
Abstract
Background: Primary care providers (PCPs) are often challenged to address multiple patient concerns during time-limited visits. The need for PCPs to limit the number of issues addressed may have a negative impact on discussion of patient-defined visit priorities.
Methods: Using data from a recent clinical trial (Aligning Patients and Providers, ClinicalTrials.gov: NCT02707146), we examined the association between patient-defined visit priorities and subsequent provider actions taken during and after the visit. We tested the hypothesis that psychosocial concerns (eg, stress, anxiety, caregiving demands) are less likely to be addressed than traditional medical concerns.
Results: We analyzed 147 patient-defined visit priorities submitted just before the visit by 109 patients (mean age, 59.0 ± 12.7 years; including 73.4% women, 47.7% non-White race/ethnicity). Nearly one quarter of patient-defined visit priorities were related to psychosocial concerns (35/147; 23.8%). In models adjusting for age, gender, race/ethnicity, and familiarity with PCP, patients' psychosocial priorities were significantly less likely than medical priorities to be addressed during the visit (63% vs. 88%; adjusted odds ratio [aOR], 0.16; 95% CI, 0.06 to 0.41; P < .001), to receive clinical action (51% vs. 82%; aOR, 0.15; 95% CI, 0.06 to 0.38; P < .001), or to receive post visit information from the primary care doctor (17% vs. 32%; aOR, 0.39; 95% CI, 0.14 to 1.08; P = .07).
Conclusions: Patient-defined psychosocial priorities are less likely to be addressed during (or immediately after) primary care visits compared with patient-defined medical priorities.
- Communication
- Mental Health
- Patient-Centered Care
- Physician-Patient Relations
- Primary Health Care
- Primary Care Physicians
- Social Determinants of Health
Patients frequently experience psychosocial concerns such as financial or housing insecurity, caregiving or work-related stress, and mental health symptoms including anxiety or subclinical depression that can significantly interfere with their quality of life.1,2 Prior observational studies have suggested that psychosocial issues are less frequently addressed during primary care visits due to time constraints, the more complex nature of these issues, and lack of available resources.3⇓⇓–6 This failure to address the full spectrum of patient needs is problematic given that factors such as financial concerns, stress, and anxiety have been shown to negatively impact health outcomes, leading to lower functional status, earlier mortality, increased rates of medical complications, and higher incidence of acute hospitalization.7⇓⇓⇓⇓–12
Primary care providers (PCPs) must balance management of acute and chronic medical conditions while also addressing an increasing number of quality and guideline-based metrics.13⇓–15 Multiple competing demands and limited time during primary care visits represent significant barriers to successful patient-provider communication and collaboration.16⇓–18 With the aging of the general population, patients present for care with a rising number of concurrent chronic medical conditions.19,20 As a result, visit agendas may be largely defined by PCPs, and patients may not always have the opportunity to voice their concerns and may leave with unmet needs.21,22
Because primary care visits typically involve discussion of multiple different concerns (eg, patient symptoms, test results, behavior changes, recommended screenings), understanding the relationship between patient-defined priorities and subsequent provider actions can provide insight into how agendas are set during visits. We had the unique opportunity to examine patient-defined visit priorities among a group of primary care patients participating in a multi-site, randomized clinical trial. In this Aligning Patients and Providers trial, patients in the intervention arm were guided to identify their top 1 or 2 visit priorities in the waiting room just before their primary care visit using a “Visit Planner” tool.23 Patients received a article print-out listing their top visit priorities then proceeded to their visit. For this current report, we examine the relationship between types of patient-defined visit priorities and corresponding clinical actions arising from the visit. We tested the hypothesis that providers would be less likely to address patient-identified psychosocial concerns compared with medically related patient priorities.
Methods
Setting
Our analysis was conducted using data from the Aligning Patients and Providers study (APP; ClinicalTrials.gov: NCT02707146), a randomized controlled trial conducted within Kaiser Permanente Northern California (KPNC). KPNC is a nonprofit, integrated health care delivery system that provides care for over 4.1 million members throughout Northern California.
Full details of the trial have been published elsewhere.24 Briefly, primary care physicians were recruited for the clinical trial between June 2015 and February 2016 from 7 primary care practices. Patient clinical trial eligibility was based on having a current gap in evidence-based primary care, defined as being due for preventive cancer screening (breast, cervical, and colorectal); having suboptimal medication adherence (for treatment of diabetes, hypertension, or dyslipidemia); being a current smoker; or having suboptimal chronic disease control (defined as elevated Hemoglobin A1c [HbA1c], systolic blood pressure, or Low-Density Lipoprotein [LDL]-cholesterol; or being overdue for osteoporosis treatment). This broad array of potential inclusion criteria resulted in a fairly representative cohort of general primary care patients. Patients with a diagnosis of dementia, psychosis, or other medical conditions which could impair participation were excluded from the study. Patients were initially contacted by phone for participation in the study after they had scheduled an appointment. During this phone call, the research assistant arranged to meet the patient in the waiting room before the visit, where written informed consent was obtained. The study was approved by the institutional review board of the Kaiser Foundation Research Institute.
Patient-Identified Visit Priorities
Our current analysis focuses on data collected from patients enrolled in the intervention arm of the APP trial. Using a tablet-based tool in the waiting room (“Visit Planner”), these patients viewed a 30-second video clip on the importance of mentioning their priorities at the beginning of the visit and then selected their top 1 or 2 visit priorities from a list of 6 prespecified categories. Within each category, patients could further select from up to 5 subcategories and/or add free text to further clarify the nature of the priority (Table 1). After making their choices, patients received a 1-page article print-out with their selections from research assistant before going in to the examination room. The patient-priorities were not entered by staff into the medical record.
Visit Priority Options (6 Main Categories and Associated Subcategories) and their Corresponding Psychosocial Versus Medical Designations for This Study
For our analysis, responses were grouped into 2 mutually exclusive categories of psychosocial versus medical priorities based on patient category selection and any accompanying free text responses. Priorities were considered psychosocial if patients identified: 1) ‘I am feeling anxious or depressed,’ 2) ‘Drug or alcohol concerns,’ 3) ‘Caregiving issues,’ 4) ‘Family concerns,’ or 5) ‘Stress at home or work.’ Free text responses with specific mention of depression, anxiety, stress, family concerns, or substance use were also categorized as psychosocial priorities. Priorities where patients indicated specific medical concerns (eg, ‘back pain,’ ‘cough,’ ‘diabetes’) were categorized as medical priorities. Priorities that could not be categorized as either psychosocial or medically-related (eg, ‘New problem’ or ‘Old problem’ without any explanatory text) were excluded from our analysis.
Study Outcomes
We used structured electronic chart review of visit progress notes, after-visit summaries, orders placed during the visit, specialty referrals, and postvisit email messages between patient and provider to determine whether the provider addressed the patient's visit priorities.
The main outcome of interest was concordance between patient-defined priority and provider response. Concordance was examined in 3 domains: 1) provider documentation of the patient-defined priority in the progress note or patient problem list, 2) evidence of action or follow up through relevant referral, documentation of in-office counseling, ordering of relevant lab tests, imaging studies, or therapeutics, and 3) provision of information about the patient-defined priority through a primary care after-visit summary or a secure message to the patient with specific reference to the patient priority within 72 hours of the visit.
Statistical Analyses
We examined patient-provider concordance comparing psychosocial versus medically related patient priorities using χ2 tests with a significance level of 0.05 and 2-sided hypothesis testing. In secondary analyses, we also examined patient-provider concordance stratified by history of patient mental health disorder and by primary care physician gender. Mental health disorders were defined by International Classification of Diseases (ICD) 10 diagnosis (anxiety disorder, major depressive disorder, post-traumatic stress disorder, Attention-Deficit/Hyperactivity Disorder, bipolar disorder type 1 or 2, or addiction to alcohol or illicit substances).
We constructed logistic regression models (SAS GENMOD) to examine odds of concordance by priority type (psychosocial vs medically-related) after adjusting for potential confounding variables including patient and provider gender, patient age and race, and patient-PCP familiarity defined as new to PCP (< 18 months) versus established relationship (≥ 18 months). We applied generalized estimating equations to adjust for the nonindependence of multiple priorities for some patients. All analyses were performed using (SAS version 9.3, SAS Institute, Cary NC).
Results
Cohort Characteristics
Our cohort included 109 patients with self-identified psychosocial or medical visit priorities. Mean age was 59.0 (± 12.7) years and 73.4% were women. A slight majority of patients identified as non-Hispanic white (52.3%). Patients were taking 2.5 (± 2.5) medications. Most patients received care from a female primary care physician (74.3%) and most patients had the same gender as their physician (71.5% gender concordance). We found no statistically significant baseline differences between patients with any psychosocial concerns compared with patients with only medical concerns (Table 2).
Characteristic of Patients with and without any Psychosocial Visit Priorities
Patients listed a total of 147 unique priorities which were included in our analysis. Most patients identified a single visit priority (77/109; 71%). Nearly one quarter of all priorities (35/147; 23.8%) were categorized as psychosocial concerns. Of these, the most common were anxiety and depression (54%) and general psychosocial stress (43%). The most frequently patient-identified medical priorities were related to musculoskeletal (26%) or cardiovascular (12%) concerns.
Patient-Provider Concordance by type of Patient Visit Priority
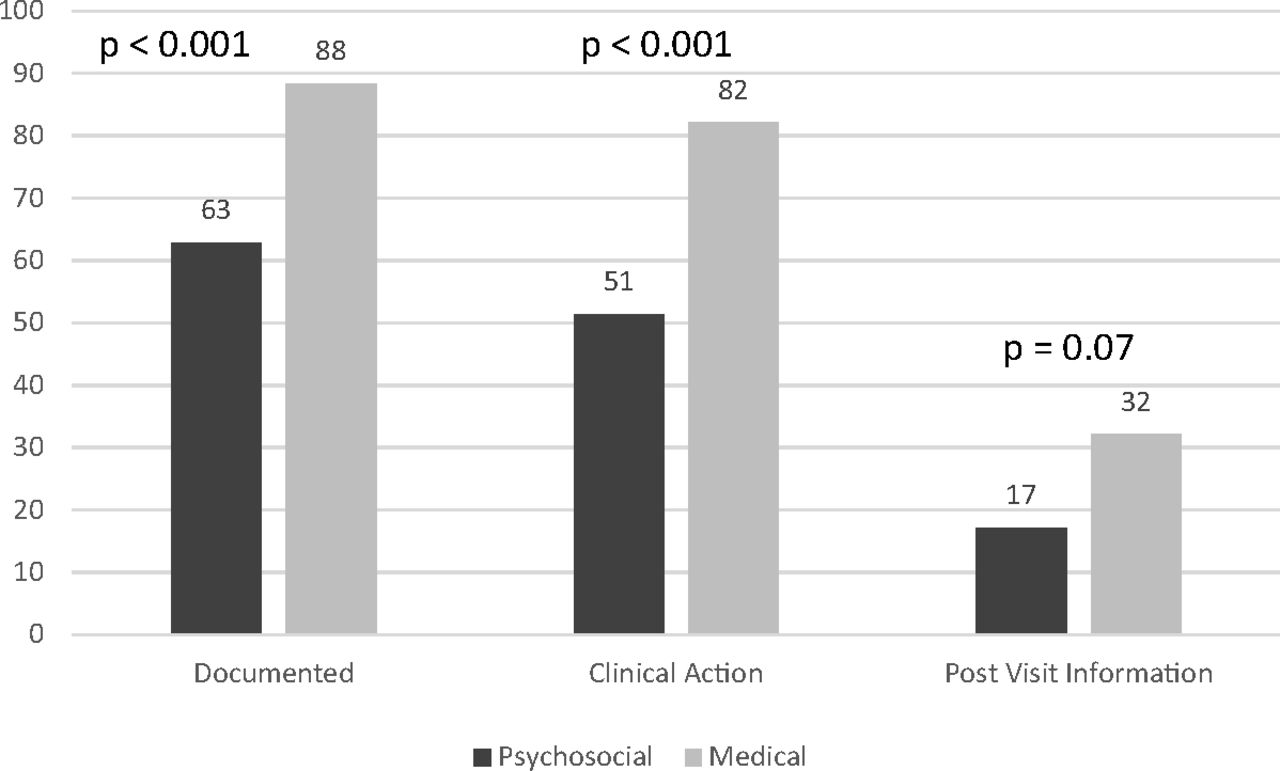
Psychosocial priorities were less likely to be addressed by the primary care provider compared with medically related priorities. More specifically, psychosocial priorities were less often documented in the chart (62.9% vs. 88.4%; P < .005), less often subject to clinical action or follow-up (51.4% vs. 82.1%; P < .005), and less often included in post visit information from the primary care doctor (17.1% vs. 32.1%; P = .09) compared with medically related health priorities (Figure 1). Results remained similar when stratified by history of mental health disorder, provider gender, or whether patient and provider were of the same gender.

Bars represent proportion of psychosocial (dark) or medically-related (light) patient-defined visit priorities that were addressed by provider, either through documentation of the patient-defined visit priority in the chart (62.9% vs 88.4%, p < .005), taking clinical action (51.4% vs. 82.1%, p < .005), or following up with the patient after the visit with related information (17.1% vs 32.1%, p = 0.09).
These concordance differences between psychosocial and medically related priorities remained after adjusting for patient and provider gender, age, patient race, history of mental health disorder, and familiarity between patient and provider. Psychosocial priorities were less likely to be addressed by the primary care provider (62% vs. 88%; adjusted odds ratio [aOR], 0.16; 95% CI, 0.06 to 0.41; P < .001), less likely to receive clinical action (54% vs. 82%; aOR, 0.15; 95% CI, 0.06 to 0.38; P < .001), and less likely to receive post visit information from the primary care doctor (17% vs. 32%; aOR, 0.39; 95% CI, 0.14 to 1.08; P = .07) compared with medically related priorities. Of the other variables considered in our models, only higher patient age was independently associated with lower odds of a patient-identified priority being addressed by the primary care provider (76% vs. 91% for age 60 to 80 vs. 30 to 59 years; aOR, 0.31; 95% CI, 0.11 to 0.82; P < .02).
Conclusions
Psychosocial concerns are a frequent visit priority for patients in primary care. Prior research has suggested that these concerns may receive less attention than medically defined problems during primary care visits.25,26 In prior studies, identification of psychosocial concerns was by physicians rather than by patients. We had the unique opportunity to examine primary care interactions based on patient-defined visit priorities. These priorities were elicited in the waiting room as part of the APP clinical trial, an intervention that included a brief (30-second) video clip encouraging patients to bring up their visit priorities at the beginning of the visit and an easy process for patients to select their priorities, which were then printed out for them before they entered the examination room.
Through review of these patient-identified priorities during primary care visits and the outcomes of these visits, we found that patient-defined psychosocial priorities were markedly less likely to be addressed by primary care physicians than medically related priorities. Our results extend prior research that providers are more likely to address medical concerns as opposed to psychosocial priorities3⇓–5,27⇓–29 by demonstrating that this disparity exists even when patients themselves have identified these concerns as top visit priorities.
There are likely several different contributors to this disparity between how psychosocial and medically related priorities are addressed in primary care. Providers receive little training in how to talk to patients about concerns such as food or housing insecurity, financial concerns, or caregiver burnout or fatigue. For these reasons, some physicians may perceive medical concerns as more appropriate targets for their care. Providers may also be less likely to initiate discussion regarding more complex psychosocial issues, especially among patients with chronic conditions, as they tend to have less concrete solutions.30 Providers may also lack the necessary resources (eg, available mental health consultants or social workers who can help with financial issues) to direct toward patients with nonmedical needs. These psychosocial needs are also generally less amenable to actions such as ordering tests, giving lifestyle advice, and prescribing medicines with which providers are generally most comfortable.
One strength of our analytic approach was to examine multiple domains of provider action: formal documentation, different tangible clinical actions, and follow-up contact with the patient. It is perhaps not surprising that patient-prioritized psychosocial issues were less likely to be documented during the visit, as providers may limit documentation to details that support billing requirements. To the extent that the psychosocial priorities raised by patients may be helpful for other clinicians reading the chart in future encounters, our results suggest that this may be a missed opportunity. Indeed, evidence has shown that patient-centered care—which would include addressing patient-defined psychosocial needs—can improve care and reduce costs.31
A secondary finding from our analysis was the independent negative association of patient age with patient-provider concordance on visit priorities. This can likely be explained by the fact that older patients have a larger number of chronic medical conditions32 and providers may be more strained for time to address patient priorities.33 Given the ageing of the primary care population, this finding may have important implications for growing the need to improve awareness of psychosocial issues in older patients. Current literature suggests that to circumvent this issue, elderly patients may benefit from family member or companion presence during primary care visits to help more effectively advocate for the patient's concerns.34
Prior research has also shown that female physicians tend to be more patient-centered than male physicians and are more likely to address patient concerns, particularly when discussing psychosocial matters.35 In contrast to these prior studies, we found no correlation between gender of primary care provider and concordance with patient-defined priorities. This association, however, has only been previously described in settings where providers had to directly elicit patient priorities, rather than receiving them from the patient, and may speak more to communication style discrepancies between genders rather than patients being forthcoming with their priorities.36
Several limitations of our study deserve mention. Our concordance assessment was based on documented priorities and actions and thus does not capture conversations that may have been conducted during the visit. Indeed, although patients were coached to communicate their visit priorities at the beginning of the visit, we cannot be sure that patients voiced these priorities. In addition, current electronic health record (EHR) systems are typically better designed to facilitate coding of medical rather than psychosocial concerns. Nonetheless, the disparities in documentation, clinical actions, and postvisit messaging captured through structured chart review all support our conclusion that psychosocial issues are less likely to be meaningfully addressed in primary care than medically related ones. In addition, we were unable to capture whether more pressing clinical matters such as an acute medical problem superseded patient priorities, thus making concordance less likely. Our tabulation of priorities from our study participants may not be generalizable to other populations, both because all KPNC patients are insured and because participation in the APP clinical trial may have facilitated recognition of psychosocial priorities. Finally, due to the relatively small sample sizes, we were unable to examine concordance by specific concerns within our 2 mutually exclusive categories.
Our results highlight the difficulties that patients face in having psychosocial needs addressed during primary care visits. Based on prior studies, we speculate that the multitude of competing clinical demands and limited resources for psychosocial care may be contributors to the results we found. Although we could not address this question directly in our analysis, our results suggest potential solutions to this problem may include improved provider training and increased care coordination with other primary care team members. Indeed, many primary care practices have begun to include a behavioral medicine specialist on the care team to help support patients with psychosocial issues. Future efforts to improve care should focus not only on helping physicians discuss patient priorities at the outset of the visit to help maximize visit efficiency and improve patient experience,37,38 but also to help bolster clinic- and community-based resources to provide psychosocial support to patients.39,40
Notes
This article was externally peer reviewed.
Funding: Research reported in this publication was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (CDR-1403-11992) and National Institute of Diabetes and Kidney Diseases (NIDDK K24DK109114).
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/32/4/513.full.
- Received for publication December 19, 2018.
- Revision received March 26, 2019.
- Accepted for publication March 31, 2019.




{kind=link}