
Abstract
Introduction: An ongoing patient-physician relationship may increase the likelihood of acknowledging obesity and providing a treatment plan. The purpose of the study was to investigate if continuity of care was associated with recording of obesity and receipt of a weight-loss treatment plan.
Methods: We analyzed data from the 2016 and 2018 National Ambulatory Medical Care Survey. Only adult patients with measured body mass index of ≥ 30 were included. Our primary measures were acknowledgment of obesity, treatment of obesity, continuity of care, and obesity-associated comorbid conditions.
Results: Among patients who were objectively obese, only 30.6% had an acknowledgment of the patient's body composition in the visit. In adjusted analyses, continuity of care was not significantly related to recording of obesity but did significantly increase the likelihood of treatment for obesity. Continuity of care was only significantly related to obesity treatment when defined as a visit with the patient’s established primary care physician. The effect was not seen with continuity with the practice.
Discussion: There are many missed opportunities for prevention of obesity-related disease. Continuity of care with a primary care physician was associated with benefits in treatment likelihood, but greater emphasis on managing obesity in a primary care visit seems warranted.
- Chronic Disease
- Health Care Surveys
- National Ambulatory Medical Care Survey
- Obesity
- Primary Care Physicians
- Primary Health Care
Obesity is a major cause of morbidity and mortality worldwide and has been associated with increased risk for the development of a wide variety of diseases including cardiovascular disease, diabetes, osteoarthritis, and cancer.1,2 Most concerning, increasing obesity has been clearly linked to increased risk for both disease-specific and all-cause mortality.3,4 Adults with a body mass index (BMI, calculated as weight in kilograms divided by height in meters squared) greater than or equal to 30 kg/m2 are considered obese, and obesity is further divided into 3 stages by BMI cutoff points: stage 1 (>30 kg/m2), stage 2 (>35 kg/m2), and stage 3 (>40 kg/m2). These stages have implications for disease prevalence and all-cause mortality, specifically with increasing rates of all-cause mortality at higher stages of obesity.4 Improving disease prevention and health promotion is relevant to improving population health, so obesity recognition and discussion of behavioral interventions for obesity is a major public health concern.
Many adults in the United States are obese. In 2017 to 2020, 42% of adults were obese based on BMI.5 Some racial/ethnic groups have a particularly high prevalence of obesity. Non-Hispanic Black women have the highest race/gender prevalence with 58% being obese. Effective strategies to prevent obesity and lose weight exist, but for patients to perceive themselves as at risk of obesity-related disease, it is important that their physicians acknowledge them to be obese.6 Moreover, when physicians acknowledge that a patient is obese, these patients are then significantly more likely to discuss weight loss with their doctor during the visit.7 Further, outlining a treatment plan to assist with weight loss and a healthy diet is particularly important to help these patients. The US Preventive Services Task Force recommends that clinicians offer or refer adults with a BMI of 30 or higher to intensive, multicomponent behavioral interventions.8
An ongoing patient-physician relationship is an important component in the delivery of effective medical care and is a hallmark of primary care. Continuity of care has shown numerous benefits in various health outcomes.9⇓–11 The development of mutual trust between patient and physician is part of that relationship. It has previously been shown that patients with obesity rate clinicians higher in honesty and trust when the clinician discussed weight-related healthier lifestyles with them.7
We investigated in a nationally representative collection of primary care physician visits whether patients with obesity who had continuity of care would be more likely to have the obesity recorded and whether they were presented with a weight-loss treatment plan.
Methods
We analyzed data from the 2016 and 2018 National Ambulatory Medical Care Survey (NAMCS), a national probability sample survey of ambulatory medical care visits to office-based physicians that allows for national estimates regarding US medical care. These 2 databases are the most current ones available for primary care visits in the United States. The National Center for Health Statistics reported problems in collecting the 2017 data, and so the 2016 and 2018 datasets were the most currently available. This publicly available, deidentified dataset meets the National Institutes of Health and institutional review board exemption as not human subjects. The study was focused on adults aged 18 and older. The sampled visits were to a primary care physician. Primary care was determined by the physician specialty coded in the NAMCS. More information on the NAMCS design and variable definitions can be found in their documentation files.12,13 A total of 1,623 visits were available for analysis, and when these visits are weighted for the population and the analysis controlled for the complex sampling design, they represent 101,432,875 office-based primary care and ambulatory medical care visits in the United States. We focused on persons ages 18 and older whose BMI computed from height and weight in the visit was ≥30 kg/m2.
Measured Obesity
BMI was calculated from patient’s height and weight recorded during the NAMCS visit. BMI was not calculated for pregnant females, patients under age 2, or patients with a recorded height and/or weight that fell outside of acceptable ranges. Persons with BMI ≥30 kg/m2 were considered to be obese.
Independent Variable: Continuity of Care
The relationship and trust that develops between a patient and a physician may impact the likelihood of acknowledging obesity or providing a treatment plan. The NAMCS contains the following 2 questions asked of the participating physicians filling out the form: “Are you the patient’s primary care provider?” and “Has the patient been seen in this practice before?” For encounters in which the physician specified that he/she is the primary care provider and the patient is an “established patient,” we classified this visit with the established primary care physician as having continuity of care with the patient. Further, the number of primary care physician visits in the past 12 months was also included in the analysis as an additional independent variable of continuity of care with the practice, or informational continuity.
Outcomes: Recorded Obesity
There were 2 options for the physician to record obesity. The first was to record it as a diagnosis code associated with the visit. The International Classification of Disease-10 (ICD-10) codes for BMI of Z68.30-Z68.45 correspond to BMI of 30 or higher. Similarly, the ICD-10 code for obesity is E66. The visit has diagnosis codes for a primary diagnosis and up to 5 diagnoses in the visit. The second option was for the physician to indicate a comorbid condition that was not the reason for the visit or the diagnosis. The NAMCS has a list of comorbid conditions including obesity.
Outcomes: Health Education/Counseling Treatments for Obesity
In the NAMCS, physicians have a list of potential health education/counseling treatments that they recommended during the visit. Treatments that would be consistent with behavioral interventions for obesity were “diet/nutrition,” “exercise,” and “weight reduction.” If any of these were checked, the patient was considered to have a treatment recommended at that visit.
Demographics
Patient race, Hispanic/Latino ethnicity, age, sex, and source of payment for the visit (eg, private insurance, public insurance, self-pay) were all collected during the visit.
Comorbid Conditions
Comorbidities that may increase the likelihood of acknowledging obesity or providing a treatment plan: type 2 diabetes, hypertension, hyperlipidemia, history of stroke, coronary artery disease/history of myocardial infarction, congestive heart failure, arthritis, obstructive sleep apnea, chronic obstructive pulmonary disease, chronic kidney disease. All of these conditions are included in the list of comorbid conditions supplementary to the recorded diagnoses. Further, we looked for these comorbid conditions in the list of diagnoses for the visit. The ICD-10 codes were E11, I10, E78, I25, I50.2, M19, G47, J44.9, and N18.
Statistical Analysis
To account for the complex sampling design of the NAMCS, we used SAS software version 9.4 (SAS Institute, Cary, NC) for all analyses. The weighting and strategies accounting for the complex sampling design allowed the analysis to provide nationally representative estimates. All presented results are weighted accounting for the complex sampling design. We used chi-squared analyses to compare acknowledgment of obesity and treatment with demographic characteristics (eg, race and sex) and the number of comorbid conditions by the status of continuity of care. We then examined the relationships between continuity of care and selected individual characteristics using multivariable logistic regression analysis. We further conducted logistic regressions to examine the impact of race, gender, comorbidities, and continuity of care on the acknowledgment of obesity and the likelihood of receiving treatment. In subgroup analyses, following the same approach, we fitted 2 separate multivariable logistic regression models to test associations of the number of primary care physician visits with the 2 outcomes among those patients with continuity of care: including the number of visits as a continuous variable in model 1 and as a categorical variable (by quartile level) in model 2. Listwise deletion was used in cases with missing data. All tests were 2-sided at the significance level of 0.05.
Results
Our final study sample of ambulatory primary care visits with an objectively measured patient with obesity consisted of an unweighted sample of n = 1,623 visits representing a US population estimate of 101,432,875 visits. In the pool of visits among patients who were objectively obese, only 30.6% (weighted n = 31,079,959 visits) had a recording of the patient's obesity. In terms of treatment, of those who had obesity recorded, 40.3% received a treatment plan for weight management. Of those visits where the obesity was not recorded, 21% received a treatment plan suggesting that some patients were receiving treatment and a tacit acknowledgment of their obesity. In total, 26.9% were receiving some weight-management treatment plan whether or not the obesity was recorded.
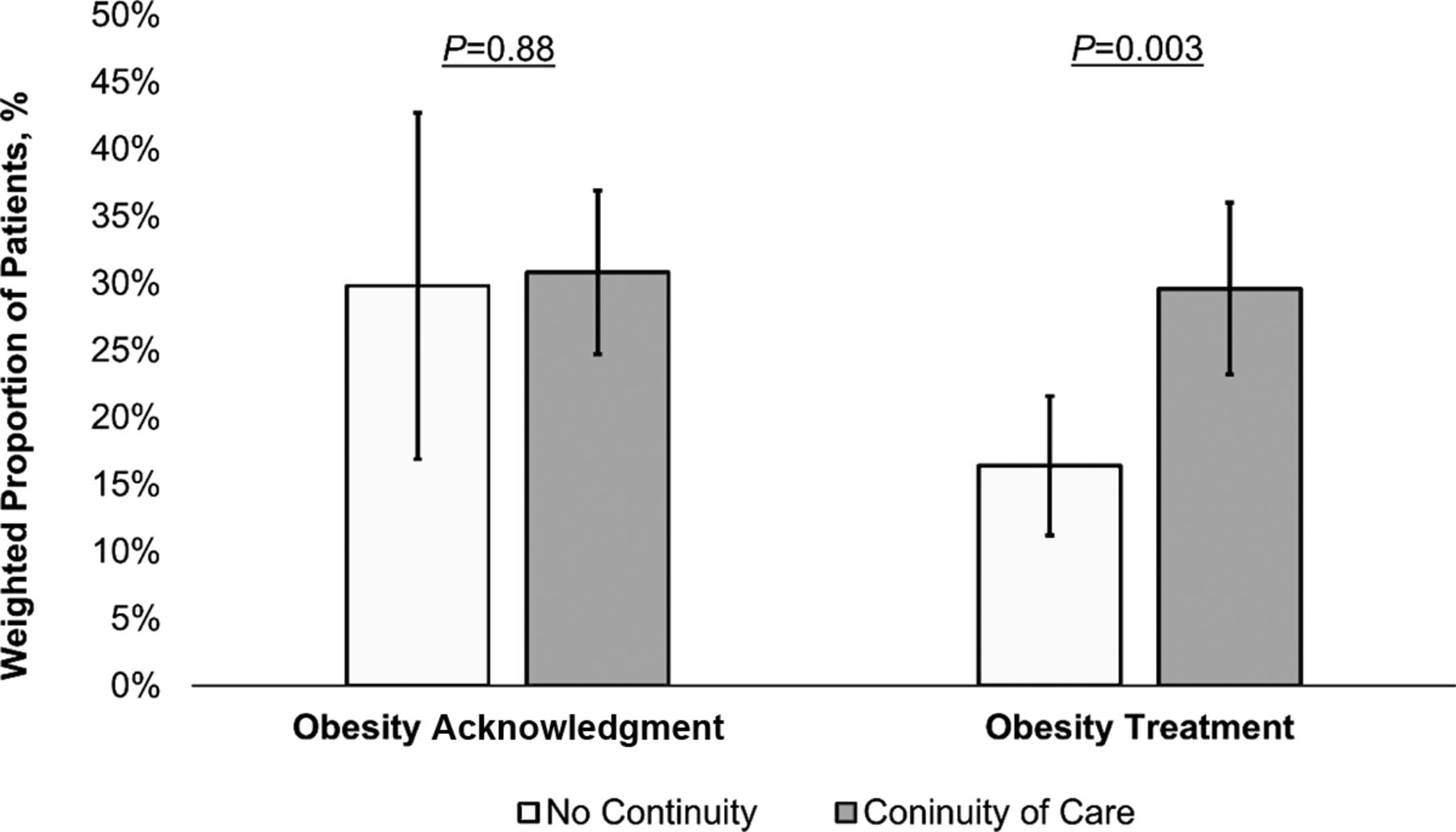
The characteristics of the population are presented in Table 1. Overall, 84.6% of patients reported having continuity of care. Patients with continuity of care are more likely to be older, male, have public health insurance, and have more chronic conditions than those without continuity of care (all P < .05). In the multivariable regression analysis, sex, payment type, and the number of chronic conditions are significant predictors of continuity of care (all P < .05). Figure 1 illustrates the weighted prevalence of obesity acknowledgment and treatment by the presence of continuity of care.

Weighted prevalence of recorded obesity and obesity treatment by continuity of care in primary care visits.
Sample Characteristics of Primary Care Visits by Continuity of Care (n = 1,623, Weighted n = 101,432,875)
Table 2 shows the associations of continuity of care with obesity recording and treatment. Patients with continuity of care were more likely to report receiving obesity treatment compared with those without continuity of care (OR 2.08, 95% CI, 1.23-3.51), whereas there is no significant relationship between continuity of care and recording of obesity. In addition, after adjusting for other characteristics, a higher BMI and more weight-related chronic diseases were significantly related to both recording and treatment of obesity. Patients who had their obesity recorded were more likely to receive an obesity treatment plan compared with those who did not. This relationship was present in both a crude (OR 2.55, 95% CI, 1.56-4.16) and adjusted analysis (OR 2.38, 95% CI, 1.46-3.88).
Association of Continuity of Care with Recorded Obesity and Obesity Treatment in Primary Care Visits
Table 3 presents the multivariate logistic regressions for the likelihood of patients with obesity having their obesity recorded and treated among those with continuity of care. In model 1, each additional increase of 1 visit was associated with a significant increase in the odds of a patient having their obesity recorded (OR, 1.04, 95% CI, 1.01-1.07). In model 2, patients who had more than 6 visits in the past year were significantly more likely to report recording of obesity than their counterparts who had ≤2 visits (OR, 1.86, 95% CI, 1.14-3.04). However, the number of visits was not significantly associated with receiving obesity treatment.
Subgroup Analysis: Association of Frequency of Visit with Recorded Obesity and Obesity Treatment Among Patients with Continuity of Care
Discussion
Although all of these patients were objectively obese and thus all should have had their obesity recorded and addressed with a treatment plan, the results of this study suggest that there are many missed opportunities in primary care to diagnose and treat obesity. In fact, in only slightly more than a quarter of the visits (26.9%) in which the physician recorded height and weight that classified the patient as obese did the physician offer a weight-management treatment plan. This is evidence of a huge missed opportunity for prevention of a wide range of diseases. Moreover, there may be an upward norming of obesity in the minds of primary care physicians. The threshold to move the physician toward action seems to be much higher than a BMI of 30.
It is important to recognize that having continuity of care with a primary care physician was associated with a greater likelihood of patients with obesity receiving treatment recommendations for their obesity. This may reflect increased trust between the physician and patient and more comfort in discussing a potentially difficult and stigmatized subject. Obesity is stigmatized in society, and so having a positive patient-physician relationship may increase uptake of therapeutic interventions.
Primary care physician behavior is also being driven by clearly risk-associated variables. Higher BMI values and an increased number of obesity-related illnesses increase the likelihood that obesity is acknowledged and treated. This is likely due to the increased disease burden experienced by patients, which provides motivation to discuss obesity and weight-loss interventions, along with the evidence of higher immediate morbidity and mortality risk, which prompts physicians to intervene.7 Evidence that clearly suggests higher mortality risk associated with higher BMI values is likely also prompting physicians to address obesity more aggressively for patients with higher BMI values.8
Although minority populations have a relatively higher prevalence of obesity, we found no evidence of a health disparity in the delivery of primary care regarding recording of obesity by clinicians or delivery of treatment recommendations.5 This finding is reassuring and suggests that clinicians are relying on objective criteria (BMI values and presence of comorbid conditions) rather than subjective factors when determining the delivery of care and recommendations related to obesity. However, with such a low rate of physician recording or treatment of obesity for all patients, this suggests that the threshold for action has been normed upward, missing the opportunity for prevention in many eligible patients.
Conversely, our findings demonstrate that recording of obesity and discussion regarding weight/lifestyle management is not routinely happening in ambulatory care settings, overall. This is a subject of significant concern, given that obesity is strongly correlated with the development of a wide variety of major health conditions, particularly with all-cause mortality.3,4 As our main analysis showed, it is possible for providers to prescribe the treatment without recording obesity. Although having more frequent provider visits was associated with higher odds of having the obesity recorded, receipt of obesity treatment was more likely if patient’s obesity was recorded regardless of continuity of care. Considering that chances of diagnosing increase with the number of visits, it is not surprising that this is the case. More concerning is that this may also suggest that some patients with obesity may have missed opportunities to receive effective care at earlier stages of their continuity of care. Many primary care physicians have reported limited time and insufficient training to engage patients in obesity and weight-management discussion.14 Further, it may be that prevention and obesity management may not be a priority for a patient with a different presenting complaint or reason for visit. There would be little time in a typical doctor’s appointment (15 to 18 minutes) for discussing obesity or lifestyle choices unless obesity or obesity-related condition is the primary reason for a visit.15 In addition, inadequate reimbursement for obesity treatment may influence the recording or recommendation for treatment for patients with obesity. Perhaps simply communicating BMI levels or discussing obesity as a cardiovascular risk factor at each visit might be effective strategies. Future studies are needed to investigate what potential barriers primary care providers may face when treating and strategies to address them (eg, documentation burden, reluctance to label patients as obese).
This study has several limitations that need to be acknowledged. First, the data collected in the NAMCS are derived from patient visits and not individual patients, so it is possible for the same person to make multiple visits. However, since NAMCS only collects data on a random week of visits, it is unlikely that the same patient visited the same provider multiple times in a single week. In addition, because of this limited data collection period, follow-up visits and detailed records of other obesity treatments (eg, history of bariatric surgery) are unavailable in NAMCS. It is still possible that the diagnosis of obesity and its treatment could have occurred during another visit. Second, some clinicians may have explicitly discussed obesity with patients, recommending weight loss and lifestyle changes, but failed to include a specific diagnosis code or checked the comorbidities or treatments listed on the survey form. Based on the standardized form and the training required for clinicians to participate in the NAMCS, that would be expected to be a low-likelihood event. There is evidence that some physicians recommended treatment without an explicit acknowledgment, but it should be unlikely that both acknowledgment and treatment would both be missing if it happened. Third, the NAMCS has limited information on practice characteristics. Physicians’ participation in incentive programs (eg, pay for performance or other value-based care programs) may have influenced their obesity-related documentation and coding practices (eg, risk population management). Again, since the NAMCS uses a standardized survey form and is not an analysis of what was placed in the electronic medical record (EMR), coding practices in the EMR would be unlikely to affect the data collected in the survey. Finally, although we have studied the delivery of obesity-related counseling and treatment plans to patients, there is no ability with this dataset to determine the effectiveness of these plans in actually affecting patient behaviors and BMI levels.
In conclusion, obesity has major implications for patients’ health, particularly in association with increasing risk of chronic health conditions and higher all-cause mortality. It is important that primary care clinicians address obesity at routine office visits and that they provide treatment recommendations regarding obesity management, including discussions of diet and lifestyle changes to achieve optimal health. These discussions are not happening routinely at office visits with US primary care providers, per our analysis, and they are more likely to occur when patients have multiple obesity-related comorbidities or at higher stages of obesity, or in the context of an established physician-patient relationship. This suggests that the United States needs a stronger network of primary care physicians with longitudinal physician-patient relationships and that physicians need to be more aggressive in treating obesity before chronic conditions occur.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: The authors have no conflicts of interest.
Data availability: The data used in this study are from public use databases (National Ambulatory Medical Care Survey) freely available from the National Center for Health Statistics.
To see this article online, please go to: http://jabfm.org/content/36/2/325.full.
- Received for publication August 31, 2022.
- Revision received November 8, 2022.
- Accepted for publication November 14, 2022.




{kind=link}