
Abstract
Introduction: Colorectal cancer (CRC) is the second leading cause of cancer death in the United States. While patient-reported barriers have been previously described, few studies have analyzed how patients’ social needs affect screening rates.
Methods: This cross-sectional study includes 3,443 Kaiser Permanente (KP) patients ages 50 to 75 years who completed the 2020 KP National Social Needs Survey. Five social needs categories were assessed: “Financial Strain,” “Housing Instability,” “Transportation Issues,” “Social Isolation,” and “Food Insecurity.” Being up to date on CRC screening was determined from patients’ electronic health records, defined as meeting Health care Effectiveness Data and Information (HEDIS) criteria for screening. We used multivariable analyses to explore associations between social needs and completion of colorectal cancer screening in 2020, adjusting for demographic factors.
Results: Among the survey respondents, 2,805 (81.5%) were up to date on their colorectal cancer screening. Patients were less likely to be screened if they had severe financial strain (OR 2.1, 95% CI 1.3–3.4), severe social isolation (OR 1.9, 95% CI 1.2 to 3.2), and severe food insecurity (OR 2.5, 95% CI 1.2–5.3). There was a nonsignificant increase in odds of not being up to date with screening for severe transportation issues (OR 3, 95% CI 0.93–10) and severe housing instability (OR 1.7, 95% CI 0.93–3).
Conclusion: Even within a fully insured population with high screening rates, respondents with financial strain, social isolation, and food insecurity had lower odds of being up to date with CRC screening. Future efforts should assess how addressing patients’ social needs could lead to increased CRC screening rates.
Introduction
Colorectal Cancer (CRC) is the second leading cause of cancer death for both men and women in the United States, and incidence of cancer in individuals ages 40 to 49 has been increasing.1 Despite recent COVID-19 related declines in cancer screening, CRC screening rates have been steadily increasing in the United States.2 In 2020, 70% of adults aged 50 to 75 were reported to be up to date for CRC screening.3 However, screening rates were noticeably lower among uninsured (37%), low-income (63%), and Hispanic (60%) populations. These rates fall short of targets in the “80% in Every Community” initiative from the National CRC Round Table.4
Because of these gaps in screening, numerous studies have been conducted to identify the factors that could be driving low screening rates.5⇓–7 Systematic reviews of patient-reported barriers to CRC screening cite obstacles to screening such as insurance challenges, concern over the costs of screening, transportation barriers, and lack of social support. Similar social factors have previously been cited as having negative associations with completion of other preventative interventions, such as screening mammography and annual flu immunizations.8,9 As Social Determinants of Health have emerged as some of the principal driving factors to health outcomes, they have become a target for research because of their modifiable nature.10,11 The social needs of transportation, social isolation, financial strain, housing instability, and food insecurity have been repeatedly cited as potential barriers. However, their quantitative effect on screening rates has been under studied. Additional research is needed to determine the association between these social needs and CRC screening uptake and disparities.
As gatekeepers to our health care system with strong understandings of their patient’s circumstances, Primary Care physicians stand at the intersection of social needs and preventative screening, and thus have the ability to play a large role in promoting increased CRC screening. Understanding which social and demographic factors impact completion of CRC screening is necessary for designing population-level interventions to improve screening rates. This study combines data from a patient-reported survey on social needs with respondent’s EHR data. Our aim was to identify the characteristics that most strongly correlate with low screening to inform future efforts within Primary Care to increase CRC screening uptake and decrease screening disparities.
Materials and Methods
This is a cross-sectional study that merged data from the Kaiser Permanente (KP) 2020 Social Needs Network for Evaluation and Translation (SONNET) National Social Needs Survey with Electronic Health Record (EHR), and administrative CRC claims data (collectively referred to as EHR data).12 The primary outcome for this analysis was being up to date with CRC screening in 2020; patients’ self-reported social needs were combined with their demographic factors and CRC screening status to identify predictors of low screening rates. This study was reviewed and approved by the Kaiser Foundation Research Institute as Not Human Subjects Research.
Study Sample
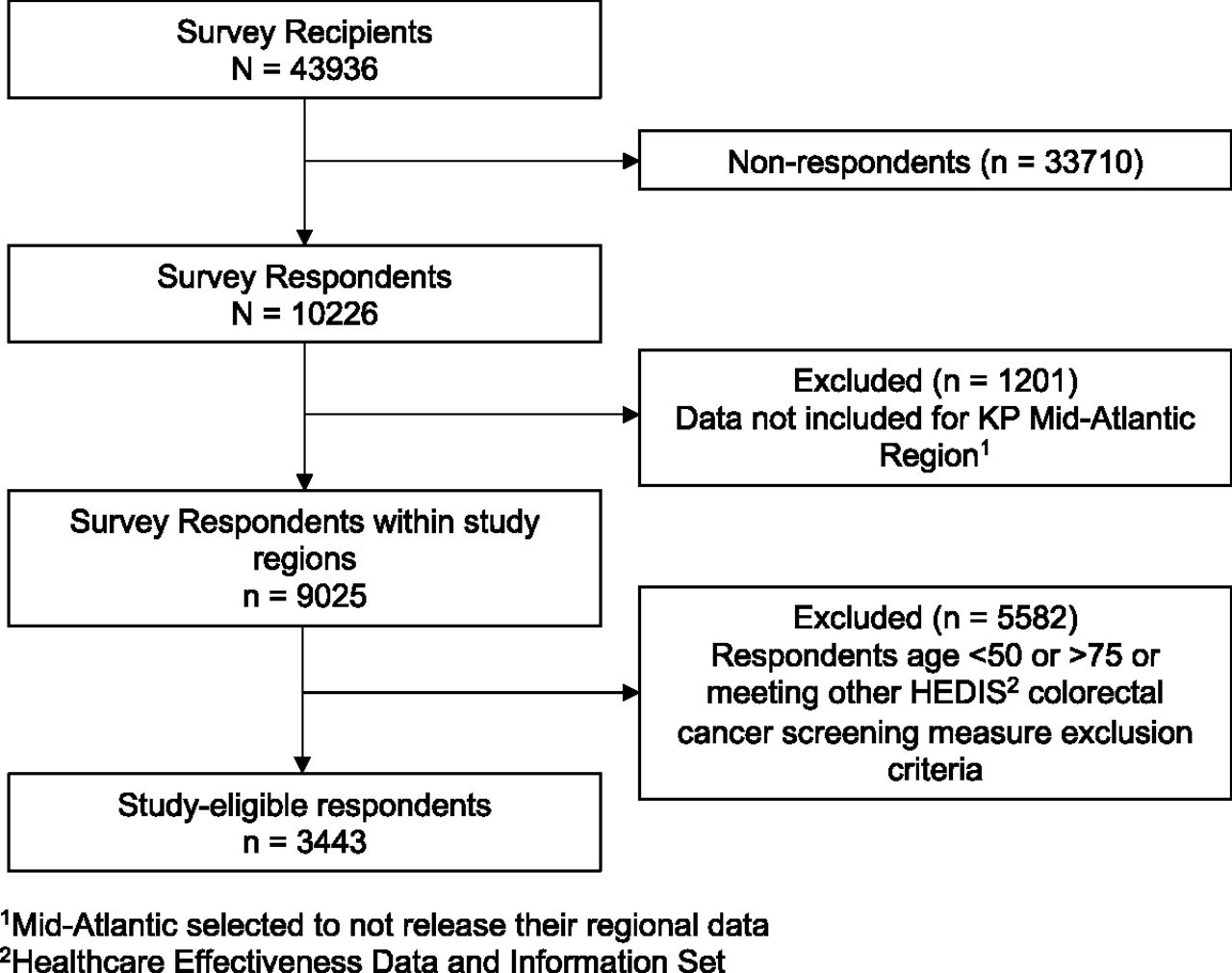
The SONNET Survey was sent out to 43,936 KP members across all 8 KP regions (Colorado, Georgia, Hawaii, Mid-Atlantic, Northern California, Southern California, Northwest, and Washington state). Data were collected between January 2020 and September 2020 with 10,226 members responding (23% response rate). Survey sampling has been described in a previously published study.13
This study used data from 7 of the 8 KP Regions. The Mid-Atlantic region elected to not release their data. Of the 10,226 respondents to the survey, 9,025 were from these regions. The study cohort included survey respondents eligible for CRC screening, ages 50 to 75 years, who met the HEDIS inclusion criteria for continuous enrollment and excluding patients with frailty or advanced illness, resulting in a sample size of 3443 (Figure 1).2 Frailty and advanced illness were defined by ICD-10 and CPT codes, as outlined by the National Committee for Quality Assurance (NCQA).14 Of note, the United States Preventive Services Task Force (USPSTF) had not yet lowered the screening age range from 50 to 45 at the time this survey was conducted. Participants’ characteristics are described in Tables 1 and 2. Thirty-two respondents were excluded from the multivariable model because of missing data.

Study sample.
Patient Demographics by Cancer Screening
Association Between Social Needs and Colorectal Cancer Screening
Main Measures
The primary outcome was being up to date with CRC screening in 2020. Screening requirements could be filled via any HEDIS-approved screening mechanism, including colonoscopy within the past 10 years, fecal occult blood test within the past year, flexible sigmoidoscopy in the past 5 years, CT colonography in the past 5 years, or stool DNA in the past 3 years.
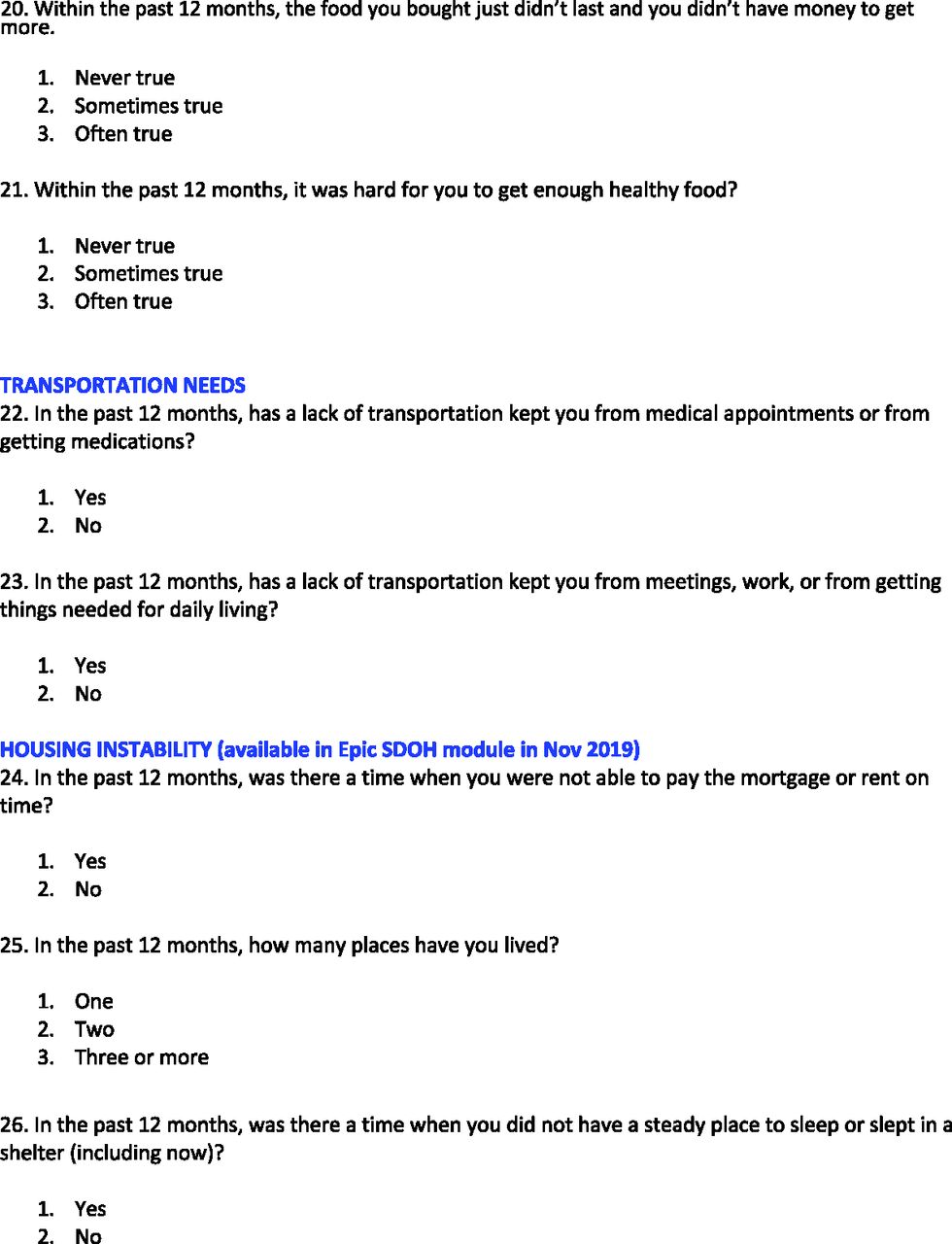
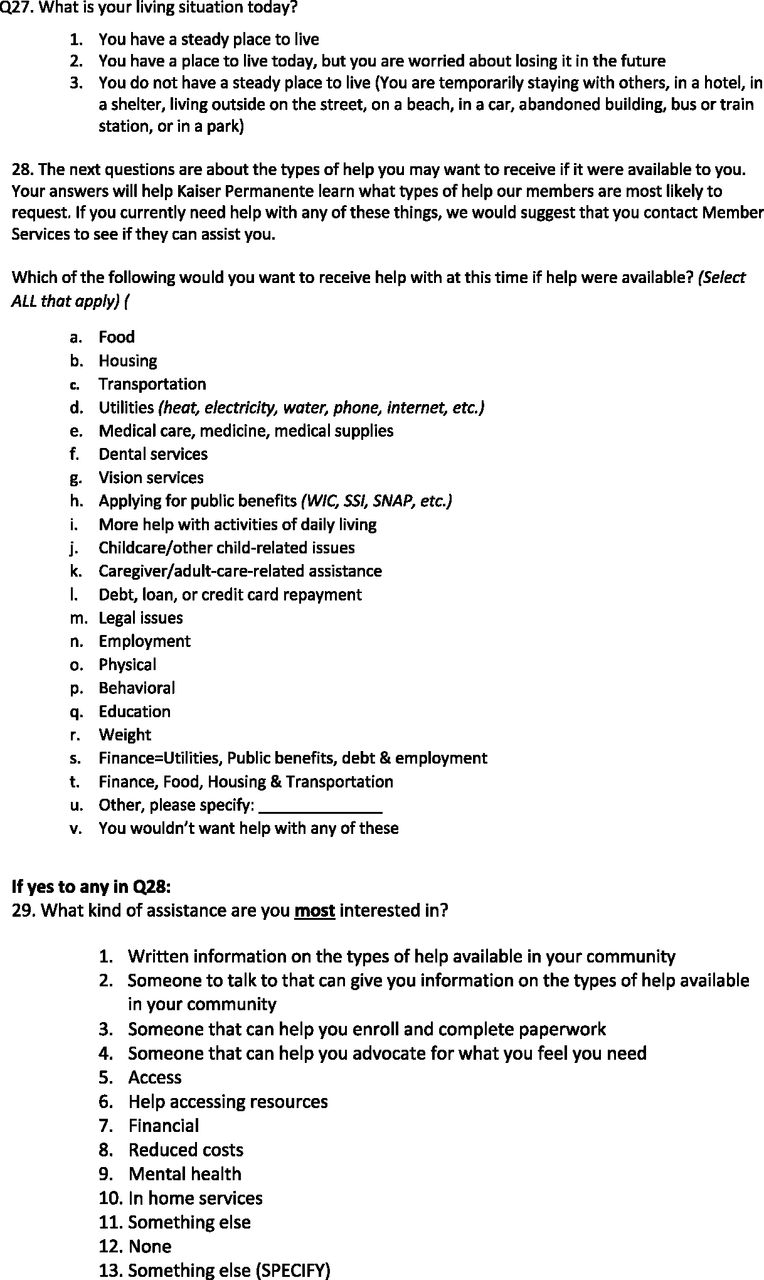
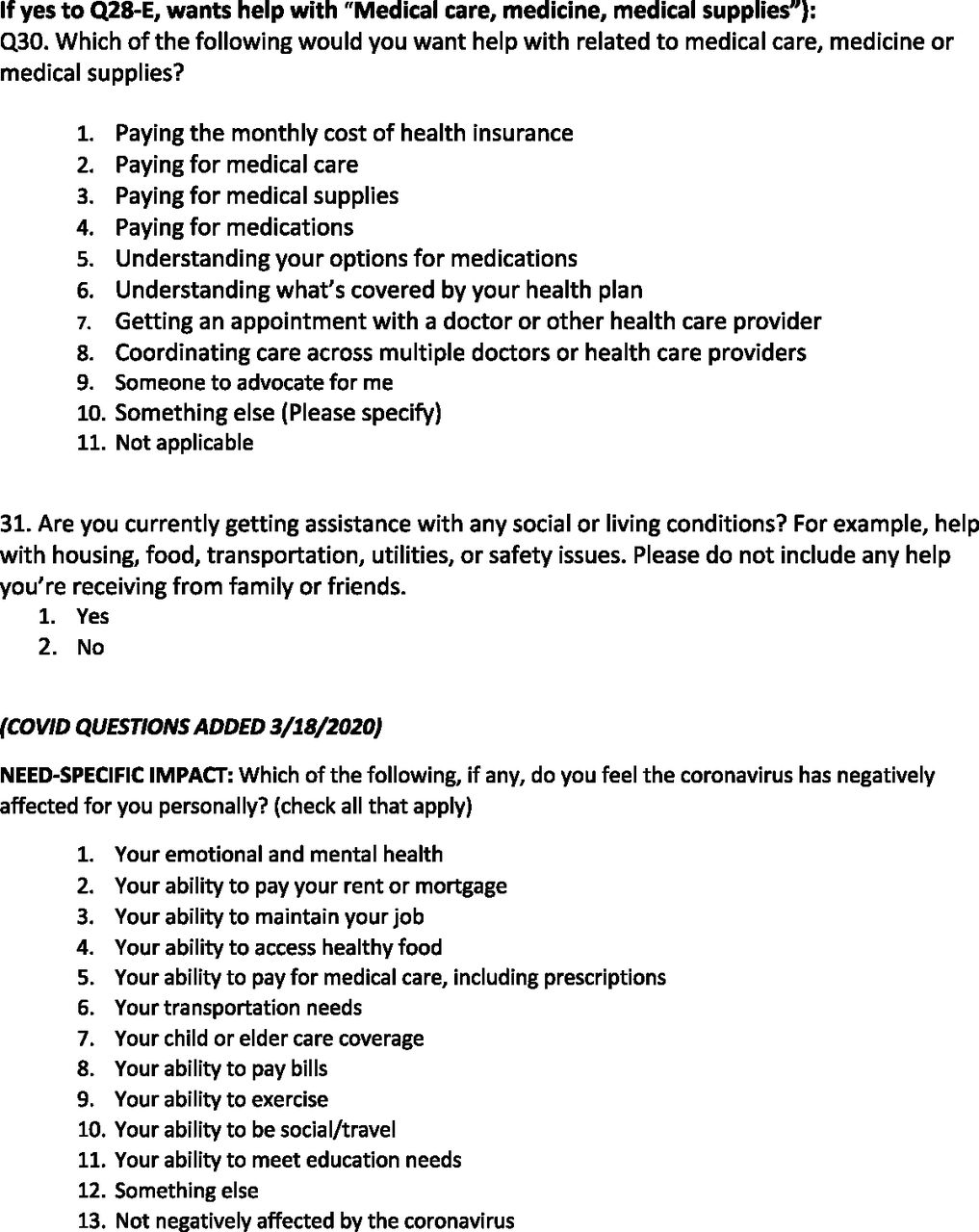
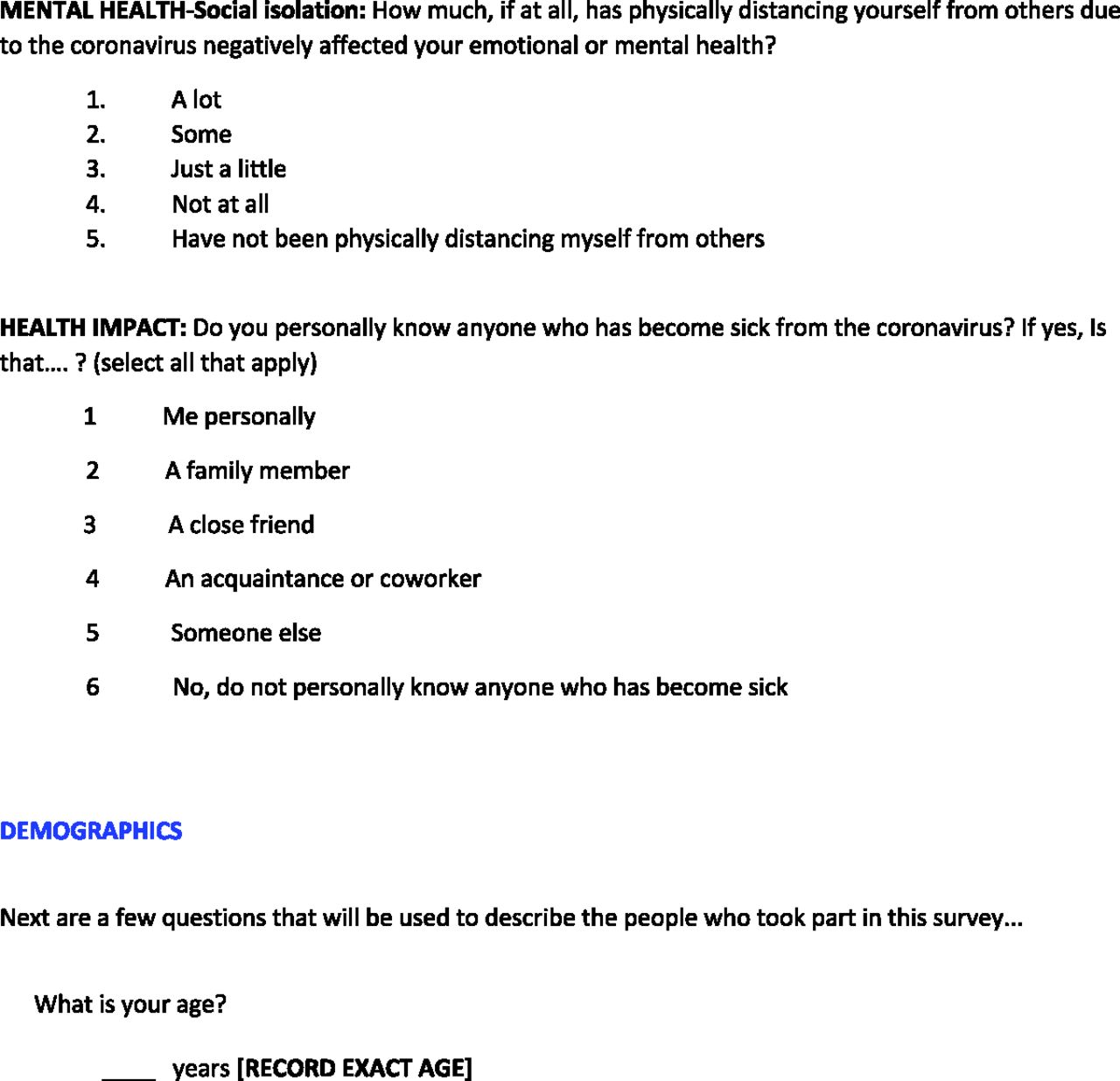
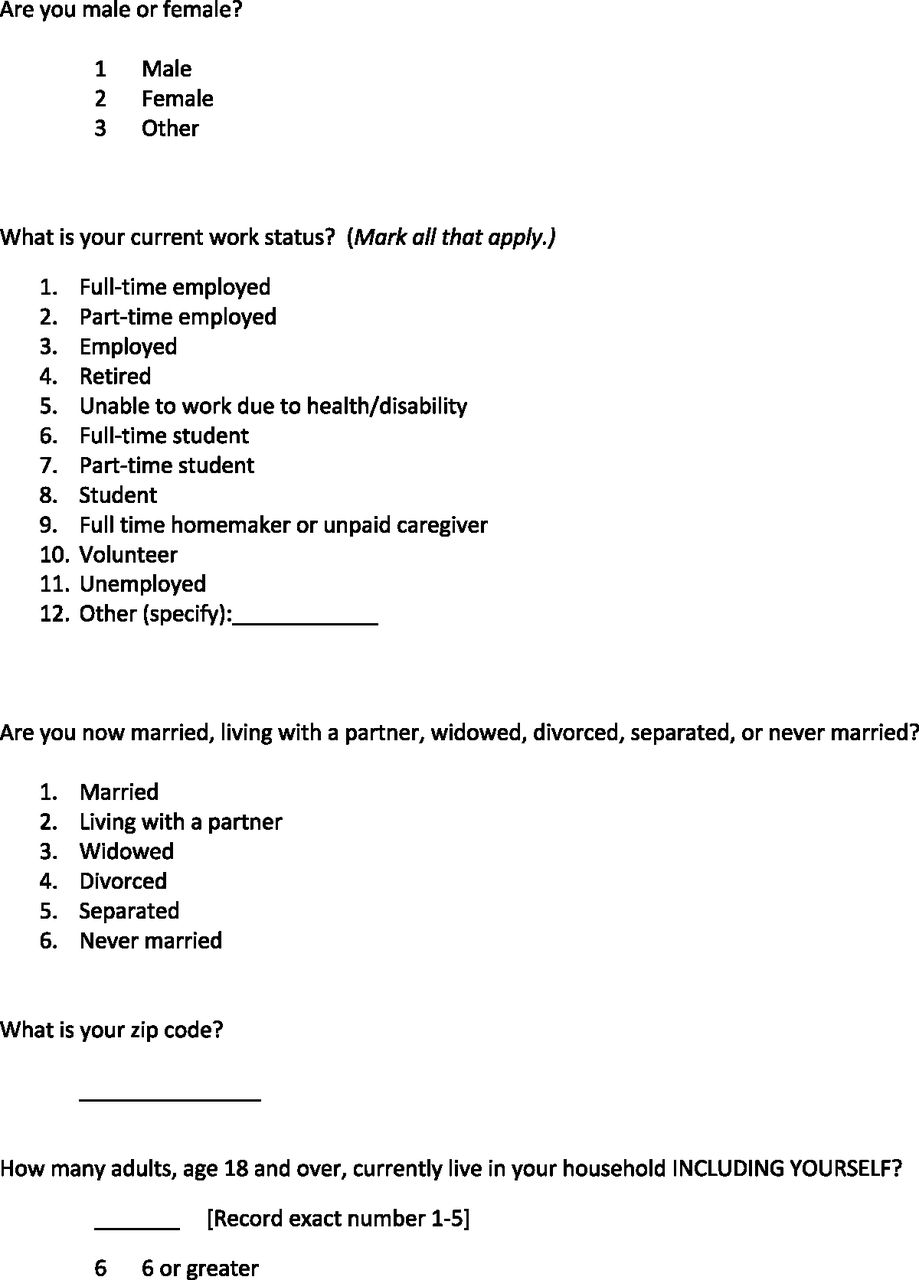
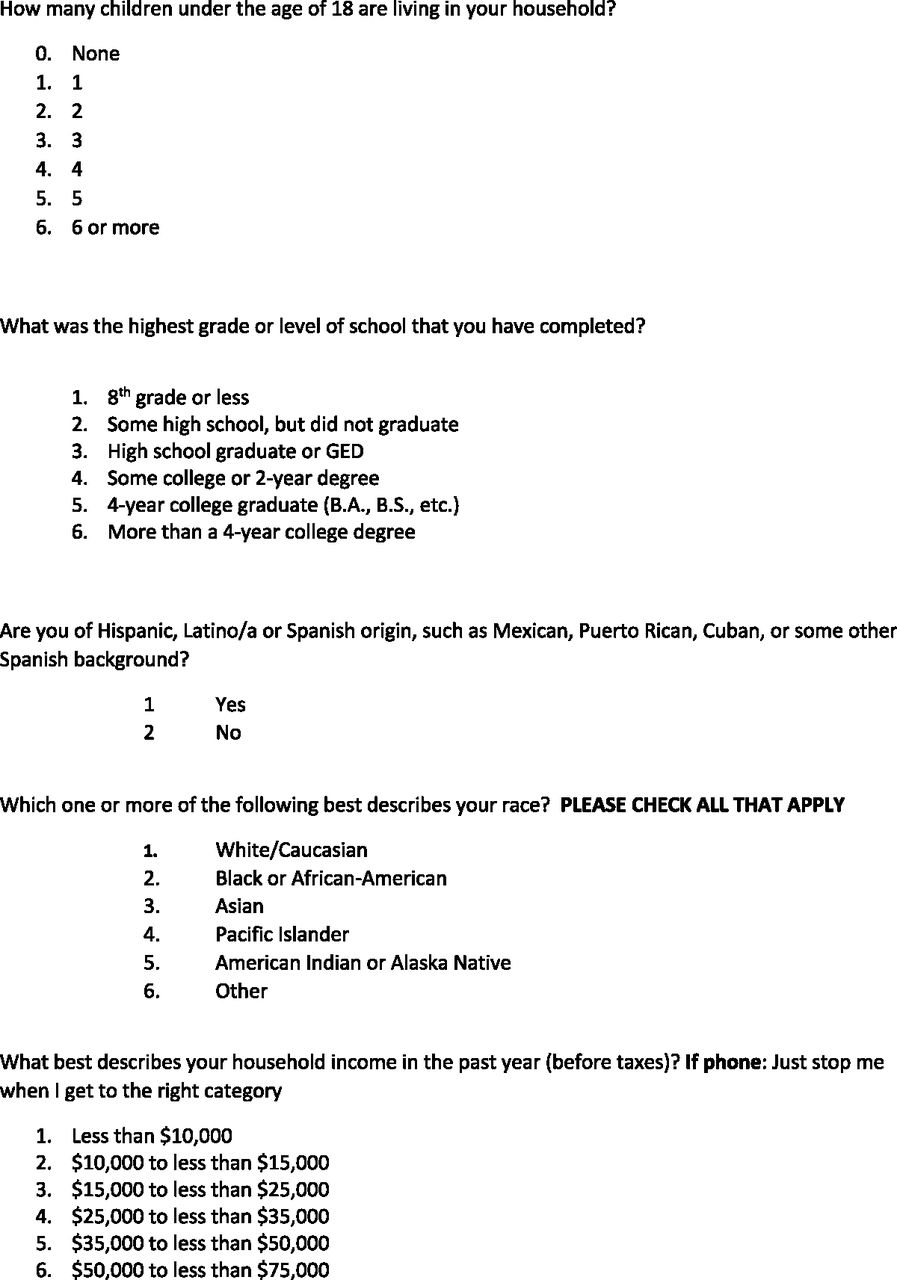
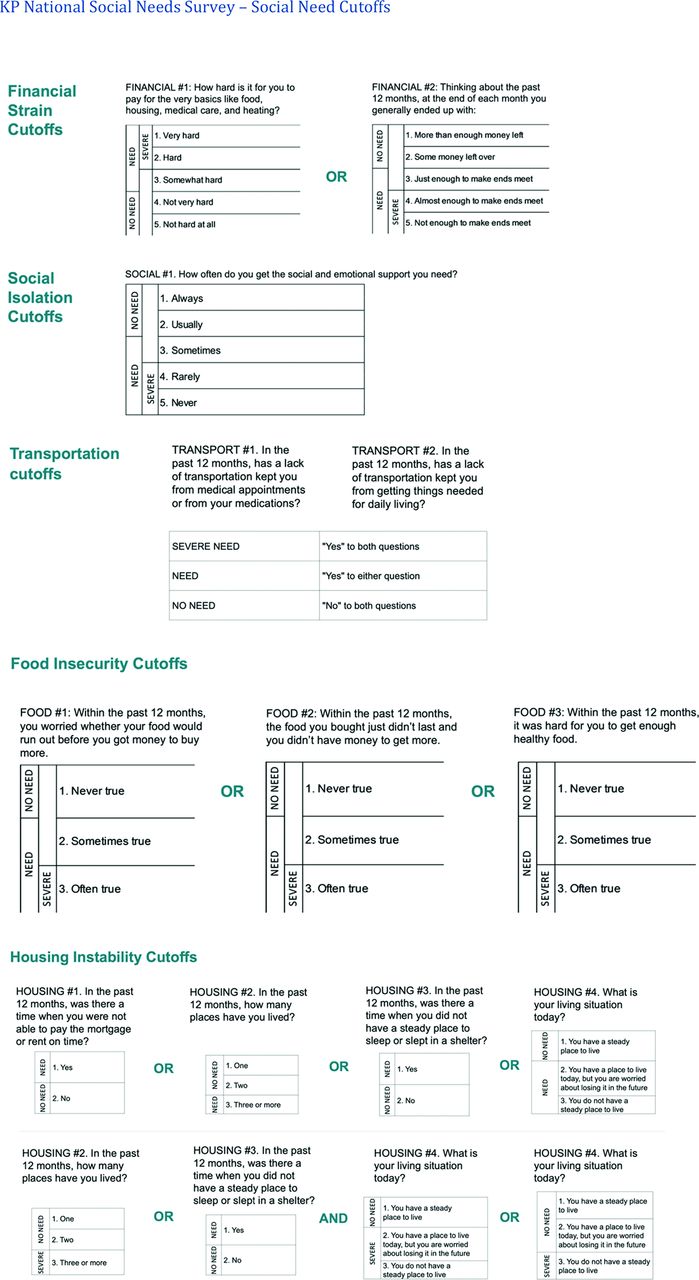
Self-reported social needs of Food Insecurity, Social Isolation, Transportation, Housing Instability, and Financial Strain were examined using the SONNET Social Needs Survey (Appendix A). The survey was available in both English and Spanish and conducted either online, via telephone, or on article. Respondents answered each of the 31 questions with either “yes” or “no,” or on a Likert scale of 1 to 5 or 1 to 3, depending on the question. Responses to each question were then categorized as “No Need,” “Severe Need,” or “Any Need” (Appendix B).
In addition, demographic information was analyzed in comparison to screening completion, including age, sex, race/ethnicity, insurance type, language, neighborhood deprivation index (NDI), and Diagnostic Cost Group (DxCG) risk score. Age was analyzed in groups above and below 65 years. Primary language was dichotomized as English versus Non-English as patient-reported primary language. DxCG scores were used as a proxy for disease burden. DxCG scores were stratified into very low (<0.25), low (0.25–0.7), moderate (0.7–1.3), high (1.3–3.0), and very high (>3) subgroups. NDI is reported in the EHR on a scale of 1 to 5, with 1 being the least deprived. The insurance plans within the KP system vary based on means through which that insurance was obtained and include Commercial (obtained through a patient or their domestic partner’s employment), Individual (bought through the health care exchange), Medicare, and Medicaid/Dual. Being employed is highly correlated with having commercial insurance within KP, and thus employment status was omitted from our models due to redundancy.
Statistical Analysis
Distribution of CRC screening completion was compared across measures of social needs and demographic characteristics via Chi-square and Kruskal-Wallis tests, for categorical and continuous variables respectively. Weighted logistic models were computed using the survey package in R for screening rate, 1 corresponding to severe social need in each of the 5 domains, adjusting for age, sex, race/ethnicity, DxCG, and insurance type. P-values from the Wald test are presented along with odds ratios—and their 5% confidence intervals—comparing the risk of screening for each covariate relative to its reference. The survey weights were chosen to make the sample representative of the national KP population. All survey results presented have been statistically weighted to account for oversampling and nonresponse bias. Weights were winsorized to the 99th percentile to limit extreme values, and prevalence rates account for stratification variables (ie, region, gender, age, risk).15
Results
Among the 3,443 survey respondents, 2,098 (60.9%) were below age 65 and 1,973 (57.3%) were female. Most were English-speaking (2,854, 82.9%) and White (2,162, 62.8%). All participants were enrolled in the KP Foundation Health Plan; (1,873 (54.4%) commercial, 296 (8.6%) individual [purchased via the exchange], 1,169 (34.0%) Medicare, and 105 (3.0%) Medicaid or Medicare/Medicaid combined (Table 1).
Among these 3,443 individuals, 2,805 (81.5%) were up to date on their CRC screening. Demographic factors that were significantly correlated with CRC screening included age, DxCG, and insurance status. Individuals were less likely to be screened if they were younger than 65 years compared with those who were older, and those with lower disease burden (DxCG) compared with those with higher DxCG. Rates also differed by insurance type, ranging from a low of 73% (216/296) completion for those with private insurance to a high of 88% (1,030/1,169) with Medicare. There were no significant differences in screening rates by sex, race/ethnicity, primary language, or NDI.
The prevalence of social needs within the study sample is presented in Table 2. Within this group, 55% (1,889/3,443) of respondents indicated some level of need, and 26% (8,87/3,443) reported a severe need. The need that was most reported was financial strain (37% [1,252/3,416] of respondents reporting any need, 13% [439/3,413] reporting severe need). Transportation issues were the lowest reported (4% [136/3,423] with any need, 2% [63/3,421] with severe need).
Not being up to date on CRC screening was significantly associated with having severe need in 3 of the 5 social need domains when adjusted for sociodemographic and health status factors (Figure 1, Table 3); severe financial strain (OR 2.1, 95% CI 1.3–3.4), severe social isolation (OR 1.9, 95% CI 1.2–3.2), and severe food insecurity (OR 2.5, 95% CI 1.2–5.3). There was a nonsignificant increase in odds for severe transportation issues (OR 3, 95% CI 0.93–10) and severe housing instability (OR 1.7, 95% CI 0.93–3).
Multivariable Analysis of the Association Between Social Needs and Uptake of Colorectal Cancer Screening
Discussion
In this population there was significant association between CRC screening rates with 3 of 5 social need domains: Financial Strain, Food Insecurity, and Social Isolation, after adjustment for demographic, health status, and neighborhood-level factors. There were nonsignificant but similar trends for Transportation Needs and Housing Instability.
Our study is the first we know of linking EHR CRC screening data to a variety of patient self-reported social needs. A recent study that explored the relationship between self-reported social determinants and CRC screening used only claims data and included only individuals from a single region, Washington, D.C. Our study draws on both EHR and claims data and encompasses a more geographically diverse population, with individuals from 7 different regions of the United States.16 Two other similar studies evaluated area-level deprivation with CRC screening, rather than individual-level, self-reported social needs data such as in our study.17,18
Prior studies have described barriers to completion of specific types of CRC tests, such as transportation difficulties and lack of social support as reasons for not completing a follow-up colonoscopy, because the procedure requires anesthesia and thus necessitates the patient have someone to drive them home.19 Another study noted how the hidden costs of screening are often cited by patients as a major consideration when deciding to screen, indicating the potential impact of financial strain.20
An ecological study addressing neighborhood social disadvantage found that census data for housing disadvantage (eg, multifamily residence and address changes) were significantly associated with decreased odds of completing CRC screening.21 Another study addressing predictors of CRC screening in California found an 89% increased odds of being up to date for CRC screening among individuals who were food secure, with lack of health insurance associated with 81% decreased odds of screening, but did not include other social needs. This study relied on self-reported screening data rather than medical records.22 Our study is unique in describing the impact of social needs in an insured population using patients’ EHR data and self-reported social needs.
There is a large body of research focused on interventions to increase adherence to CRC screening.11,23,24,25 A 2018 systematic review of various interventions found that among 73 randomized clinical trials, interventions that were associated with increased CRC screening rates included patient education, outreach, navigation, and patient and clinician reminders.22 The most effective strategies were direct mailing of fecal tests and patient navigation. The authors described navigation as a barrier-focused intervention, addressing logistic barriers, sociocultural education, and minimizing loss to follow-up. Individuals with social needs might be more likely to need navigation to complete CRC screening. However, it is unknown whether programs that address social needs in general (eg, food banks, ride shares) without specifically targeting CRC would result in increased CRC screening.
Our study has limitations. Data obtained within the KP population may not be generalizable to patients outside of this health care system. Furthermore, there was possible survey response bias, with respondents possibly being more literate and engaged in their health care. There was also no data collected on various individual-level factors such as health beliefs, education level, lack of trust, and patient embarrassment, all which may have acted as confounders.6,10 In addition, CRC screening rates were high, 81.5% (2,805/3,443) compared with 70% nationally in 2020.3 This high screening rate is likely in-part driven by characteristics of the KP system, in which patients all had some level of health insurance with no out-of-pocket costs for screening. It is notable that we found these results within a population in which there were no differences in screening among its subpopulations (ie, sex, race/ethnicity, or primary-language). It is also important to note that this study was completed in the year 2020, during the start of the COVID-19 pandemic. Most KP regions mailed fecal immunochemical test kits directly to patients due for screening during this time, and, in contrast to national decreases in breast and cervical cancer screening, research has shown that CRC screening rates did not decline during the pandemic thanks to increases in at-home stool testing.26 Lastly, we were unable to distinguish between a screening test versus a clinically indicated test (eg, anemia workup), nor were we able to distinguish between average risk versus increased risk patients. Test modality was also not analyzed, and social needs might impact the 2 most common tests, FIT and colonoscopy, differently. Despite these limitations, our study has several important strengths. Research has shown that KP membership is representative of the socioeconomic diversity of the national population, suggesting our results may provide valid applicability to settings outside of the KP system.27 Our sample represents a geographically diverse population nationally, and detailed, patient-reported social needs were found to be associated with CRC screening rates even among a fully insured population. These significant results show that social needs put pressure on health care outcomes despite insurance status, and therefore even primary care physicians with fully insured patient panels must take social needs into consideration when caring for their patients.
Primary Care physicians are well positioned to help assess and address these needs. Research has shown that EHR-based screening and referral systems within Primary Care can be successful in identifying and providing resources to patients with social needs.28,29 Kaiser Permanente’s Community Support Hub, a free online directory that can be filtered by area code and social need, is an example of one way health care systems can begin responding to the housing, food, and other daily needs of their patients.30 Furthermore, patient navigators who help with filling out forms, calling community partners, and other navigation services have been demonstrated to help patients access the resources to which they were referred.31
Conclusions
While there are many societal and health care reasons that social needs should be addressed, further research is needed to determine whether assessing and addressing these needs lead to increases in CRC screening uptake. Possible future directions to address social needs include developing systems through which clinicians can easily connect patients to community resources, and investing in health care navigators who can help ensure that those connections come to fruition. Quality improvement efforts to increase CRC screening should consider such interventions and evaluate their potential impact on screening uptake and other important health and wellness outcomes.
Acknowledgments
The Social Needs Network for Evaluation and Translation (SONNET) is funded by Kaiser Permanente’s Office of Community Health.
Appendix A












Notes
This article was externally peer reviewed.
Funding and conflict of interest: Dr. Green is a member of the National Colorectal Cancer Round Table steering committee, which is supported by the American Cancer Society and Centers for Disease Control and Prevention. She receives no compensation for this position except for travel to steering committee meetings. Dr. Ngo-Metzger is a member of the Screening Clinical Advisory Board for Guardant Health. Dr. Levin has received research funding from Freenome, Inc. No other authors have any conflicts of interest or financial disclosures to declare.
Results from this study were previously presented at a poster session at the American Society of Cancer and Oncology conference in June 2023.
To see this article online, please go to: http://jabfm.org/content/37/5/868.full.
- Received for publication December 30, 2023.
- Revision received March 8, 2024.
- Accepted for publication March 25, 2024.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}