
Abstract
Background: Due to the COVID-19 pandemic, a “state of emergency” was declared in North Carolina on March 10, 2020. Subsequent “stay-at-home” (SAH) orders restricted activities including use of fitness facilities, and teleworking was encouraged. This study investigates metabolic effects of these changes in activity level.
Methods: This retrospective prepost study included adults diagnosed with type 2 diabetes mellitus and hypertension with hemoglobin A1c (HbA1c), weight, and blood pressure (BP) measurements for 3 time periods: 3/10/2019-9/9/2019 (“pre-SAH”), 3/10/2020-9/9/2020 (“during SAH”), and 3/10/2021-9/9/2021 (“post-SAH”). The primary outcome was change in HbA1c pre-SAH to during SAH and during SAH to post-SAH. Secondary outcomes were changes in weight, systolic BP (SBP), and diastolic BP (DBP) over the same periods. Exploratory outcomes included health care utilization. Paired t test compared outcomes between time periods using Bonferroni-adjusted α of 0.025 for significance.
Results: Analysis included 301 participants with an average age of 69.8 years. HbA1c, SBP, and DBP trended up from pre-SAH to during SAH and then decreased post-SAH with a significant change only for DBP from during SAH to post-SAH (74.2 mmHg to 73.6 mmHg, P < .001). Weight trended down across the 3 study periods. In-office visits significantly decreased from pre-SAH to during SAH, and telehealth visits significantly decreased from during SAH to post-SAH (both P < .001).
Conclusions: With the exception of DBP, findings reveal consistency in HbA1c, weight, and BP across time periods before, during, and after COVID-19 SAH orders in North Carolina.
Background
In North Carolina, stay-at-home (SAH) orders due to the (COVID-19) pandemic were enacted on March 10, 2020, leaving residents inside their homes and adapting to new routines and lifestyles. SAH orders also promoted telehealth rather than in-office health care visits to reduce viral spread. SAH orders slowly lifted with facilities (ie, gyms, restaurants) reopening at 30% capacity on September 4, 2020, and SAH orders were fully lifted in February 2021.1 Beyond the detrimental impact of the novel coronavirus itself, general well-being was also negatively affected. A survey-based study showed that during SAH orders, fried food and sugar-sweetened beverage consumption rose, with a concomitant increase in anxiety/stress in overweight/obese people.2 Self-reported studies of dietary intake at the beginning of the pandemic showed a reduction in fresh fruits and vegetables followed by an increase in both red or processed meats and starchy vegetables.3
It is not fully understood how SAH orders affected metabolic parameters. A single-center observational study showed that 26% of people with previously controlled diabetes had an increase in hemoglobin A1c (HbA1c) of at least 0.3%.4 Pandemic-related studies also showed an increase in sedentary time and decrease in exercise time.2 These behaviors trigger disease progression and decline in metabolic health parameters, including blood pressure (BP), HbA1c, and cholesterol panels. Dysregulation of these parameters increases the risk of cerebrovascular accident, myocardial infarction, and progression of chronic kidney disease.5,6
The purpose of this study was to evaluate the change in glycemic control, weight, and BP before, during, and after SAH orders were issued in North Carolina. Given the risks of progressing metabolic diseases, this retrospective review hoped to outline some of the long-term impacts of the COVID-19 pandemic on people with common chronic diseases.
Methods
This retrospective prepost study was conducted by reviewing electronic medical records from 2 primary care practices, both in urban settings and not associated with an academic institution. Included participants were adults (≥18 years) with diagnoses of type 2 diabetes mellitus and hypertension who had HbA1c, weight, and BP measurements for the 3 time periods outlined below. Pregnant women were excluded. The first time period, “pre-SAH,” was March 10, 2019, to September 9, 2019. “During SAH” was March 10, 2020, to September 9, 2020. “Post-SAH” was March 10, 2021, to September 9, 2021. These time periods were chosen to allow adequate time for meaningful change while also limiting seasonal variation. HbA1c, weight, and BP were recorded as the last value within the given time period. The primary outcome was change in HbA1c from pre-SAH to during SAH and from during SAH to post-SAH. Secondary outcomes were changes in weight, systolic BP (SBP), and diastolic BP (DBP) over the same periods. Exploratory outcomes included health care utilization during the 3 periods. The null hypothesis was that no change would be seen in metabolic parameters across the time periods. Outcomes were compared pre-SAH to during SAH and from during SAH to post-SAH periods using paired t test. Due to multiple comparisons testing, a Bonferroni-adjusted α of 0.025 was set for statistical significance. This study was approved by the local Institutional Review Board.
Results
Data for 301 participants were analyzed. The mean age was 69.8 years, 57.8% were female, 59.8% identified as Non-Hispanic White, and 67.4% were obese/overweight (Table 1).
Baseline Characteristics
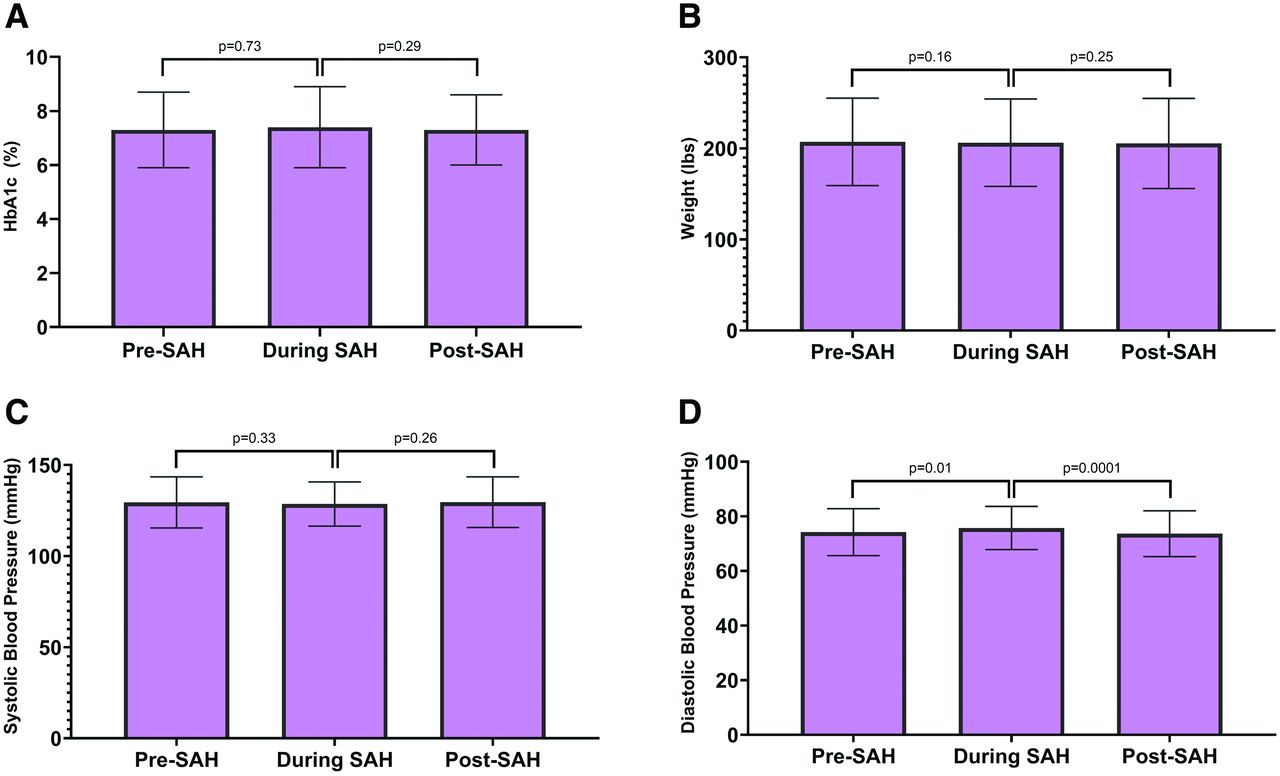
HbA1c trended upward from 7.3% pre-SAH to 7.4% during SAH (P = .73) and then back to 7.3% post-SAH (P = .29) (Figure 1A). There was a nonsignificant decrease in weight across the 3 study periods (Figure 1B). SBP trended down from 129.5 mmHg pre-SAH to 128.6 mmHg during SAH (P = .33) and then up to 129.6 mmHg post-SAH (P = .26) (Figure 1C). DBP increased from 74.2 mmHg pre-SAH to 75.7 mmHg during SAH (P = .01) and then decreased to 73.6 mmHg post-SAH (P < .001) (Figure 1D).

Changes in metabolic parameters. Abbreviations: During SAH, during stay-at-home defined as 3/10/2020-9/9/2020; HbA1c, hemoglobin A1c; Pre-SAH, pre stay-at-home defined as 3/10/2019-9/9/2019; Post-SAH, post stay-at-home defined as 3/10/2021-9/9/2021.
Before SAH orders, in-office visits were the primary mode for accessing care (mean visits 2.7 ± 2.1), while telehealth was introduced during SAH (mean visits 0.3 ± 0.7). There was a statistically significant difference between in-office visits pre-SAH to during SAH (2.7 to 2.2, P < .001) as well as for telehealth visits during SAH to post-SAH (0.3 to 0.1, P < .001).
Discussion
This retrospective prepost study assessed changes in HbA1c, weight, and BP at 2 primary care clinics in North Carolina. Findings reveal consistency in HbA1c, weight, and SBP across 3 6-month time periods over a 3-year span before, during, and after SAH orders. However, there were statistically significant changes in DBP across the 3 periods.
HbA1c was relatively stable with a nonsignificant increase of 0.1% during SAH orders followed by a decrease back to baseline. As HbA1c is based on the approximate 3-month lifespan of red blood cells and the last value within a given time period was recorded for each participant (ie, all values may not have been after at least 3 months since the start of that time period), it is possible that the full effect of changes related to SAH orders may not have been seen. On the other hand, many people may have experienced increased flexibility in work or social calendars during SAH orders, which could have allowed more time for physical activity, thus keeping metabolic parameters in check. Similarly, a nonsignificant rise in HbA1c from 6.6% to 6.8% was seen in another study investigating changes in metabolic parameters before versus after the 8-week COVID-19 lockdown in Italy in people with well-controlled type 2 diabetes.4
Interestingly, weight trended downward over the 3 study periods. As the average age of the study population was just under 70 years old, potential reasons for this could be muscle wasting due to decrease in exercise and fewer meals eaten out due to fear of being exposed to the virus. A study investigating change in body mass index (BMI) and physical activity in older adults in Italy found no major changes in BMI but a significant decline in physical activity in this age-group.7 Another study collected questionnaires from Dutch older adults assessing nutrition and physical activity and found that older age was associated with eating less and losing weight.8 Although our study did not collect data on diet or physical activity, results from these publications present possible explanations for body weight trending down.
Although no significant changes were observed with SBP over the study period, DBP increased significantly from pre-SAH to during SAH and then decreased significantly post-SAH. One study compared the change in BP during the pandemic to the previous year and showed an increase in both SBP and DBP (1.10 to 2.50 mmHg and 0.14 to 0.53 mmHg, respectively).9 Increases in BP could be related to stress precipitated by the COVID-19 pandemic, increased sodium and alcohol intake, and decreased activity.10 Another study demonstrated worsening SBP and DBP during the first 8 months of the COVID-19 pandemic among individuals with hypertension; however, once other solutions such as telemedicine were provided, BP began to stabilize.11 These findings provide a possible explanation for the decrease in DBP found in our study from pre-SAH to post-SAH as telehealth was implemented.
A statistically significant decrease was observed from pre-SAH to during SAH for in-office health care visits. Although SAH orders did not restrict people from visiting primary care offices, many may have postponed visits or turned to telehealth to avoid public spaces. However, a statistically significant decrease in telehealth from during SAH to post-SAH was found, suggesting that health care utilization began to normalize after SAH orders ended. Telehealth outside of a pandemic setting could be beneficial for persons with barriers to participating in in-office appointments but may not be the preferred option for the population seen at these 2 clinics, particularly with the average age just under 70 years. Reasons for this disinclination from published literature in adults over age 65 include lack of ownership of internet-enabled devices, lack of knowledge of how to use internet-enabled devices, and general discomfort or unwillingness to participate in nontraditional platforms.12
Limitations
This study included predominantly White people, which minimizes the understanding of disease states that disproportionately affect more African American people.13 Moreover, with participants from only 2 health care clinics in a similar geographic location and average age approaching 70 years, further insight could be found in future studies with larger sample sizes and more equally dispersed demographics. In addition, this study is subject to selection bias due to the specificity of the inclusion criteria and may be skewed toward those more engaged in their care versus participants who were excluded due to lack of outcome data. Lastly, historic effect cannot be ruled out and could be contributing to the observed results.
Conclusions
With the exception of DBP, consistency was found in HbA1c, weight, and BP across the pre-, during, and post-SAH time periods. As such, it seems that the population included in this study was generally able to maintain levels of metabolic parameters despite limited access to fitness facilities and rising use of telehealth, which may support the use of telehealth as a viable alternative to in-person medical encounters.
Acknowledgments
Authors would like to acknowledge contributions from Jaidyn Bentley, PharmD and Briana Jackson, PharmD.
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict if interest: The authors declare that they have no conflict of interest.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication May 30, 2023.
- Revision received August 21, 2023.
- Accepted for publication August 29, 2023.




{kind=link}