted appointment time to address all the patients' concerns. Patients valued knowing that their physician would take extra time with them when necessary, realizing this may mean that the physician would be running behind in clinic at times (Quote 15). Patients also expressed awareness that if they were going over their allocated time, another patient would be affected (Quote 16).
Physicians expressed concerns over the added burden of necessary computer documentation, for example, electronic medical record (EMR), within time constraints (Quote 17). Some physicians discussed how they attempt to overcome the EMR focus during their patient visits (Quote 18). A patient in the corresponding dyad to that PCP independently noted that he really appreciates how his PCP reviews his chart before he arrives for the visit and does not enter things into the EMR while speaking to him (Quote 19).
Another frequent source of misalignment between patient and physician involved differences in relative ranking of condition importance, which generally reflected a greater patient focus on current symptoms compared with the physician tendency to prioritize medical risk reduction. For example, 1 patient receiving end-of-life treatment for renal failure wanted to focus on what the physician considered the comparatively less important issue of toenail fungus. Another patient prioritized his eczema and felt his heart was fine, whereas his physician prioritized cardiovascular risk reduction due to his past history of a heart attack. Some patients felt that all the items on their list were important and they could not rank 1 over another, while other patients preferred to let their physician prioritize.
Items perceived by physicians as “nonactionable” tended to create a barrier to effective agenda coordination. PCPs reported that a key goal while listening to patient information was to determine actionable steps for patient care. For example, 1 physician described frustration with receiving excessive, nonactionable information (Quote 20). “Nonactionable” items could also include existing patient concerns that had been previously addressed. For example, 1 patient had listed her dizziness as a top priority, while her physician reported that this symptom had been extensively evaluated in the past and that no further management actions were planned.
Patient delays in raising concerns (or physician inability to elicit them early in the visit) led to the problem of new issues coming to light at the end of the visit (Quote 21). One final example of potential misalignment was differences related to medications versus lifestyle management. One patient described how she felt her PCP was “pushing” medication to manage her elevated blood pressure and early diabetes; however, she preferred to focus on a strict diet and exercise plan to avoid having to take additional medications.
Discussion
Through qualitative interviews with complex patients and their PCPs, we found that visit preparation and alignment of visit agendas were critical concepts influencing primary care visit interactions. Time constraints require patients and physicians to implement proactive strategies early in the visit to better manage their limited time together. When this process was not well aligned, interactions during visits tend to suffer. In Table 2, we summarize simple advice from physicians to patients and from patients to physicians.
Key Tips for More Effective Primary Care Visits
Many of the complex and typically older adults in our study expressed some difficulty in being able to visit priorities. Prior quantitative research has shown that the initial starting point for a visit has a very large impact on the subsequent content of that visit. For example, 1 study using videotaped encounters revealed that the first item addressed in the primary care visit received the bulk of the subsequent attention for that visit.14 Prior studies have also shown that many patients tend to leave important concerns until the end of the encounter, adding to the time pressure of the visit.15⇓–17 We found that many these delayed or deferred concerns were considered embarrassing or stigmatizing by the patients. This barrier has been described in other studies as “unvoiced concerns” and “disclosure deliberations”18,19 that often include issues related to sexual activity, depression or anxiety, financial or domestic problems, or physical function.18
Our results extend prior research on the importance of list making.20 We found that truly effective previsit preparation required an important additional step in which patients effectively prioritize and limit the length of their lists to fit within the constraints of a single visit. Moving from simple list making to active prioritization is an advanced skill.21 Even among patients who make lists, we found several examples of persistent misalignment that could potentially be alleviated and reflected the broader theme of differences between patients and physician perspectives. Many patients focused on current symptoms whereas physicians highlighted reduction of future medical risk. Similarly, several patients preferred lifestyle interventions and resisted medication prescriptions.22,23 Efforts to educate both patients and physicians on their counterpart's perspectives (Table 2) may help both to more quickly and effectively negotiate the visit agenda.
One novel issue identified in our study underscoring differences between patients and physicians was the concept of “nonactionable” items. These items, while important for understanding the patient's current circumstances, did not require any specific action on the part of physicians. In the context of needing to make best use of limited time, several physicians preferred that patient lists highlight items that could be directly addressed.
Our findings must be viewed in the context of our study design. Because this was a qualitative study, our results are better suited for hypothesis generation and cannot be used to infer causality. Moreover, patient and provider interviews with research staff may not fully capture the “true” interaction that occurs during visits. We did not note any significant thematic differences between the internal medicine and family medicine physicians, although we did not systematically explore this. Finally, while interviews were conducted in a wide range of geographic locations, all patients were insured and English speaking, and thus results may not be generalizable to other settings and patients.
Based on our results, we suggest 3 potentially strategies for improving primary care. The first is patient education on how to prepare for visits. Such education should go beyond recommendations for list making to developing skills related to prioritization, engagement in care planning, and disclosure. The second is physician training: Physicians, too, could benefit from early career training in how to work with patients to set up a visit agenda and how to balance individual patient needs with clinical efficiency during busy clinic days. The third is greater involvement of other care team members and family. This strategy is consistent with the Patient-Centered Medical Home model24 and Wagner's Chronic Care model25, both of which describe a team-based approach to the primary care of complex patients.26 Making significant changes to our current system is a major long-term endeavor. Our findings suggest initial efforts focused on patient and provider training related to visit preparation and agenda setting may help improve the complex process of primary care.
Notes
This article was externally peer reviewed.
Funding: Research reported in this publication was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (CDR-1403-11992). The views, statements, and opinions in this article are solely the responsibility of the authors and do not necessarily represent the views of the PCORI, its Board of Governors, or Methodology Committee.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/1/29.full.
- Received for publication April 19, 2017.
- Revision received August 30, 2017.
- Accepted for publication September 23, 2017.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Filling a gap in safety metrics: development of a patient-centred framework to identify and categorise patient-reported breakdowns related to the diagnostic process in ambulatory care
- Patient-Defined Visit Priorities in Primary Care: Psychosocial Versus Medically-Related Concerns
- Yonder: Patient complaints, after-visit summaries, rectal bleeding, and the doorknob phenomenon
- Interventions Must Be Realistic to Be Useful and Completed in Family Medicine