
Article Figures & Data
Figures
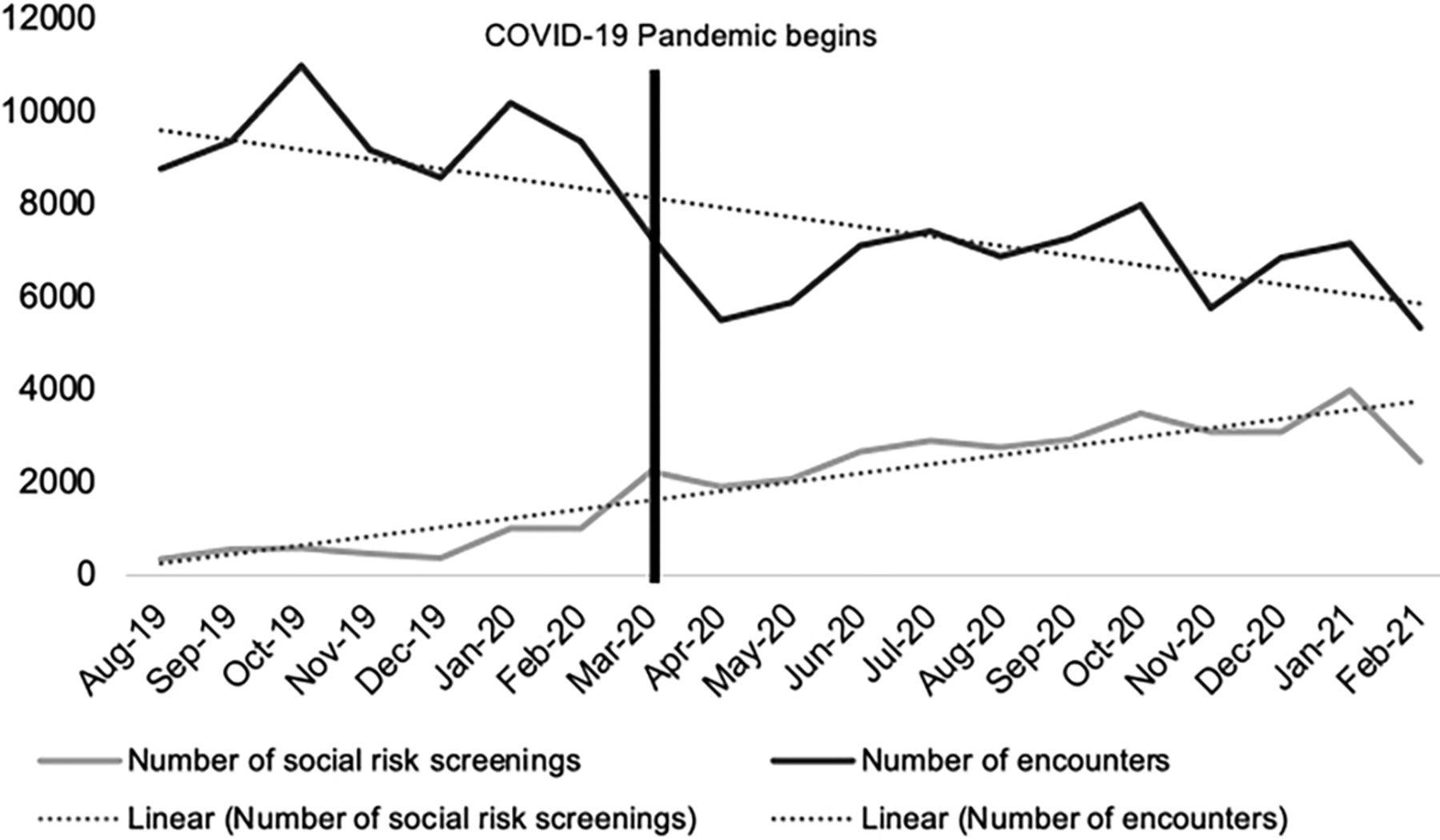
- Figure 1.
Trends in number of monthly encounters and social risk screenings at 2 community health centers (CHCs) August 2019 to February 2021.
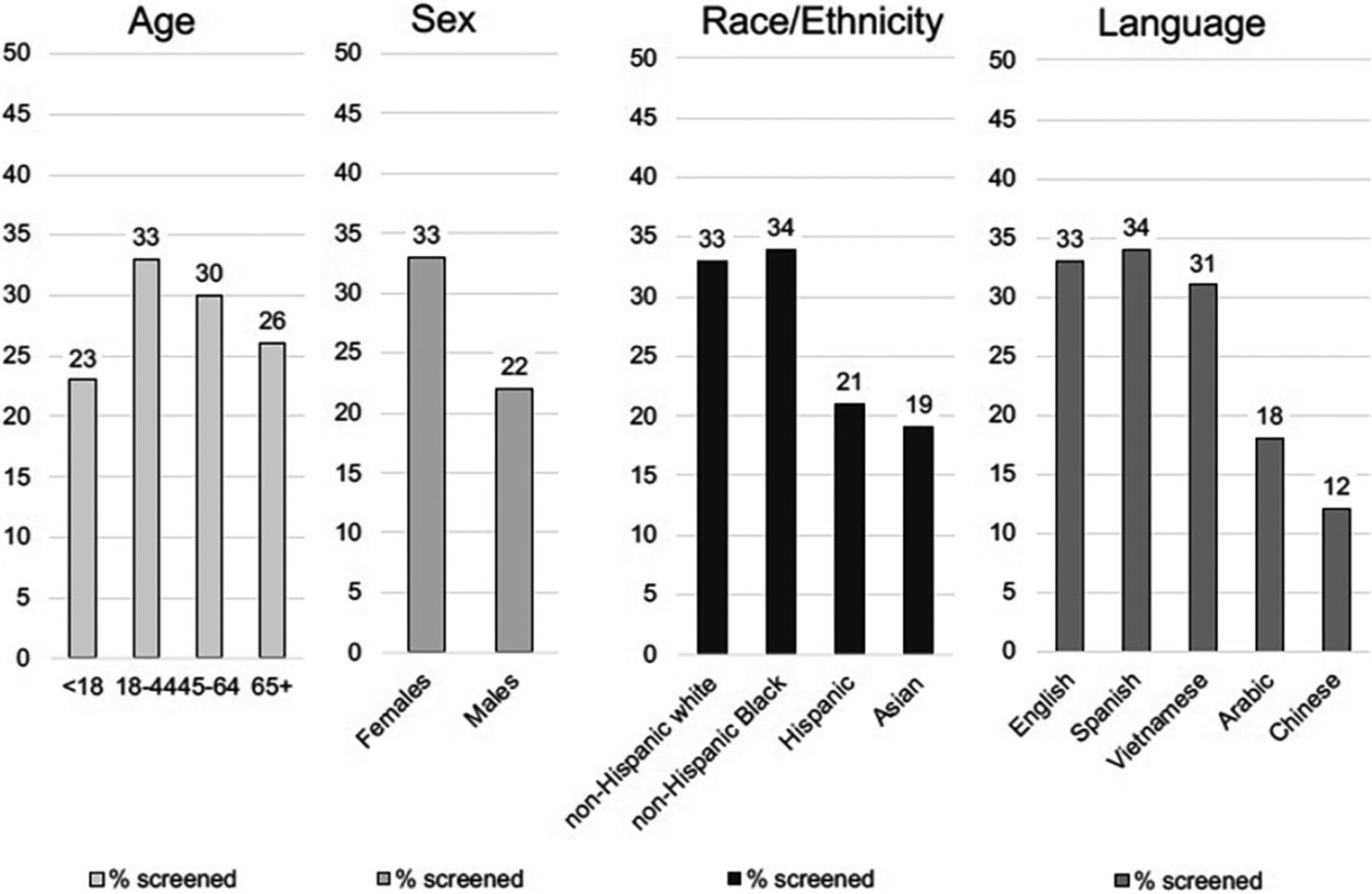
- Figure 2.
Proportion of patients screened for social risks at least once at Site 2, stratified by patient demographics (n = 10,436 patients).


Tables
Interviews Surveys EHR Data Staff Providers Providers Patients Site 1 4 5 9 8,236 unique patients screened for social risks Site 2 1 3 31 35,635 unique patients (10,436 unique patients screened for social risks) Site 3 3 3 45 – Site 4 4 4 12 – Total 12 15 97 43,871 unique patients; 18,672 unique patients screened for social risks Abbreviation: EHR, Electronic health record.
- Table 2.
Demographics of Participating Staff (N = 12 Interviews) and Providers (N = 15 Interviews; 97 Surveys)
Demographics of Staff/Providers Interviews Surveys Staff
N = 12Providers
N = 15Providers
N = 97N (%) N (%) N (%) Age 20 to 24 1 (8.3) 0 0 25 to 34 9 (75.0) 6 (40.0) 29 (33.0) 35 to 44 1 (8.3) 7 (46.7) 33 (37.5) 45 to 75+ 1 (8.3) 2 (13.3) 22 (25.0) Gender Man 3 (25.0) 5 (33.3) 22 (25.3) Woman 9 (75.0) 10 (66.7) 61 (70.1) Non-binary 0 0 1 (1.1) Prefer not to answer 0 0 3 (3.5) Race/ethnicity Non-Hispanic White 3 (25.0) 1 (6.7) 34 (39.1) Non-Hispanic Black 2 (16.7) 4 (26.7) 7 (8.1) Hispanic 5 (41.7) 4 (26.7) 15 (17.2) Non-Hispanic Asian 2 (16.7) 6 (40.0) 16 (18.4) Other/Non-Hispanic multiple races 0 0 9 (10.3) Prefer not to answer 0 0 6 (6.9) Years working at clinic Less than 1 1 (8.3) 2 (13.3) 11 (12.2) 1 to <3 3 (25.0) 3 (20.0) 33 (36.7) 3 to <5 5 (41.7) 4 (26.7) 26 (28.9) ≥5 3 (25.0) 6 (40.0) 26 (28.9) Theme 1: Broad Support for Social Risk Screening/Care Integration Subtheme Provider/Staff Illustrative Interview Quotes Provider Survey Data EHR Data Increase in screening efforts The reason why we passed the torch to the back [as opposed to front office] is because once the patient gets to the back of the clinic, that's when they open more […][T]rying to figure out where should we be screening for SDoH, ‘Should it be in the front? Should it be in the back? Should it be the doctor? Should it be the MA? Should it be once we connect them to the care coordinator?’ to see when the patient would actually give us the right answers or not the right answers, but the honest answers. – Staff
[T]he constraints that we have on all that just make it hard when time is such a factor for our visits. But I still find it important, so I still incorporate [social risk screening] into my visit somehow. -- ProviderSocial needs screening activities at my clinic have (1 = Decreased; 10 = Increased) (n = 87):
Mean 6.8, 0.23 S.E.,* 95% CI 6.4–7.3Combined social risk screening rate† at Site 1 & 2:
August 2019: 4.1%
February 2021: 46.1%
Peak: January 2021: 55.9%Mission aligned [T]his [is] the stuff that this place has been attuned to for a long time. I mean, before we were calling things social determinants of health…what they talked about was treating the whole person in a holistic view and providing wraparound services. And so having social work, talking about resources, trying to connect with resources, partnering with other agencies, that was something that the folks here were already attuned to and doing when I got here. So when things came up in the course of treating patients or working with patients, it was very much felt to be part of their care for us to try to connect them with resources and stuff. But we weren't proactively looking for issues around social determinants of health in any systematic or standard way. …the idea of advocating around those issues and the idea of trying to have the resources has been kind of long-standing. – Provider Social needs screening and referral activities at my clinic have become (1 = Less important, 10 = More important)
(n = 87):
Mean 7.4, 0.24 S.E., 95% CI 6.9-7.8- Facilitated by trust/longstanding position in community [T]he reason we're asking these questions is knowing that all of this impacts your health, and we want to do better to support you on your journey to health as much as we can, based on the work that's being done here. And so I think trust-building takes a long time. Just by being in the community for more than 25, 30 years, folks know us, we've been around for a long time and always strive every day in our services to communicate the fact that it really doesn't matter to us race, ethnicity, belonging. But we are here to provide the best quality services possible. And then our initiatives, whether it's food prescriptions, or medical legal partnerships, and other things that we're working on all stem from the fact of wanting the best possible health for our folks. – Staff The likelihood that patients at my clinic bring up topics related to their social needs has (1 = Decreased; 10 = Increased) (n = 89):
Mean 7.1, 0.20 S.E., 95% CI 6.7-7.5- Theme 2: Barriers to social risk screening efforts could be traced back to lack of time and staffing, which contributed to downstream inequities in screening reach Time barrier to screening [W]ell, not all of them answer the questions, so sometimes we have to ask the questions but we don't always have the time to go over the screening, especially if someone that we have seen multiple times or is something that just not addressed in the visit. …the majority of patients don't like filling out information. … They think they've done it before, so they don't want to do it every time they go into the clinic. – Provider Perceived barriers to screening:
I didn't have enough time to conduct screening:
Major barrier: 45 (54.2%)
Minor barrier: 22 (26.5%)
Not a barrier: 16 (19.3%)- Staffing barrier to screening [I]f a patient is screened by one of our community health workers or health educators, then the staff is the one who is updating that on our EHR, so that the provider can … see that updated information on if and how the patient was helped and if a referral is made. Sometimes, our community health workers and health educators just get overworked. – Staff There were technology barriers to conducting screening:
Major barrier: 10 (23.2%)
Minor barrier: 30 (36.6%)
Not a barrier: 33 (40.2%)- Language/literacy barriers to screening [T]he other challenge, with their patient population, with the educational background, and then the language barriers…They've made it at the most basic level for patients to understand as best they can, but there's still just those barriers from the patient side. The MAs can do it efficiently, but then there's still some information that the patient may not want to share directly, so it's easier to put on a form, but then those forms are not in the right language. But we offer all of those things in different languages, but there's still that barrier. Patients still can't quite necessarily grasp it, or need helping filling it out, but then that takes time, and then the MA will have to walk them through it, so then that just bleeds into … like domino effect. – Provider - see Figure 2 & Table 4 Other barrier: Lack of social services Well, the easiest one is the food insecurity one because we literally have a resource that comes to the campus. Don't have to tell them. The thing that I've noticed is you can give them information about a resource, but if it's way too out of their way, they're not going to utilize it. – Staff
[A] paper resource guide is a great first step. Our electronic resource guide is a great first step, but we know it has to be more tailor made[.] Also do these organizations truly have capacity. So that's another thing to see with health navigation, is where are we referring to? What's the success rate of referrals and where are those gaps. And why is there no capacity? – StaffPerceived barriers to screening:
There were no/not enough community social services or community resources available to address our patients' needs so I didn't think it made sense to screen for these needs.
Major barrier: 21 (25.0%)
Minor barrier: 32 (38.1%)
Not a barrier: 31 (36.9%)- Other barrier: Lack of communication as barrier to screening efforts [W]e have periods where we hear a lot and others where we just don't hear anything at all. I would say maybe two or three times a year, we have a push for, ‘Don't forget to do the screening, now this is happening.’ …when they have an initiative, they announce it and it becomes big, and with time it kind of starts fading. Then we hear it again, and then it starts. – Provider Perceived barriers to screening:
I didn't have enough training or experience to conduct screening:
Major barrier: 17 (20.2%)
Minor barrier: 30 (35.7%)
Not a barrier: 37 (44.1%)- Other barrier: Top-down approach to decision making as barrier to screening efforts I don't think they seek out clinician feedback. They kind of just decide a workflow, try it out, and then if it doesn't work, they're like, ‘Oh.’ But it seems like, and I've mentioned this to them before, it's wasted effort. Because, if you have someone on the clinical side, it doesn't even have to be a clinician it can be a medical assistant, it can be a nurse, someone who's on the floor present at these discussions about clinical workflow, then, one, it will probably flow better when it's actually implemented. And two, you haven't put in a lot of work to something that might not work. – Provider - - Abbreviations: SE, Standard error, CHC, Community health centers, EHR, Electronic health record.
↵† Social risk screening rate: number of patients screened for social risks by standardized CHC screening tool per month/number of patient clinical encounters per month.
- Table 4.
Differences in Demographics of 10,436 Patients with ≥1 Documented Social Screen Compared to 25,199 Patients Never Screened at Site 2 (n = 35,635)
Total Screened at least once for social risks Never Screened P value n = 10,436 (29.3%) n = 25,199 (70.7%) N N (%) N (%) Patient level-characteristics Age (years) (n = 34,414 patients)* <18 10,569 2,391 (22.6) 8,178 (77.4) 18 to 44 14,907 4,929 (33.1) 9,978 (66.9) 45 to 64 7,231 2,186 (30.2) 5,045 (69.8) ≥65 1,707 443 (26.0) 1,264 (74.0) <0.001 Sex (n = 35,635 patients) Female 23,376 7,692 (32.9) 15,684 (67.1) Male 12,259 2,744 (22.4) 9,515 (77.6) <0.001 Race/Ethnicity (n = 35,631 patients) Non-Hispanic White 15,277 5,021 (32.9) 10,256 (67.1) Non-Hispanic Black 9,497 3,235 (34.1) 6,262 (65.9) Non-Hispanic Asian 8,068 1,509 (18.7) 6,559 (81.3) Hispanic 1,274 263 (20.6) 1,011 (79.4) Non-Hispanic Other/Multiple Races 1,144 312 (27.3) 832 (72.7) Declined to report 371 96 (25.9) 275 (74.1) <0.001 Language (n = 35,557 patients) English 18,528 6,195 (33.4) 12,333 (66.6) Spanish 8,528 2,869 (33.6) 5,659 (66.4) Chinese 1,553 184 (11.9) 1,369 (88.1) Vietnamese 1,980 618 (31.2) 1,362 (68.8) Arabic 1,806 326 (18.1) 1,480 (81.9) Other 3,025 199 (6.6) 2,826 (93.4) Declined to specify 137 29 (21.2) 108 (78.8) <0.001 Encounter level-information Visit type (n = 1,54,328 encounters)† Routine well visit (gyn/primary care) 34,244 6,022 (17.6) 28,222 (82.4) Routine follow up care (gyn/obstetrics/primary care) 80,303 13,581 (16.9) 66,722 (83.1) Procedure visit 13,973 1,030 (7.4) 12,943 (92.6) Urgent/walk in care/hospital 6,150 310 (5.0) 5,840 (95.0) Other (e.g. Dental/eye/mental health/nutrition/ specialty) 19,658 4,011 (20.4) 15,647 (79.6) <0.001 Telehealth (n = 1,54,342 encounters) No 1,29,388 24,392 (16.6) 1,22,607 (83.4) Yes 24,954 562 (7.7) 6,781 (92.3) <0.001 *Number of patients in each demographic domain may vary due to missing data.
↵†Number of encounters may vary due to missing data.
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Methods
- Results
- Discussion
- Limitations
- Conclusion
- Acknowledgments
- Appendices.Appendix 1. Provider/Staff Interview Guides and Provider Survey Tool
- Appendix 2. Background on Study Site Screening Practices
- Appendix 3. Survey Data Measures/Analyses
- Appendix Table 1. Survey Results Relevant to Screening Practices Across Four Study Sites (N = 97 Providers)
- Appendix Table 2. Demographics of Patients at Two Community Health Centers (CHCs) That Participated in Electronic Health Record (EHR) Data Analyses
- Notes
- References
- Figures & Data
- References
- Info & Metrics
Related Articles
Cited By...
- Clinician and Staff Perspectives on a Social Drivers of Health Program Implementation
- Adjusting Clinical Plans Based on Social Context
- Lingering Impact of COVID-19, Preventive Care Considerations, and US Health System Challenges
- Practicing Family Medicine in a Pandemic World: Lessons for Telemedicine, Health Care Delivery, and Mental Health Care