
Abstract
Background: Screening and referral programs for social isolation and loneliness in older patients increased during the COVID-19 pandemic in primary care settings to mitigate associated adverse health outcomes. This study explores community health centers’ experiences implementing a social isolation and loneliness screening program involving a community resource referral platform integrated into the electronic health record to support referrals.
Methods: A formative mixed methods evaluation in 4 community health centers. Semistructured interviews, observation of implementation meetings, facilitated group discussions, surveys, and utilization data extracted from the electronic health record and community resource referral platform were collected and analyzed concurrently.
Results: Screening for social isolation and loneliness can heighten health center staff knowledge and prioritization of socially isolated older patients. Participants indicate using an integrated community resource referral platform may only be useful in certain circumstances, particularly for those located outside urban areas. The experiences of these health centers indicate that when implementing interventions to mitigate patients’ social isolation and loneliness, it is necessary to consider other resource directories, needed adjustments to referral and documentation workflows, and potential impacts on patients and care teams.
Conclusion: Screening older patients for social isolation could increase care team awareness of social risk; assistance related referral options should be considered carefully.
- Community Resources
- Health Information Technology
- Loneliness
- Referral and Consultation
- Screening
- Social Determinants of Health
- Social Risk Factors
Introduction
Social isolation increased dramatically during the COVID-19 pandemic, particularly among older individuals,1 and even after vaccines became available, many older adults remained wary of interacting with people.2 Seclusion to avoid viral infection thus increased older adults’ risk of social isolation and loneliness (SI/L), which can negatively impact physical and mental health and substantially increase risk of mortality, a paradox between the risks and benefits of physical distancing.3⇓–5 These negative impacts are why SI/L are considered an adverse social determinant of health (ie, social risk) and why a 2020 (The National Academies of Science, Engineering, and Medicine) NASEM report on SI/L called for evidence on intervention strategies that can mitigate these risks.3
One way to support patients experiencing SI/L is by connecting them to community-based social service organizations (CBOs), but the difficulty of maintaining up-to-date lists or databases of organizations to which patients can be referred is well-known.6 One emerging strategy to mitigate this barrier involves using community resource referral platforms (CRRPs), which provide local and national databases of social service programs and resources.7,8 CRRPs are designed to streamline connecting persons with social needs to CBOs by providing a searchable resource database and supporting making referrals to these CBOs. In some cases, CRRPs also enable CBOs notifying the referring agency that the patient received support.
Screening and referral-making for SI/L and other social risks have been studied in the community health center (CHC) setting from the perspective of patients, clinical teams, and other impacted partners.9⇓⇓–12 Less is known about CHCs’ experiences with implementing SI/L screening programs involving a CRRP that is integrated into the electronic health record (EHR) to support related referrals. This study evaluated CHCs’ implementation of a CRRP-related SI/L screening and referral program.
Methods
A formative mixed methods evaluation13,14 was conducted between February 2021 and June 2022 to understand implementation and use of an SI/L screening program and EHR-integrated CRRP to support referrals in the CHC setting. The evaluation explored how the introduction of SI/L screening and the availability of the CRRP impacted care provided by CHC staff and barriers and facilitators to its use. Evaluation activities were reviewed by the OCHIN (not an abbreviation) Compliance Department and declared exempt from Institutional Review Board oversight.
Setting and Participants
This work was conducted at OCHIN, a nonprofit health IT organization hosting a central instance of the Epic EHR for more than 700 community-based clinics nationally. Most persons served by OCHIN member clinics live in households with income <200% of the federal poverty level; approximately 20% of this population have unmet social needs. One in 5 OCHIN member patients is aged older than 55, and nearly 1 in 5 patients self-report experiencing SI/L.
With funding from the American Association of Retired Persons Foundation, 4 OCHIN member CHCs (the pilot CHCs) implemented SI/L screening and an EHR-integrated CRRP to support related referral-making. Findhelp,15 the CRRP selected for these pilot efforts, was chosen because of its EHR integration functionality and because its free online search platform enables direct patient access. The integrated CRRP lets care team members identify relevant resources and make referrals from within the EHR. Such referrals may be sent electronically to CBOs, and referral information can be printed out for patients or shared via text message or e-mail. The platform listings are not limited to community resources; rather, they include nationwide resources to support regions with fewer CBOs. Notably, the CRRP relies in part on a crowdsourced model of requesting additions of new CBOs to their platform. CBOs are required to validate their organization’s information and provide permission to have their information listed in the CRRP.
CHCs were invited to take part in this project based on their interest in expanding access to social service resources and addressing SI/L among their older patients in the context of the COVID-19 pandemic. Participating CHCs came to the pilot with varying experience in systematically screening for social risks and using CRRPs. Each participating clinic identified at least 1 clinical champion and 1 project champion to coordinate and support project activities. CHC leaders and staff representing the 4 pilot CHCs participated in evaluation activities. Leaders were identified according to their ability to make organizational decisions about the CRRP implementation and workflows, and included roles such as medical director, program manager, quality improvement (QI) manager, and chief executive officer (CEO). CHC staff were defined as individuals working directly with patients and using the CRRP (eg, medical assistants (MA), community health workers (CHW), patient navigators, clinicians).
Two SI/L screening questions were developed for the purpose of the project by a study consultant with expertise in social isolation in older populations (ie, How often do you feel lonely? Are there enough people you feel close to and could call for help?). These questions were informed by language used in other social risk screening tools,16,17 and developed to be conversational so that they could be used flexibly (ie, alone or added to an existing tool).
Based on prior implementation research, each participating CHC received implementation support tailored to accommodate their unique setting and patient population.18 The content of this support ranged from help with developing and refining workflows for SI/L screening and using the CRRP, technical training in use of the CRRP, to facilitated discussions and decision making about adaptations to their screening programs. Once the pilot processes began, CHC staff were invited to attend regular facilitated peer-to-peer learning workgroups open to all participating CHC staff, monthly coaching calls for individual CHC staff, and CRRP office hours staffed by OCHIN practice coaches and CRRP staff.
Five data collection approaches were utilized for this evaluation of the implementation process and how it was adapted in each CHC.13,14 These included (1) semistructured interviews with CHC staff at 2 time points (Appendix 1); (2) observations of project check-ins with CHCs; (3) electronic survey of CHC staff focusing on CRRP training and use (Appendix 2); (4) facilitated group discussion; and (5) utilization data extracted from the EHR and the CRRP. Interviews, observations, survey, and group discussion were conducted and analyzed by RG and MP; EHR and CRRP utilization data were collected and analyzed by NM.
Qualitative data from interviews, field notes, and group discussion transcripts were analyzed using a rapid analytic approach.19,20 First, specific domains were identified that corresponded to pilot evaluation questions. Second, individual data collection episodes were summarized using a structured template containing the domains from the initial step; these summaries were transferred to a matrix by data collection type (eg, leadership interviews, staff interviews, field notes). Third, matrices were reviewed to identify themes, key points, and outlying phenomena across pilot sites. The fourth and final step was the development of summary documents based on findings highlighted in the matrices. These findings were shared with participating pilot health centers to provide participants with the opportunity to react to the interpreted data and further strengthen the validity of the findings.21
Quantitative data including longitudinal EHR and CRRP utilization data were analyzed using descriptive statistics.22 Survey data were analyzed similarly to summarize individual variables and uncover patterns. Qualitative and quantitative findings were reviewed concurrently by the larger project team (RKG, MP, NM, RG, MB, MV) to compare, contrast, and interpret the data using a convergence model of triangulation design to combine methods, allowing a deeper understanding of the CRRP intervention by triangulating findings from the respective analyses.23 Qualitative and quantitative findings were reviewed concurrently by the evaluation team, implementation team, and project leadership team to compare, contrast, and interpret the results leveraging the expertise of the cross-disciplinary team and participants to yield complementary insights. The mixed methods analyses were conducted during a series of team discussions and served to highlight drivers and barriers of SI/L screening and CRRP implementation.
Results
The pilot CHCs screened 4646 adult patients aged 50 and above during the study period (January 2021–June 2022). Of those, 963 indicated feeling SI/L and 174 referrals were made through the EHR-integrated CRRP.
Nine preimplementation interviews were conducted with 15 individuals and 11 postimplementation interviews with 18 individuals. Observations were conducted throughout the clinics’ pilot processes, including at the project kick-off meeting, monthly coaching and training sessions (n = 46), CRRP office hours (n = 6), and peer support meetings (n = 4). Representatives from all health centers participated in the survey and group discussion. Table 1 outlines study participation and timeline by CHC and role.
Participant Engagement and Timeline
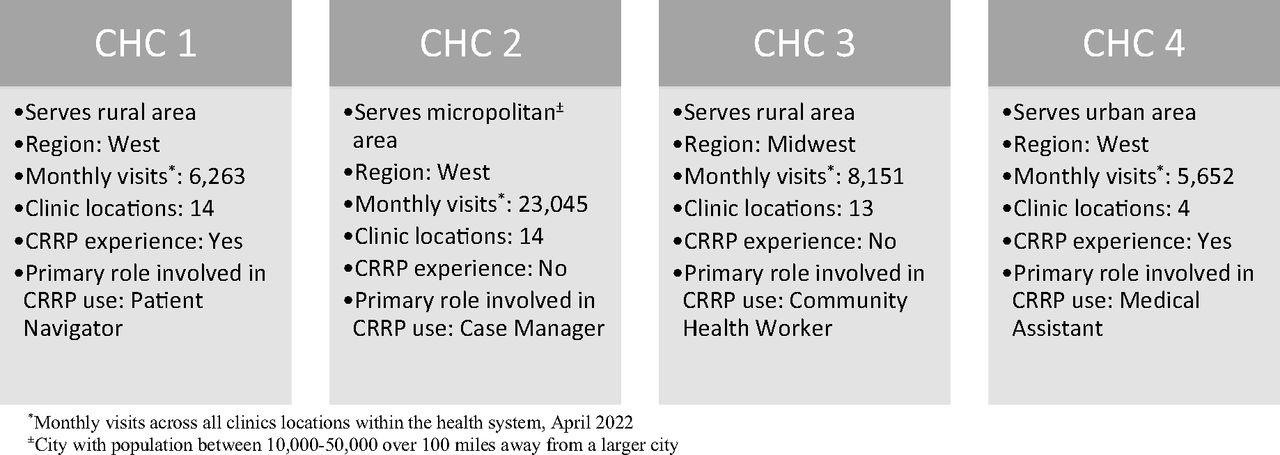
With the implementation support described above, the CHCs adjusted workflows as needed and prioritized patient populations for screening. Each CHC approached their SI/L screening and referral program implementation differently but shared overlapping characteristics with other pilot CHCs, including region, rurality, and prior CRRP experience. A snapshot of each CHC profile is presented in Figure 1. All pilot CHCs are federally qualified health centers and have been on OCHIN Epic for at least a decade.
Participating CHCs reported being satisfied with their involvement in this pilot because it heightened their knowledge of and enabled prioritizing the support of socially isolated older patients. They perceived that the CRRP created efficiencies during patient encounters when the CRRP had relevant CBO information. A significant barrier identified by CHCs located outside of urban regions (in this case, 3 of 4 CHCs) was a lack of available CBOs in the CRRP. Participants perceived that this was related to 2 factors: (1) limited CBOs in rural regions with which to populate the CRRP, and (2) lack of clinic capacity to provide the crowdsourcing support to suggest CBO additions. Staff from these rural CHCs indicated the CRRP was occasionally useful, particularly if they needed to search for CBOs located in urban areas (ie, if a patient were moving or needed to travel to a different location). This finding is reflected across qualitative data and survey results. Case studies exploring each CHC’s unique approach, success, challenges, and postpilot plans are described below.

Participating community health center profiles. Abbreviations: CRRP, Community resource referral platforms; CHC, Community health center.
CHC 1 Case Study
Located more than an hour’s drive from the nearest city, CHC 1 is in a rural town of roughly 500 people, of whom the majority are more than 65 years old. The CHC has provided affordable health care to the community since the 1970s and the staff have long-established relationships with their patients. Their leaders were interested in participating in this pilot effort because of their largely older – and potentially isolated – patient population. This clinic had several years of prior experience screening for social risks and providing community referrals involving a CRRP other than findhelp and lacked EHR integration.
Clinic staff started screening for SI/L and using the CRRP within 2 months of the initial training provided for the pilot study. Their workflow typically started with a article-based screening questionnaire handed to patients by front desk staff or a medical assistant. Because this health center already had substantial experience and an established workflow screening for social risks in adult patients, they incorporated the SI/L questions into their existing approach. For patients indicating social isolation, a transfer of care was made from the care team member initiating screening to a patient navigator tasked with identifying an appropriate CBO. Referrals for CBOs were typically provided directly from the patient navigator to the patient, either via phone call or mailed letter. The patient navigator documented referral information in the EHR and subsequently updated the chart with the referral ‘outcome’ (ie, whether the patient received the services to which they were referred), if they had time to ask the CBO or patient about their referral. During the study period (January 2021–June 2022), CHC 1 administered 1754 SI/L screening questionnaires to patients aged 50 and older. Of those, 694 indicated experiencing SI/L. Seventeen referrals were placed through the EHR-integrated CRRP, indicating their preference for making referrals through different means, as described below.
Seeking to engage as many patients as possible early in the pilot, CHC 1 developed a bilingual postcard with information about SI/L and a QR code that linked to the free CRRP website, which patients could use to look up CBOs. The clinic faced significant staffing shortages during the pilot period, requiring periodic closures. Clinic staff also found using the CRRP to be challenging due to 2 related issues: 1) there was limited availability of CBOs in their region, and 2) of those available, none were listed in the CRRP. The lack of known CBOs in the CRRP could be due to a breakdown in any of the steps to add a CBO outlined above (ie, CRRP staff exploration, clinic resource request, CBO validation process). Despite the clinic manager’s efforts to encourage their local CBOs to add their information to the CRRP, no new CBOs materialized in the database, which restricted the CHC’s ability to place referrals using the CRRP. Participants reported that the perceived impact on care was limited. The clinic manager shared,
We just need the resources to be there so [the CRRP] is worth using. Because right now we’re kind of separated into multiple workflows because we don’t have all the resources in [CRRP]. We’re like, “well if you can’t find it here then you need to start here and go here.” If we had everything in one location, then we could have one solid workflow for it.
As a result of these barriers, CHC 1 opted to continue screening for SI/L but discontinue their use of the EHR-integrated CRRP after the pilot period ended. They chose to use the free unintegrated, web-based version of the CRRP, but only in instances where it was useful a (eg, for a patient asking for resources in neighboring zip codes). CHC 1 now primarily relies on their clinic staff’s local knowledge of available resources and internally maintained list of resources to refer patients, which was the system they relied on before CRRP integration.
CHC 2 Case Study
CHC 2 serves patients in 2 counties in a geographically isolated area. Founded in the early 1970s to provide health care access to surrounding rural logging communities, CHC 2 had strong leadership support for this effort. Implementation of SI/L screening and integrated CRRP began 7 months after the pilot start date. Activities focused primarily on designing, building, and implementing a social risk screening program, and an intern was engaged to add and/or update CBO listings in the CRRP. Because social needs screening was new to this organization, they kept their screening and referral workflow small in scope by limiting it to a single care team member. The case manager screened for SI/L in case management office visits for all patients aged 50 years and older, then utilized the CRRP or their own local knowledge to refer patients to community resources. Both resource referrals were provided to patients by way of verbal or written CBO information, with the referral information being documented by the case manager in the patient’s record. The case manager then systematically called patients or CBOs to confirm that the patient received the services to which they were referred and documented this in the EHR. During the study period CHC 2 administered 84 SI/L screening questionnaires to patients 50 and older. Of those, 69 indicated experiencing SI/L. Thirty-six referrals were placed through the EHR-integrated CRRP but is not comprehensive of the different ways they made referrals, described below.
CHC 2 participants perceived the integration of the CCRP in the EHR to impact patient care favorably by creating efficiencies, yet they experienced challenges related to competing demands, staff turnover, and the considerable effort to populate the CRRP with CBOs. One leader reflected on the work their intern did to populate the regional offerings in the CRRP,
As lovely as the platform sounded at the very beginning, until we had a person that could do this work, it was a real point of discussion if we should participate. It took [the intern] a lot of time to call these organizations. A lot of CBOs have one or two people that work at them, so they don’t have time themselves to call him back and flesh out all the questions that he has and upload and verify their information in [the CRRP].
Due to these barriers and the burden placed on the Case Manager, CHC 2 delayed a larger clinic-wide rollout of their new screening and referral workflows and chose not to use the EHR-integrated CRRP after the pilot period ended but continued to screen for SI/L and provide referrals mostly based on local staff CBO knowledge.
CHC 3 Case Study
CHC 3 has a catchment area covering a patient population on >20,000 square miles, with small towns dispersed throughout. Started by volunteers to provide health care access to underserved communities, CHC 3 had strong leadership support in raising clinic staff awareness of social isolation risks among older community members. This CHC implemented SI/L screening and referral workflows approximately 3 months after their initial training, which was conducted by 1 care team member, a community health worker (CHW). As they had only just started a social risk screening program, their implementation approach was smaller in scope. In most cases, referrals were made by the CHW copying CBO information from the CRRP and pasting it into a document which was printed and shared with patients. Referral information was documented in the patient chart, and the CHW followed up with the referred patient or CBOs about referral outcomes, as time allowed. During the study period CHC 3 administered 243 SI/L screening questionnaires to patients 50 and older. Of those, 118 indicated experiencing SI/L. Thirty-four referrals were placed through the EHR-integrated CRRP.
CHC 3 faced barriers related to limited CBOs in their rural community, and of those CBOs, contact information was either outdated or missing entirely from the CRRP. Of CBOs listed in the CRRP, many did not accept referrals through the CRRP, which rendered the CRRP less useful. A CHW at this CHC commented,
I am finding not all [CBOs in the CRRP] accept referrals from other organizations. I don’t know … who makes those decisions to say yes, we accept referrals, and these are the workflows we need set up in order to accept referrals … And so I guess when I participated in this pilot, I didn’t think that even if they’re searchable, doesn’t mean they’re going to accept referrals.
Throughout the pilot period, this CHC continued to conduct SI/L screening. Participants shared that the most noticeable impacts on patient care were that it saved time when patients needed referrals outside the CHC’s region. However, due to the drawbacks with the CRRP described above, they often used other resources such as a clinic-developed directory or staff knowledge to identify CBOs. They discontinued use of the integrated CRRP at the end of the pilot period but planned to continue to screen for social risks and use the free web-based version of the CRRP to search for CBOs outside of their region for patients requesting it. For patients requesting referrals locally, CHC 3 transitioned back to using staffs’ local knowledge and their health center-maintained CBO directory.
CHC 4 Case Study
CHC 4 is located in a predominantly agricultural community close to a large metropolitan area. This CHC system was created in the 1970s to provide health care access for the community’s agricultural workers, and it continues to serve these workers and others in the region. This CHC had prior experience screening patients for social risks and referring them to CBOs via a nonintegrated, regionally focused CRRP. CHC 4 participated in the pilot because their CRRP platform was being phased out, and they were motivated to try a CRRP that could interface directly with the EHR. Implementation began 7 months after the pilot started in all clinics in their health system. This health center had experience screening for social risks and decided to add the SI/L questions to their existing screening instrument and workflow. CHC leadership also arranged staff trainings in motivational interviewing techniques for those involved in screening and providing referrals to patients for SI/L. During the study period CHC 4 administered 2565 SI/L screening questionnaires to patients 50 and older. Of those, 82 indicated experiencing SI/L, all of whom received referrals placed through the EHR-integrated CRRP.
Medical assistants provided the SI/L questionnaire to the patients during rooming at an office visit, reviewed the results with the patient, and offered to connect them with a navigator for additional support. If desired, the navigator met with the patient during the visit and provided referrals to CBOs by way of printed CBO information from the CRRP and sometimes via text, if requested by the patient; alternately the navigator would call the patient if they were unable to see them during their office visit to share referral information verbally or via text message. Referrals were sparsely made directly through the integrated CRRP, more often going to patients directly for them to contact the CBO. The Navigator documented referrals in the patient chart but would generally not conduct follow-up related to the referral. The CHC appreciated the focus of SI/L during the COVID-19 pandemic. A member of leadership shared,
If there’s a silver lining to the pandemic, it’s made it socially acceptable to be lonely … For our seniors that have been isolated by the pandemic, they’re all universally feeling the loneliness of the pandemic, so somebody asking about that … There’s not as much stigma anymore. So, saying that there’s something that we can do about it and that we can help connect you to others is sort of a relief for some people.
CHC 4 faced fewer challenges in searching for CBOs in the CRRP, in contrast to the other pilot locations, due to their location near an urban center with access to more CBOs, and more populated CRRP. Participants perceived that use of the CRRP impacted the care they provided by streamlining referrals and ensuring that patients could quickly access needed information. They were the only pilot clinic that chose to continue screening for SI/L and also continue to use the integrated CRRP beyond the pilot period, and when it ended, they began looking into building reporting and interoperability functionality to their CRRP.
Discussion
Four CHCs implemented an SI/L screening and referral program including using an EHR-integrated CRRP to make referrals. Results suggest that screening for SI/L may heighten knowledge and prioritization of socially isolated older patients at CHCs, but using an integrated CRRP may only be useful in certain circumstances.
One theme of these results is that CRRPs are not a panacea for every health center, which aligns with other recent research findings about social needs referrals in general.7,24,25 In some cases, a CRRP might be the primary method of referral provision, whereas some may use it to augment other CHC-preferred referral approaches. For example, CRRPs may be used as a technological enhancement, but do not replace knowledgeable care team members and relationships between organizations. In addition, the CHCs encountered challenges to using the CRRP, such as ensuring that local CBO listings are available and accurate, and the lack of an efficient way to document and track referrals systematically. CHCs interested in adopting a similar screening and referral program could investigate different options that support community referrals, in addition to different CRRP choices to determine the best fit for their needs and communities. Other options may include CBO notebooks or spreadsheets that are developed and maintained in clinics and may be used instead of or in combination with a CRRP, particularly in locations with limited CBOs or sparsely populated CRRP directories. Relying on health center staff to maintain their own resource libraries or databases requires time and effort but may be preferable for clinics for whom a CRRP is not as practical.
Study findings suggest promising practices for health care organizations interested in implementing SI/L screening and referrals. First, before investing in a CRRP, health centers may wish to consider all options for CBO identification and referrals, including researching whether local CBOs are listed in the CRRP directory. If local CBO options are lacking or not listed, an EHR-integrated CRRP may be of limited value unless CBOs are willing to validate their information with the CRRP or clinics submit requests to add known CBOs. Clinic-based notebooks, binders, spreadsheets, brochures, web-based directories, and care team local knowledge can also be used.
Second, health centers may consider developing an implementation plan that takes into account needed workflow revisions and potential care team, CBO, and patient impacts. In addition to deciding on a method to identify CBOs and provide referrals, considerations include how to document referrals, the role(s) of care team members, and how these changes can be evaluated to show improvement. Moreover, pilot CHC staff professed a lack of confidence at times when talking with patients about this potentially sensitive topic. Future research could examine how best to train clinic staff in effective, empathetic communication strategies specific to SI/L and how to tailor such dialog (and assistance options) to a patient’s unique circumstances.
This study is limited in its generalizability due to its small sample size of 4 CHCs. We mitigated this by sampling CHCs with diversity of rurality, patient populations, and history of social needs screening, referrals, and CRRP use. In addition, using the case study approach enabled an in-depth, nuanced look at this complex topic in a real-world setting.26 Future research could explore a larger, more diverse sample of health centers and platforms and incorporate the patient perspective. Finally, referrals for SI/L were only able to be tracked using discrete EHR data, resulting in a probable undercount of total referrals.
Conclusion
This study highlights the implementation of a SI/L screening program and integrated CRRP in CHCs. The 4 pilot sites approached their implementation and use in varying ways, but similar barriers and facilitators were discovered across all sites. Findings indicate that CRRPs are not a remedy for all older adults experiencing social isolation and loneliness but may be useful in combination with other solutions. Moreover, CRRPs may not be useful for CHCs without an upfront investment to ensure they have adequate CBO information before implementation. Regardless of a CHC’s referral approach, this study emphasizes the importance of screening for SI/L to heighten CHC staff knowledge and prioritize support for socially isolated older patients.
Acknowledgments
The authors appreciate the participating CHCs. We would also like to thank Julianne Bava, Miguel Alvarez, and Teresa Weir for their support of the CRRP pilot implementation, and Dr. Matthew L. Smith for his expertise in social isolation and loneliness in older adults.
Appendix 1. Clinic Staff Interview Guide
Appendix 2. CRRP Survey
Notes
This article was externally peer reviewed.
Funding: This study was supported by the AARP Foundation (ISO-2020-05-001). The content provided is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Conflict of interest: The authors report no conflicts of interest. The study sponsor did not play a role in the study design or the submission of this manuscript.
Implementation of Social Isolation Screening and an Integrated Community Resource Referral Platform
To see this article online, please go to: http://jabfm.org/content/36/5/803.full.
- Received for publication February 11, 2023.
- Revision received April 28, 2023.
- Accepted for publication May 8, 2023.




{kind=link}