
Abstract
Background: Despite 2 decades of cancer survivorship research, policy, and advocacy, primary care in the United States has not fully integrated survivorship care into its generalist role. This manuscript describes innovative roles primary care physicians have adopted in survivorship care and how these roles emerged.
Methods: We conducted qualitative in-depth interviews with a snowball sample of 10 US primary care physician innovators in survivorship care. Interviews were recorded and professionally transcribed. Our team met weekly as interviews were completed to review transcripts and write summaries. We analyzed data using an immersion-crystallization process.
Results: Innovators did not receive formal survivorship training but gained knowledge experientially and through self-guided education. All worked in academic primary care and/or cancer centers; context strongly influenced role operationalization. We delineated 4 major role-types along a spectrum, with primary care generalist orientations at one end and cancer generalist orientations at the other. Primary care generalists applied survivorship guidelines during regular visits (“GENERALISTS+”) or focused on cancer treatment effects amid other comorbidities during blocked clinic time (“oncoGENERALISTS”). Cancer generalists focused on cancer-related sequalae during and after treatment; some provided continuity care to survivors (“ONCOGENERALISTS”), while others incorporated unmet primary care needs into survivorship consults (“ONCOgeneralists”).
Conclusions: Primary care survivorship innovations are occurring in academic primary care and cancer centers settings in the US. To move beyond the work of individual innovators, systematic investments are needed to support adoption of such innovations. For wider diffusion of survivorship care into community primary care, additional strategies that include primary care survivorship education and workforce development are needed to facilitate risk-stratified and shared-care models.
- Cancer Survivors
- Care Coordination
- Disease Management
- Family Medicine
- Preventive Health Services
- Primary Care Physicians
- Primary Health Care
- Qualitative Research
- Survivorship
- Workforce
Introduction
Despite almost 2 decades of cancer survivorship research, policy, and advocacy, initiated by the seminal 2006 Institute of Medicine report, Lost in Transition,1 and further stimulated by the 2016 Cancer Moonshot,2 primary care as a field has not systematically integrated survivorship care into its generalist role.3,4 Factors contributing to this are well-documented and include lack of communication infrastructure and care coordination between oncology and primary care5–9; ill-defined survivorship care roles7,10; and lack of standardized survivorship education.3,7,9,10 Since most patients with a history of cancer (“survivors”) receive most of their post-treatment health care from primary care physicians,11,12 with numbers expected to reach 26.1 million by 2040,13,14 solutions are urgently needed to more fully engage primary care.
While not widely diffused, innovative models of primary care survivorship care have emerged.15 Survivorship care includes preventive screenings, recurrence monitoring, managing cancer treatment late and long-term effects, including those related to psychosocial and sexual health, and care coordination.1,16,17 Roles conceptualized for primary care-trained clinicians in survivorship care have included “oncogeneralists” providing generalist care for cancer sequelae in cancer centers and survivorship-designated clinicians in primary care settings.10,18 Ideally, all primary care clinicians would participate in shared-care models, where primary care and cancer team roles and tasks are defined and coordinated during and after cancer treatment.10,19 Evidence suggests that primary care is necessary for optimal survivorship care and that primary care-engaged survivorship models are as effective and more cost-efficient than oncology survivorship models.3,20 Innovations in primary care survivorship need to be better understood to advance dissemination and implementation of these models.
When we first examined the primary care survivorship landscape in 2015, we found few pioneering examples of primary care clinicians providing survivorship care.4,21 With the “reinvigorated” focus and increased investment in survivorship care generated by the 2022 Cancer Moonshot22,23 and proposed Comprehensive Cancer Survivorship Act,24 we sought to reexamine the landscape to determine how far the field has evolved. In this manuscript, we describe the refined primary care survivorship roles we found and discuss the implications of these roles for survivorship care and the field of primary care.
Methods
We conducted individual in-depth, semistructured interviews between December 2021 and April 2022 as part of a larger NCI-funded study. Our steering committee and advisory board of nationally recognized leaders in survivorship research, policy, and advocacy recommended primary care physicians providing survivorship care to interview. Our inclusion criteria were that interview participants be trained in primary care and have additional training in survivorship care, merging elements of these roles in providing patient care. Using snowball sampling, we then asked each interviewee for their recommendations of primary care physicians providing survivorship care to interview. We concluded recruitment for interviews when participants began recommending the same people (see Figure 1). This research was approved by the Rutgers Institutional Review Board.

Snowball sample.
Data Collection
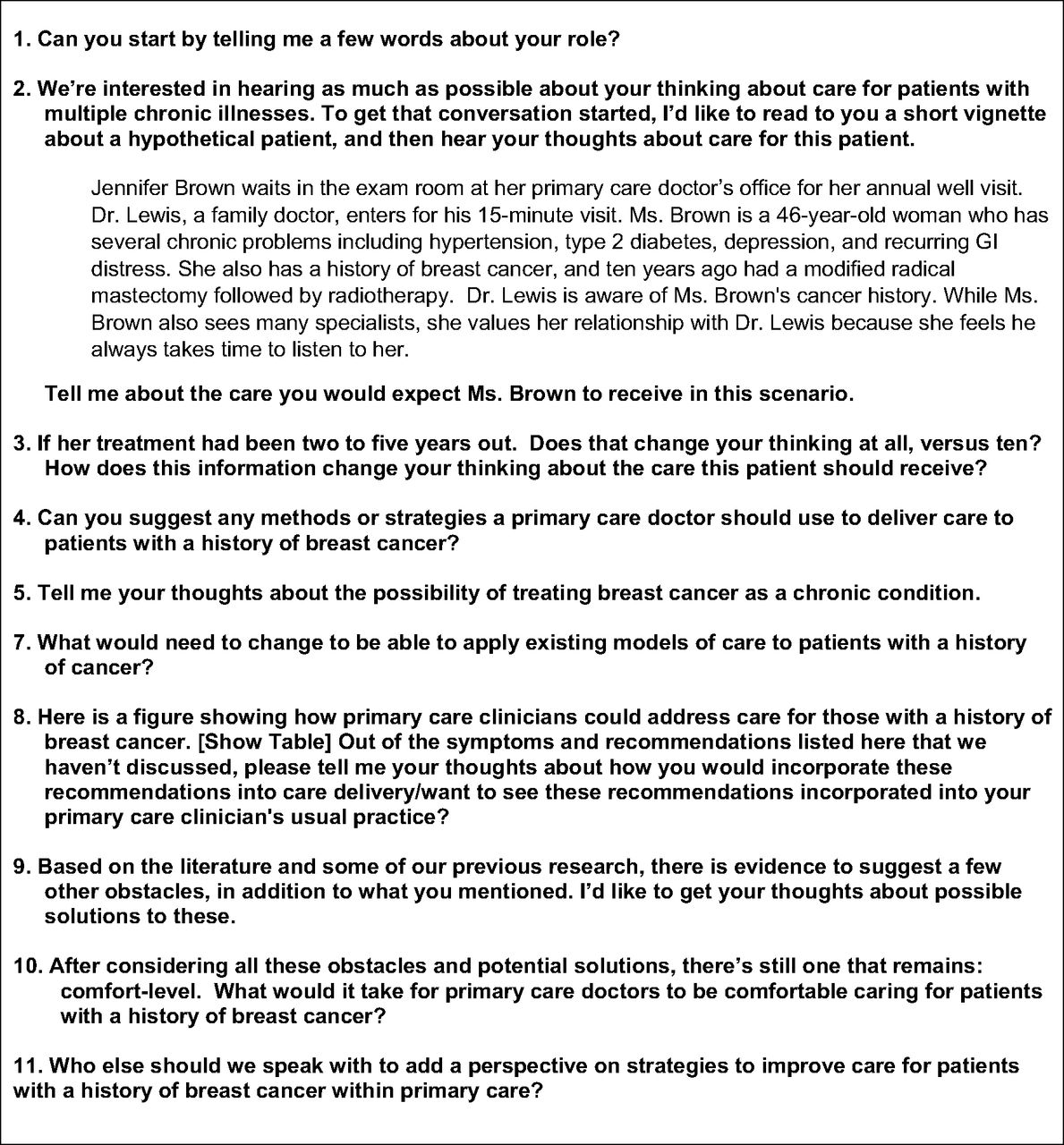
The authors designed a semistructured interview guide based on McCracken’s recommendations for combining a review of the literature and team member self-reflections.25 Grand-tour questions focused on primary care survivorship roles, training, and processes of care for breast cancer survivors, as our larger study focuses on primary care breast cancer survivorship care. We included questions about challenges and potential strategies for integrating survivorship care into primary care. (See Appendix for interview guide.) We supplemented interviews with information found on web sites and in publications that provided details about participants’ clinics, roles, and survivorship scholarship.
Interviews were conducted by a qualitatively trained medical sociologist (JH) with extensive experience researching primary care. After obtaining informed consent, interviews were conducted over Zoom, recorded, and professionally transcribed and deidentified. Interview duration averaged 49 minutes.
Data Analysis
The core analysis team (JRH, BFC, JH, LM, RK), consisting of methodological and content experts and researchers with decades of qualitative experience, conducted a 2-stage analytic process26 over a year of weekly meetings. First, we completed systematic, rolling reviews of interview audio and transcripts. After discussing each interview over a 2-hour period, the lead author wrote a 3- to 5-page summary detailing emergent themes. As themes began to crystallize, the lead author produced a matrix capturing key details of internal and external motivators and opportunities that enabled roles to emerge.27 The team then conducted an intense second round of analysis using a well-established immersion-crystallization process, repeatedly immersing themselves in the transcripts, summaries, and detailed matrix, reflecting on them to compare emergent themes until coherent themes across participant interviews crystallized.26
Results
We interviewed 10 primary care physicians known for providing survivorship care across all US geographic regions. Participants were female, 30 to 60 years in age, and identified as either White (60%) or Asian (40%). Two males with primary care survivorship experience were referred to us, but we excluded them since they were not actively providing survivorship care or primary care to patients. Most participants were trained in internal medicine (70%); others practiced family medicine. All worked in academic settings, most affiliated with NCI-designated cancer centers (90%). A few worked in the cancer center, either solely or in addition to their primary care clinic (40%). We labeled participants “innovators” because they represent pioneering primary care roles in survivorship.15
Our interview guide focused initial questions on breast cancer survivorship care, but innovators discussed survivorship models and roles more broadly. We found similarities in how innovators embarked on their survivorship roles and acquired skills and knowledge. Roles themselves were different, depending on clinical context; context also influenced criteria of survivors included in innovators’ scope of practice and complexity of knowledge needed. We describe these trends and roles below.
Innovators Experienced Similar Pathways to Survivorship Roles
While we interviewed innovators across the country from different clinical settings, we identified similarities in their experiences entering survivorship care roles. Most had prior interest in cancer or oncology but limited (if any) knowledge of survivorship care before embarking on this pathway. As one noted:
The word “survivorship,” never heard of it until I came here [academic medical center with affiliated cancer center]. Survivorship care plan, never heard of it. [I understood] the health history part and getting the history of cancer, but understanding that that could impact what treatment they received, could impact their current health status? That point [had] not [yet] sunk in. (Participant 1)
Most said they were recruited by others working in the survivorship field, most by an oncologist who recognized patient comorbidities were not being managed. Innovators described not receiving formal education in survivorship but learning from cancer specialists, research, conferences, online modules, and networking:
I learned a lot of the academic side of the literature from [being on an NIH grant] and going to [conferences] and seeing some of the clinicians who were presenting…. I would see some of the clinical applications [there]. There’s never been anything that I’ve learned [about] cancer survivorship from primary care itself, like in boards review classes. (Participant 3)
Given the lack of formal training, innovators described their relationships with cancer specialists as critical. Most innovators were introduced to survivorship care at the beginning of their academic medicine careers and were able to grow their panels from oncology referrals:
I started seeing [the breast surgeon’s] patients, and then started working more closely with the oncologists … discussing long-term side effects, as well as implications for young cancer survivors and some of the hormonal therapies … and started to share more and more patients with them … and then just grew my practice from there, and then subsequently expanded it [into a survivorship clinic]. (Participant 8)
Another explained that her first clinical faculty position enabled her time to go to oncology grand rounds and make connections: “I was there, and I did not have restrictions. My attitude was—has always been—send me whoever you want, I will never say no” (Participant 6).
Innovators also described learning experientially. Seeing large numbers of survivors consistently enabled them to identify trends, standardize question sets, and develop cognitive schema for interpreting symptoms in relation to cancer history. For example, 1 clinician described: “You just kind of build up your panel…. [T]hat’s where the practical knowledge comes in” (Participant 9). Another explained, “I am getting good at this because I—repetition is the key to mastery, you know? … And even if I do not know the cancer, I know … the questions that I am supposed to ask, the things that could be happening” (Participant 1).
Institutional support, beyond the professional support from the cancer specialists who initially engaged them, also helped advance survivorship roles. Most described having the freedom to operationalize their roles independently; few assumed predesigned roles carved out by the organization. Regardless of how roles materialized, roles aligned with institutional and health system missions. Participant 1 described, “This was like an area of the department that they were wanting to develop in this survivorship space.” Another working in a cancer center described their rationale for developing her role:
There were just challenges in getting people into primary care. People were having unmanaged comorbidities. People were not getting seen by their primary care during time of treatment… not getting screened for their other cancers and high ER utilization rates…. (Participant 7)
With institutional investment and support, innovators were able to structure visits differently. For instance, most described holding longer orientation visits (∼1 hour) and follow-up visits (∼30 minutes). Strategies innovators described included using special billing codes (eg, 99215), subsidization from their academic departments or cancer centers (eg, survivor centers or clinics were allotted administrative and clinical support), and/or grant, foundation, or philanthropic support to help compensate extended visit times.
While Pathways Were Similar, Different Survivorship Roles Emerged
A key finding was that innovators performed different primary care survivorship roles, which we characterized along a spectrum (see Table 1). At 1 end are roles in primary care practices that integrated survivorship care into generalist primary care orientations – those focused on “whole-person” care. We labeled these “GENERALISTS” and “oncoGENERALISTS.” At the other end are roles in cancer centers with cancer generalist orientations – those merging oncology-related and generalist care delivery processes. We labeled these “ONCOGENERALISTS” and “ONCOgeneralists.” Roles exist in a typology and are generalizations of innovators’ specific roles28; in reality, most innovators spanned roles and clinical contexts, however, the roles themselves are distinct. Table 1 provides a summary of key features and examples of these role-types. Below, we describe each in more detail.
Primary Care Survivorship Roles by Context and Orientation
Survivorship Innovations in Primary Care Contexts
Innovators providing survivorship care within primary care settings, GENERALISTS+ and oncoGENERALISTS, maintained primary care generalist orientations – a focus on the “whole person.” They cared for survivors mostly post-treatment and viewed cancer history as another comorbidity, like diabetes or cardiovascular disease.
The GENERALIST+ role required basic knowledge of survivorship guidelines, particularly screening surveillance, late and long-term effects, and psychosocial needs. Because these innovators saw survivors within their panels, they first needed to identify patients as survivors and then use this knowledge to direct their questioning. One GENERALIST+ explained:
I’m not seeing them in particular for survivorship…. I’m seeing them for … high blood pressure, diabetes, or so on and so forth. But knowing that they have [cancer] history, I make it a point to ask them about what the follow-up is … who’s your oncologist, when was your last treatment, what did they say? … are they experiencing anything from their cancer? (Participant 10)
Only 1 of our innovators, a physician in a community setting, described working with her colleagues to create a registry of cancer survivors from the clinic’s patient panel. She offered each survivor a consultative visit, during which she wrote action items in the problem list of the EHR for other clinicians to follow:
Like mine wasn't a care plan …. I was just in the problem list, I would add the things that they needed … something like patient has an oncologist at where, and if we know the name. They go every March, and they get a breast MRI every March that’s ordered by that person… [then] when my colleague sees it, there's no ambiguity or question about what's going on…. My colleague doesn't have the time to figure that out. (Participant 3)
GENERALISTS+ were able to ask standardized questions, interpret treatment history, and use this information during exams to ensure survivorship guidelines were being followed and enable colleagues to do the same.
oncoGENERALISTS were generalists with a special focus on survivorship. These clinicians often started their own primary care survivorship clinics in their practices, blocking time for consultations. Some also saw survivors as part of their continuity panels. oncoGENERALISTS needed more advanced knowledge of cancer and cancer treatments than GENERALISTS+, spending more time treating wider ranges of cancer treatment-related comorbidities, yet they retained their primary care generalist orientation:
I think what we at my group do a little differently is probably have all the familiarity with some of the therapies … and some other oncologic sub-type treatments, and the potential side effects and latent side effects that go with those…. But it's putting that therapy in context of their other disease states at the time you're seeing them…. I'm still an internist at heart, right? (Participant 8)
Treating large numbers of survivors increased the need for oncoGENERALISTS to maintain fluency in cancer treatments and potential side effects. Participant 8’s clinic held monthly “mini-tutorials” and case discussions on emergent therapies for their own clinicians, and clinicians frequented oncology grand rounds. oncoGENERALISTS were also committed to educating other primary care clinicians, recognizing that survivorship knowledge tailored for primary care must come from primary care. Some held educational workshops with community clinicians and residents (eg, Project ECHO29). Others authored survivorship modules and texts. They described positioning themselves as resources for clinicians, understanding the support, infrastructure, and education needed to enter the survivorship space.
Survivorship Innovations in Cancer Center Contexts
Innovators working in cancer centers, ONCOGENERALISTS and ONCOgeneralists, treated survivors during and after treatment. They worked as part of oncology teams and described intricate knowledge of oncology treatment regimens and their sequelae, developing cancer generalist orientations.
ONCOGENERALISTS balanced primary care and cancer generalist orientations. One explained that she provided primary care to cancer survivors and their families, including continuity care and “acute and urgent-care needs for any patients who have other primary care clinicians but are unable to get in with them.” For survivorship, she described providing acute care beyond the oncoGENERALIST role, above; but she described most of her care as within the scope of primary care:
I’m probably doing more fluids and management of chemotherapy side effects [than primary care clinicians]. Things like nausea and antiemetics during chemotherapy… during the active treatment phase … in coordination with our oncology team…. I do a little bit more in terms of management of some of the late and long-term effects… neuropathy management … anxiety-depression management … mental and behavioral health aspects…. But I stay very much restricted to primary care. I don’t much extend beyond the scope of that. (Participant 7)
ONCOgeneralists, on the other hand, had fully developed cancer generalist orientations. They described themselves as “survivorship physicians” (Participant 4). One explained: “I am not providing primary care … when I see patients here in survivorship, I am a consultant … who sort of is holistic in my approach” (Participant 4). Another ONCOgeneralist, who moved between cancer-specific pods, described providing “a holistic comprehensive view of their health care” (Participant 6). Because her population of survivors was underserved, often reconnecting to health care at the time of their cancer diagnosis, she described herself as “the survivorship doctor that is also giving them other chronic health conditions diagnoses…. We discuss the importance of chronic disease management in the setting of a cancer diagnosis.” She viewed her role between oncology and primary care:
[I’m] the person who sits between PCP and cancer specialist, right? And I fit that in-between role…. I’m communicating with the PCP as well as if they need another cancer clinician, too…. Most of our patients don’t actually have PCPs yet, so I’m trying to manage their chronic conditions and get them in with primary care physicians so that they can establish a relationship with them. (Participant 6)
ONCOgeneralist Participant 6 also described comanaging survivorship care with primary care physicians until they were comfortable providing survivorship care, for as long as that process would take. In addition, ONCOgeneralists described “uptraining” primary care clinicians through shared patient care, especially through writing primary care-focused notes for them about patient-specific survivorship needs.
Discussion
In our reexamination of the field, we found limited diffusion but notable refinements in early innovations of primary care survivorship roles.10,18,21 We differentiated 2 main types of survivorship roles in primary care settings: GENERALISTS+ identified survivors from patient panels and employed cancer-history-related question sets and algorithms in their care; oncoGENERALISTS held primary care survivorship clinics for consultations about cancer-treatment-related sequalae. We also delineated primary care-based roles in cancer centers: ONCOGENERALISTS provided acute and long-term survivorship and primary care; ONCOgeneralists provided survivorship consultations and primary care as needed. Role operationalization was influenced by the local primary care or cancer center contexts, but also by the complexity of patient care needs and specialized knowledge required in those contexts. As the field of cancer survivorship has matured, risk-stratified models have been endorsed to provide greater clarity in role definition between primary care and oncology based on patient factors and to support chronic care needs.10,18 These innovator roles were not created expressly to support risk-stratified models, but the increased role specification we found in relation to context suggests an implicit incremental movement toward adopting these models. Hence, operationalization of risk-stratified care models could help delineate which generalist role would be optimal for survivors and the care processes and training needed to support more systematic adoption of primary care survivorship care.10
Importantly, most of the roles we identified are not transferable to or scalable in community primary care settings. Innovators emerged exclusively in academic health systems and/or cancer centers. These institutions provided clinicians structural support and resources: the time to dedicate to learning about survivorship, the necessary infrastructure to support connections to oncology,30 and the ability to hold longer survivorship visits. However, innovators describe supporting community physicians in providing informed approaches to survivorship care, suggesting some degree of knowledge transfer. For instance, on the GENERALIST- side of the spectrum, innovators designed educational materials and centralized resources for community primary care physicians. Innovators on the ONCO- side “uptrained” clinicians through shared patient care. All role-types provided consultations and notes, translating oncologic history into action items. Whether favoring cancer or generalist orientations, most reported acting as intermediaries or bridges between oncology and primary care due to lack of formalized primary care survivorship care training and communication pathways between oncology and primary care.
The GENERALIST+ role is the most aligned with and has the greatest potential to transfer into nonacademic primary care settings. In 1 unique example, clinicians assembled a registry of their survivor patients, not a common practice in primary care settings,4,30 and 1 physician scrubbed their charts, met with these patients, and wrote action items in the problem list for other clinicians to follow. This process required up-front investment – clinician cooperation in creating a clinic-wide survivor registry, a knowledgeable survivorship champion, and extended survivorship orientation visits – but clinicians (eg, Advanced Practice Providers [APPs]) in community primary care settings could adopt similar survivorship-focused chart prepping procedures. Developing the competencies of the GENERALIST+ role has potential to benefit the largest numbers of survivors, as community primary care settings see the majority of survivors.11,31 Community primary care settings also tend to see survivors with less complex cancer-related needs,32 thus these roles do not require the intensively specialized knowledge and training we observed among ONCOGENERALISTs and ONCOgeneralists.
To support integrating survivorship care into primary care, primary care-based survivorship education needs to be integrated into medical education and expanded on for advanced training.10,33 Training and role delineation would also help prepare other clinical primary care roles, such as APPs, to support the growing needs for survivorship care within primary care. Without additional training, investment, and support, primary care survivorship roles are likely to remain innovations in elite spaces. A systematic review found considerable variation in primary care clinician knowledge and confidence in survivorship care within domains of prevention and surveillance of cancer recurrences; surveillance and management of physical effects, psychosocial effects, and chronic medical conditions; and health promotion and disease prevention.33 Basic residency or postgraduate medical training in survivorship guidelines, cancer treatments, and side effects of the most common cancers is needed for the GENERALIST- end of the spectrum. Once clinicians have awareness of survivorship as a health status, simple strategies such as keeping cancer history in the problem list can help clinicians incorporate survivorship into routine care. Advanced fellowship training in oncology treatments and complex multi-morbidities can prepare primary care physicians for the ONCO-side of the spectrum. Cancer centers could incorporate these advanced survivorship primary care physicians into their settings so that survivors would receive whole-person care during active treatment. While there are concerns about primary care overspecialization,34–36 we view these 2 education pathways as enabling diversity in primary care survivorship roles, helping survivors receive primary care and survivorship care from the type of clinician best suited to serve their needs.32,37,38 A range of primary care roles could be delineated to support the implementation of risk-stratified models and resource- and knowledge-sharing between community and survivorship physicians, resulting in better potential for shared care across the cancer continuum.
Limitations
We interviewed 10 primary care physicians delivering survivorship care in the US. An effect of snowball sampling, interviewees knew each other and often recommended the same person to us to interview. This suggested to us that innovators comprise a small, select group. However, it is possible that we reached a bounded group with limited perspectival and experiential variation and, as such, did not find other primary care-based survivorship roles (eg, APPs) or ways of integrating survivorship care into primary care. In addition, while interviews were rich, we did not receive specific information about institutional support in terms of funding lines or resource allocations that enabled many of these roles. As interviews were conducted over Zoom, we were not able to observe innovators at work, missing opportunities for viewing negotiations between primary care and survivorship care.
Conclusion
In the absence of widespread diffusion of survivorship care in primary care, primary care survivorship innovators have emerged in academic primary care and cancer center settings. To promote adoption of survivorship care in community primary care settings, systematic investments are needed in education and workforce development. A range of primary care roles across settings would help facilitate risk-stratified and shared care models, bridging gaps in both primary care and survivorship care.
Acknowledgments
We thank our interview participants for sharing their experiences and insights with us. We also thank our steering committee and advisory committee for imparting their knowledge and recommendations.
Appendix

Interview guide grand tour questions.
Notes
This article was externally peer reviewed.
Funding: This work is supported by National Cancer Institute Grant R01CA257197. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funder organization.
Conflict of interest: The authors have no conflicts of interests to disclose.
To see this article online, please go to: http://jabfm.org/content/37/3/399.full.
- Received for publication June 8, 2023.
- Revision received December 1, 2023.
- Accepted for publication December 11, 2023.




{kind=link}
{kind=link}