
Abstract
Objective: The objective of this study is to describe the facilitators and barriers of telemedicine during the COVID-19 pandemic for primary care clinicians in safety-net settings.
Methods: We selected 5 surveys fielded between September 2020 and March 2023 from the national “Quick COVID-19 Primary Care Survey” by the Larry A. Green Center, with the Primary Care Collaborative. We used an explanatory sequential mixed method approach. We compared safety-net practices (free & charitable organization, federally qualified health center (FQHC), clinics with a 50% or greater Medicaid) to all other settings. We discuss: 1) telemedicine services provided; 2) clinician motivations; 3) and telemedicine access.
Results: All clinicians were similarly motivated to implement telemedicine. Safety-net clinicians were more likely to report use of phone visits. These clinicians felt less “confident in my use of telemedicine” (covariate-adjusted OR = 0.611, 95% CI 0.43 - 0.87) and were more likely to report struggles with televisits in March 2023 (covariate-adjusted OR = 1.73, 95% CI 1.16 - 2.57), particularly with physical examinations. Safety-net clinicians were more likely to endorse reductions in no-shows (covariate-adjusted OR = 1.77, 95% CI 1.17 - 2.68). Telemedicine increased access and new patient-facing demands including portal communications.
Conclusions: This study enhances our understanding of the use of telemedicine within the safety-net setting. Clinician perceptions are important for identifying barriers to telemedicine following the end of the Federal COVID-19 Public Health Emergency. Clinicians highlighted significant limitations to its use including clinical appropriateness, quality of physical examinations, and added patient-facing workload.
Introduction
Technology-based practice transformations can play a role in efforts to design high-value primary care by facilitating communication, improving team-based care, and centering patient preferences1 including the needs of underserved and vulnerable patient populations who receive care in safety-net settings.2,3 Safety-net practices are defined as practices that “organize and deliver a significant level of healthcare and other needed services to uninsured, Medicaid and other vulnerable patients.”4 For this study, we designate a safety-net clinic as any clinic that self-categorizes as a free & charitable organization, and/or a federally-qualified-health center (FQHC), and/or a clinic with a 50% or greater Medicaid population.
Prior to the COVID-19 pandemic, national data demonstrated that the expansion of state telemedicine policies alone was not associated with increased use of these services by underserved patient populations, or those who most often provided their care.4 Those studies show that low-income patients, patients with multiple chronic conditions, and patients in rural settings expressed a willingness to use telemedicine but were less likely to do so compared to middle-class, healthy, urban adults.5–7 It is hypothesized that these differences are in part due to inequities in access to high-speed internet services necessary for video-based telemedicine and lack of computer literacy, which disproportionately affects Black, Hispanic, poor, and rural households.1,8 Data regarding telemedicine access during the pandemic are consistent with pre-pandemic findings: differences in use of telemedicine exist based on patient socioeconomic and clinical characteristics, for both video and phone visits, in a variety of ambulatory care settings.12–16
A number of studies suggest that clinician factors may account for variations in the success of technology-enabled visits.10,11 However, few report on the implementation of telemedicine from the perspective of clinicians within safety-net clinical settings.17–21 In this study, we describe facilitators, barriers, and implications of telemedicine during the COVID-19 pandemic comparing primary care clinicians in safety-net settings from clinicians in all other practice settings. Our aim is to clarify the specific barriers to implementation in this setting, and to better understand the impact of the changing policy and service landscape during the COVID-19 pandemic on the ability of these clinicians to deliver telemedicine.
Methods
The “Quick COVID-19 Primary Care Survey” (C19 Survey) was fielded weekly, then monthly by the Larry A. Green Center, in partnership with the Primary Care Collaborative (a not-for-profit organization that aims to improve costs, quality, and delivery of health care) from March 13, 2020, to March 1, 2023. The 36 electronic surveys were distributed through professional networks, listservs, and to clinicians who opted to receive the survey directly by email, to cross-sectional cohorts that mirrored the demographic diversity of primary care nationally. The survey questions were vetted by a National Advisory Committee of subject matter experts established for the survey. These questions focused on pandemic issues such COVID-related practice strain, payment issues, and telehealth, and were modified at each survey to reflect the changing care delivery and policy environment during the pandemic. For this study, we selected surveys spread over the entire survey period that focused on telehealth questions with a sufficient sample of safety-net clinicians. This study was reviewed by the Virginia Commonwealth University School of Medicine Institutional Review Board as an exempt study.
For the purposes of this study, we focus on five surveys between October 2020 and April 2023, of unique survey populations. These five surveys include sets of questions on telemedicine usage during the height of the COVID-19 pandemic (October 2020, November 2020, March 2021, November 2021) and the time period leading up to the end of the federal COVID-19 Public Health Emergency (PHE) Declaration (March 2023) in May 2023. This time period allows for a longitudinal assessment of changes in telemedicine adoption and use. We use an explanatory sequential mixed method approach to analyze our data: the quantitative data provided evidence of generalizability and magnitude of effects. These findings then inform our analysis of the qualitative data from safety-net clinicians which serve to triangulate the validity of the quantitative data while also providing greater context to those findings.22 The key independent variable is defined as a binary indicator of safety-net setting (free & charitable organization, and/or an FQHC, and/or a clinic with a 50% or greater Medicaid population) or non-safety-net setting. These designations were made based on self-categorizations by survey respondents.
First, we identify three outcomes of interest pulled from structured survey questions: 1) types of telemedicine services provided; 2) motivations for offering these services; 3) and access to telemedicine by vulnerable populations. Logistic regressions are used to model the probability of each outcome: we performed univariate analysis of our independent variable and outcome at each time point with relevant potential confounders including practice characteristics (size, ownership, setting, state), clinician characteristics (specialty, training). Variables that confound the relationship between the independent variable (safety-net settings vs other) and the outcome (telemedicine use) were included as predictors in our multivariate analysis. Confounders changed with each model. Second, we undertake a thematic content analysis of the qualitative data using an editing style of coding to generate themes based on survey data.23 Each survey was independently coded by the primary investigator (AN) and at least one other coder (MG). Differences in coding were reconciled through discussion. Representative quotations were selected from the survey time periods included in the study from each thematic group. All statistical analyses were conducted using StataMP version 17.
Results
Sample Demographics
A total of 4,405 survey responses during five time points were analyzed for this study. Table 1 describes the clinician and practice characteristics of respondents. MD-trained family medicine physicians provided the majority of responses across surveys (64.1%–72.5%). Slightly under one-third of respondents provided care in safety-net settings (25.7%–28.5%) across the five time points.
Characteristics of Survey Respondents Who Participated in Five Instances of the Green Center Quick COVID-19 Survey, September 2020–April 2023
Key Findings
In the sections that follow, we describe our key findings grouped into the themes of Telehealth Adoption, Clinician Motivations, and Access to Care. In each section, we provide quantitative findings of structured questions, and qualitative findings of open-ended comments by safety-net clinicians to frame our statistical analysis results.
Telemedicine Adoption
Clinicians identified the speed of adoption of telemedicine within their practice as an important factor for maintaining care continuity during the pandemic. When prompted to share open-ended responses for critical weaknesses in telemedicine delivery as revealed by the pandemic, safety-net clinicians discussed several barriers including lack of reimbursement, the slow adaptation to the new healthcare environment, and the lack of knowledge sharing between practices as they made necessary changes to meet patient needs (Table 2).
Open-Ended Responses on Telemedicine Adoption from Safety-Net Clinicians, October 2020–November 2021
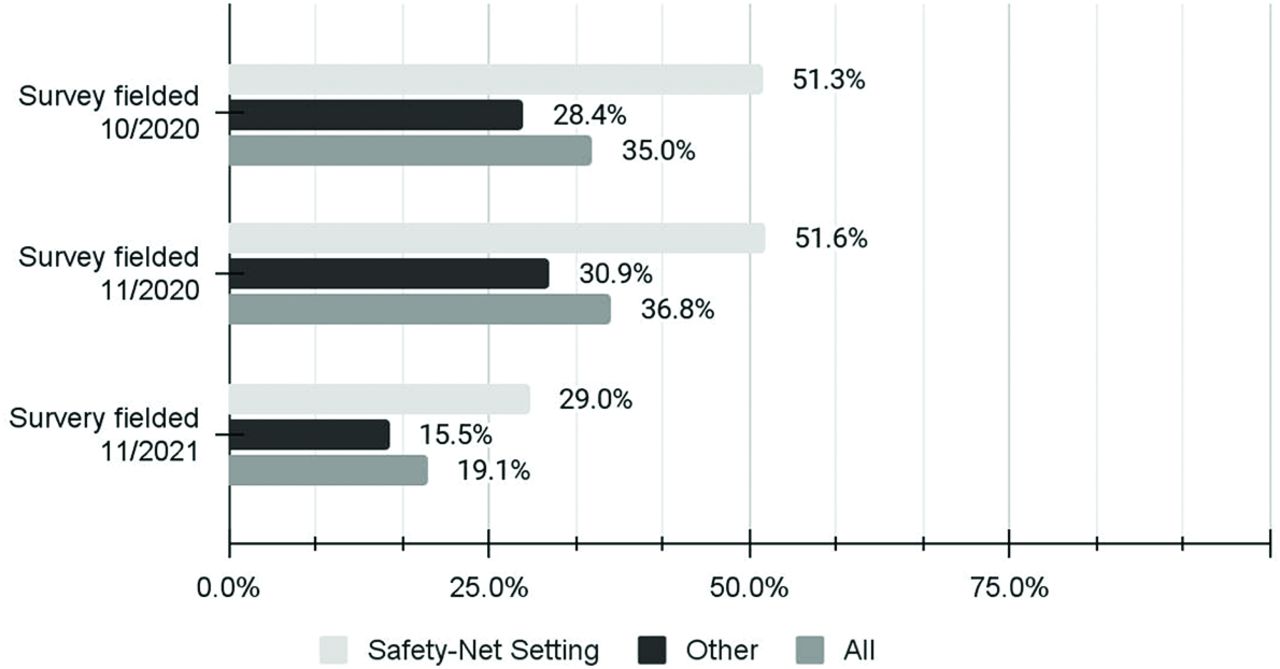
The modality of choice of virtual visits differed across the study period. As indicated in Figure 1 a greater proportion of safety-net clinics utilized phone-based care throughout the survey period. Table 3 shows results for phone-based telemedicine use between March 2020 and November 2021. Clinicians in safety-net settings were significantly more likely to report that 20% or more of their visits were conducted via phone (as opposed to all other telehealth or in-person visit types) than clinicians in non-safety-net settings when adjusted for clinician, practice, and patient characteristics through November 2021. This relationship shifted by the end of our study period. When surveyed: “we rely on telehealth (either phone or video) for at least 20% of patient visits” in March 2021, we continued to see a significant difference in telemedicine usage with safety-net clinicians less likely to use either phone or video visits when adjusted for clinician training and practice setting (p < 0.001).
Regression Results of Phone-Based Visits Use for at Least 20% of Total Visits Compared to All Other Modalities Among Primary Care Clinicians, October 2020–November 2021

Proportion of clinicians that reported using phone-based visits for at least 20% of total visits compared to all other modalities the COVID-19 pandemic, October 2020 – November 2021.
Clinician Motivations
Motivations for telemedicine use may have an effect on a clinician’s willingness to provide these visit modalities. In November 2021, when clinicians were prompted to select motivations for the use of telemedicine, a greater proportion of non-safety-net clinicians selected shifts in payments, increased access to care, and patient interest, among other possible motivations, though the differences were small (Figure 2).

Clinicians motivations for telemedicine use during the COVID-19 pandemic, November 2021.
In our multivariate analysis, safety-net clinicians were significantly less likely to report feeling “confident in my use of telemedicine with patients” (OR = 0.611, 95% CI 0.43 - 0.87). However, we found no differences in reported “gained confidence in my use of telemedicine during the pandemic” between groups. In March 2023, safety-net clinicians were significantly more likely to endorse the statement “telehealth - yes, it's here, but we still struggle to use it well. If only we had help!” (OR = 1.73, 95% CI 1.16 - 2.57).
In Table 4, safety-net clinicians expressed concerns about the limitations of physical examinations via telemedicine visits, which may contribute to multiple visits and the need for escalation. Furthermore, clarifications on which types of visits were better suited for telemedicine modalities facilitated positive clinical experiences. Clinicians viewed telemedicine as a tool that could enhance patient-physician communication with significant limitations.
Open-Ended Responses on Clinician Motivations from Safety-Net Clinicians, October 2020–November 2021
Access to Care
Widespread implementation occurred within the context of continued concerns about patient access and apprehension about the implications for clinician workloads. At the start of the pandemic, safety-net setting clinicians were more likely to endorse that the use of telemedicine contributed to access barriers for their patients compared to other clinicians (OR=1.60; 95% CI 0.99–2.57, p=0.050). Specifically, safety-net clinicians were more likely to report a lack of broadband (OR=1.97, 95% CI 1.35–2.88), and a lack of computer literacy (OR=2.16, 95% CI 1.44–3.26) in at least 20% of their patient population. Even with challenges in these patient populations, safety-net clinicians were more likely to endorse that telemedicine significantly reduced no-shows (OR = 1.77, 95% CI 1.17–2.68), thereby improving access to care.
While telemedicine increased access to care it also increased patient-facing demands on clinicians including a surge in patient calls and portal communications, as shown in Table 5. In open-ended responses, safety-net clinicians discussed the added burden that the pandemic had created on their workload along with the benefits to access provided by new care modalities.
Open-Ended Responses on Patient Access to Care from Safety-Net Clinicians, October 2020–November 2021
Nevertheless, these tools facilitated contact with patients who would otherwise face barriers to care due to age, transportation, or other social determinants of health during the period of limited in-person visits. Nearing the end of the Federal COVID-19 Public Health Emergency, in March 2023 we found no difference in endorsement that telemedicine “increased access to care for our patients—we don't want to lose it”; nor that it “increased use of health services overall” between safety-net and other clinicians.
Discussion
The COVID-19 pandemic presented a unique opportunity to explore the factors that influence the adoption and success of telemedicine services in safety-net settings, as perceived by practicing clinicians. Through our mixed-method approach, we quantified differences in barriers and facilitators of telemedicine implementation and characterized this data with open-ended responses from safety-net clinicians in settings of interest. In 2014, 63% of community health centers provided no telemedicine services25, and this figure rapidly changed by April 2020 when 53% of all visits to community health centers were by telemedicine.26 Consistent with our own findings, the Assistant Secretary for Planning and Evaluation briefing on national trends in telemedicine use in 2021 showed that disparities existed between video and phone visit access based on socioeconomic factors including age, race/ethnicity, insurance type, and income.27
Our study found that clinician perceptions are important for identifying barriers to continued use of these services following the end of the Federal COVID-19 Public Health Emergency. All clinicians were similarly motivated to implement technological transformations in patient care delivery. However, as demonstrated by Table 2, safety-net clinics were not provided with adequate shared resources for implementing telemedicine that was specific to their clinical context contributing to differing speeds of implementation. Several recent studies have indicated that different patient populations present unique infrastructural challenges beyond well-established differences in readiness at the patient level within medically underserved populations such as broadband access and computer literacy.16,17,26 Organizations that were able to rapidly transition from in-person to virtual visits may have had established champions or dedicated teams with adequate knowledge and resources to conduct the necessary foundational work that would facilitate a smooth transition.27,28 In our sample, safety-net clinicians continued to experience difficulties with telemedicine visits post-pandemic.
Our findings on clinician motivations indicate that safety-net clinicians were less confident in their skills at providing telemedicine, in particular determining which types of visits would be most appropriate for which modality and performing virtual physical examinations. Feasibility and techniques for virtual examinations by body systems are available which may promote buy-in by clinicians and lead to higher quality virtual care.29 Professional development in this type of care delivery will be essential for the continuation of phone and video visits in this setting. Nevertheless, clinicians appreciated the effect on patient-clinician relationships of technology-enabled visits. Overall, clinician experiences with telemedicine were positive, particularly during the period of limited in-person visits. By 2023, safety-net clinicians and all other primary care clinicians did not differ in their endorsement of improved care access due to telemedicine. Our study was limited by the nature of the study design: we were not able to track a single group of clinicians to determine whether use, barriers or facilitators, or confidence with the technology had changed over time. It is unclear in our data whether unresolved obstacles during implementation, including technical challenges and new workloads, contributed to this general preference to return to in-person visits.30 Our findings are strengthened by the large national sample and the comparative nature of our study design between safety-net settings and all other clinical settings. Further research is needed to track telemedicine utilization in specific subgroup settings such as clinics with language services or those providing care to a large pediatric population. To address clinician perceptions of virtual visits and increase preference for their use, guidelines should be created to address the fundamental challenges to widespread telemedicine usage post-pandemic.
Notes
This article was externally peer reviewed.
Patient and public involvement: Patients or the public were not involved in the design, conduct, or reporting, or dissemination plans of our research.
Funding: This study was supported by a grant from the Alpha Omega Alpha Carolyn L. Kuckein Student Research Fellowship. The data collected and analyzed for this study were supported by funding from the Agency for Healthcare Research and Quality (1R01HS028253-1), the Andrew and Corey Morris-Singer Foundation, and the Samueli Foundation.
Conflict of interest: The authors have no conflicts of interests to declare.
To see this article online, please go to: http://jabfm.org/content/37/3/409.full.
- Received for publication September 16, 2023.
- Revision received December 3, 2023.
- Accepted for publication December 11, 2024.




{kind=link}
{kind=link}