
Article Figures & Data
Figures
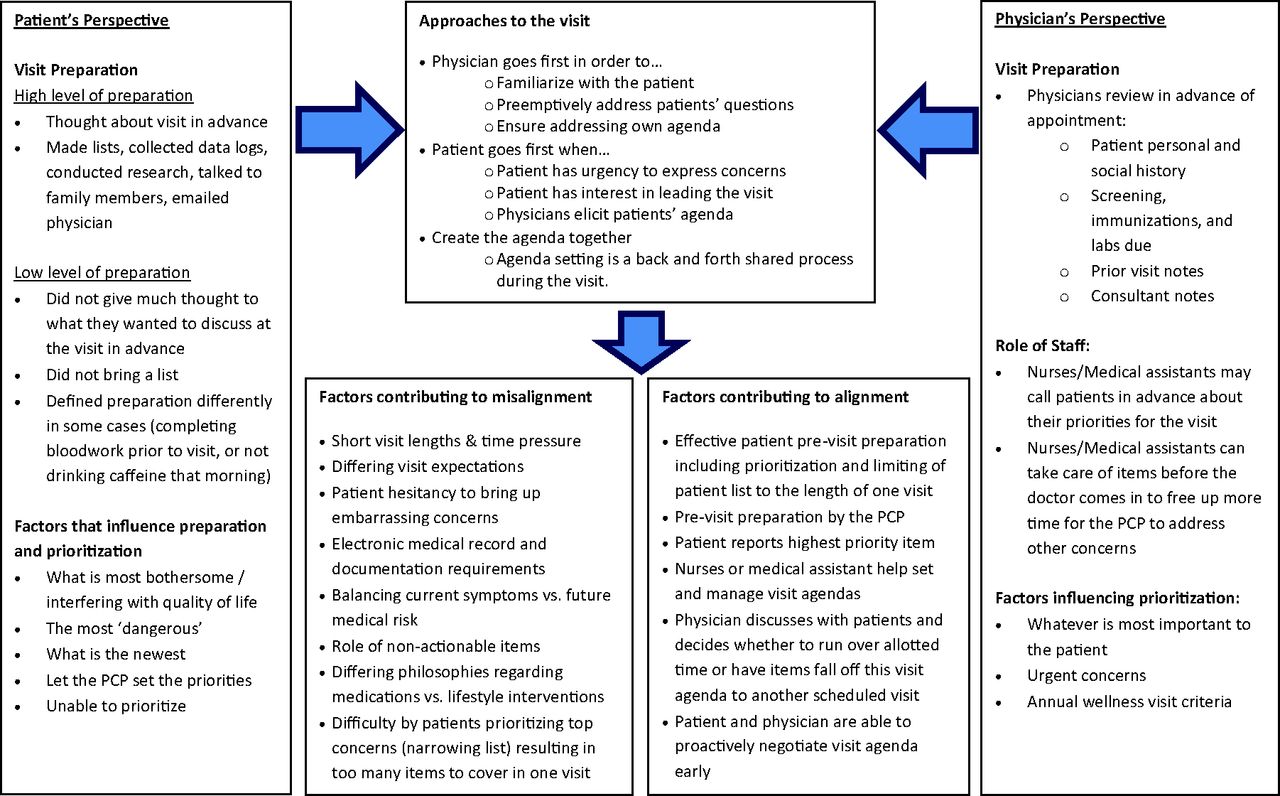
- Figure 1.
Schematic diagram of factors influencing patient-provider visit agenda alignment. PCP, primary care physicians.

Tables
- Table 1.
Illustrative Quotes from a Qualitative Study of Preparation, Prioritization, and Agenda Setting by Complex Patients and their Physicians during Primary Care Visits
Quote No. Interviewee Type Quotation Primary care visit preparation 1 Patient “You don't think about that when you are right in that room. It's that white coat syndrome, you kind of freeze up a little.” 2 Physician “You're able to listen to them better because you've got everything ready there for you.” 3 Physician “Sometimes I'll have patients throw something at you as you're trying to walk out the door; you think you're all done and then, ‘Oh, there was one more thing,’ I will actually address it the first or second time it happens and say, ‘What you can do to make things go better and make this visit less stressful is to bring in a list, write it ahead of time so that you remember everything you want me to deal with, and then we'll be able to get through everything.’” 4 Physician “Because I know the more they have on their list, even though I try to address it, the less I think I'm giving them what they need, because there's just so much …” Insights into agenda setting for primary care visits for medically complicated patients 5 Patient “I basically let him [doctor] set the priorities because there's certain things that are more critical than others, like my blood pressure, he really likes to make sure that that's well controlled.” 6 Patient “Something I couldn't take or stand.” 7 Patient “I say [to myself], ‘Okay, how are you going to prioritize what you're going to say and then what are you're going to obey?’ because if I'm paying $93 a visit I want to be compliant, but on things that I feel, both of us feel are important.” 8 Physician “I've been doing this for 20 years and at the beginning this was very difficult—because patients often come in with a very long list and you need to be able to learn to help them and yourself sort out what are the most important things that need to be talked about today.” 9 Physician “When I first started out in medicine, I hated lists. I love lists now. The best list is one you can take from the patient yourself and look at, but even if they just have a list because then they don't have that ‘by the way’ as you walk out the door, ‘I'm having rectal bleeding, or chest pain, or shortness of breath.’” Factors that facilitate or impede alignment of visit agendas 10 Physician “Don't be embarrassed, no matter what it is, your doctor has heard everything and this room is private and anything you say and hear is privileged information.” 11 Physician “I don't burden those things on Dr. [PCP]… . He has his agenda. I have my agenda… . Time is not really long … I think at most 15 minutes. By the time [we] greet each other 5 minutes of that is gone. I never had a chance to tell him [PCP] all I told you because we just don't have that kind of time.” 12 Patient “Well, even today because it was only 15 minutes I did not ask about my [concern that] … I can't lift my arm that high and I need physical therapy.” 13 Patient “Well, depressed. I'm depressed as hell. I mean, really bad, lately. And… [Interviewer: Do you tell [PCP] about that?] No. I didn't tell her that. [Interviewer: Okay. How come?] I don't know.” 14 Physician “I think we have too many patients … all of us who are actually doing this work are going to be completely stressed out. People are sicker, they're living longer, they're pushed out of the hospital sooner and there's this kind of sense that it all falls down on the primary care doctor.” 15 Patient “One of the things that is so great about him is that he has never told me that he is too busy to talk to me. If it takes 45 minutes, then he will.” 16 Patient “I am aware of his schedule, but sometimes, just between you and me, I'll creep over into the next poor soul's minutes slightly. I'm aware of that, but if we're into a discussion and I'm getting the information I need …” 17 Physician “When I started, we had paper charts to take notes in, and so you'd see a patient, you'd be writing their note while you talk to them, which isn't very distracting to you or the patient and then you would hand them their check-out stuff and you were done. So I worked at work and I lived at home, and then through the years, now everything has to be on the EMR, that takes longer, everybody knows it takes longer.” 18 Physician “I feel strongly that the computer ought not to be a focus point during the interaction, so I have my notes in advance and one of the reasons I have always done that is so I don't look things up on the computer … I'm not saying, “Well let's find out what the cardiologist said when they saw you, and let's check to see if you're due for any immunizations,” I've done all that in advance, so I don't have to interact with the computer for that purpose, and I don't type things while I'm talking to people.” 19 Patient “They [other doctors] have to go into the electronic medical record and he does a really good job of not doing that when the patient's in the room. You know, the physicians have to work on some of that themselves and some of them will do it right when the patient's sitting there because of time constraints, but he does his all on his own time. He told me that he feels it's really important to have eye contact and have a regular conversation with the patient.” 20 Physician “It took forever to get to [her request]: ‘I just need you to write a letter and then they waive the admission fee… .' And I was like, ‘Gosh, if you could have just said that I would have been typing the letter while you were talking about things.’ 21 Physician “There's always the, when you think you're done and the hand on the door, ‘By the way, you know, I've had chest pain or I'm really depressed.’ Those are usually the ones they sometimes are reluctant to talk about but really want to talk about … there's always a surprise.” EMR, electronic medical record; PCP, primary care physician.
Tips from physicians to patients: 1) Bring a thoughtful list of your concerns and questions to your visit.
2) Try to prioritize your list and bring up the issues most urgent or important for you at the beginning of the visit.
3) Do not be shy, your doctor has heard everything before and they are here to help you. Try not to save issues that you may perceive as embarrassing or scary for the end of the visit.
4) Ask any questions that you have during your visit.
5) If you have any remaining concerns when the visit is closing, make a plan with your physician for how to address them later.
Tips from patients to physicians: 1) Ask for the patients' agenda early.
2) Explain how many items and the types of concerns that can be covered during a typical visit.
3) Make a plan for concerns that remain after the visit.
4) Leave sufficient space for patients to raise sensitive or private concerns.
5) Be clear about when issues feel “unactionable” or explored as much as possible.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Filling a gap in safety metrics: development of a patient-centred framework to identify and categorise patient-reported breakdowns related to the diagnostic process in ambulatory care
- Patient-Defined Visit Priorities in Primary Care: Psychosocial Versus Medically-Related Concerns
- Yonder: Patient complaints, after-visit summaries, rectal bleeding, and the doorknob phenomenon
- Interventions Must Be Realistic to Be Useful and Completed in Family Medicine