
Abstract
Introduction: The COVID-19 global pandemic has affected all ethnic and minority groups although not equally. The goals of the present study are twofold: describe the diverse COVID-19-related care needs Hispanic patients presenting to a primary care facility and the symptom clusters and socioeconomic factors that may impact their wellbeing.
Methods: This is a retrospective cohort of Hispanic patients in an outpatient clinic serving an urban lower socioeconomic demographic, between May 9 and July 31, 2020. COVID-19 infection was confirmed by polymerase chain reaction or rapid antibody test. Student's t-test was used for means and the chi2 was used for comparisons of proportions.
Results: A total of 6616 patients visited Alivio, 409 were triaged to a containment area, and 378 were tested for COVID-19; 230 with, 148 without symptoms. Of those tested, 161(42.6%) were positive, representing 2.4% of total patients seen. Age, temperature, and pulse rate were all significantly higher in patients with symptoms compared with those without. Symptoms were grouped into 5 clusters: constitutional, n = 143(62%), respiratory, n = 136 (59%), and somatic, n = 97(42%) were most common. No single cluster was particularly diagnostic of COVID-19, although those with symptoms in multiple clusters were more likely to test positive, P < .001. The majority worked in essential jobs, were uninsured, and had more than half had prolonged symptoms.
Conclusions: Hispanic patients have diverse reasons for seeking health care and for testing in a pandemic. COVID-19 is a syndromic disease as evidenced from the clustering of symptoms. Essential workers and uninsured health status may lead to more prolonged disease course.
- Cluster Analysis
- COVID-19
- Healthcare Disparities
- Hispanics
- Minority Health
- Outpatients
- Pandemics
- Primary Health Care
- Retrospective Studies
- Socioeconomic Factors
- Triage
- Underserved Populations
Introduction
SARS-CoV-2, designated COVID-19 by the world Health Organization, is a novel coronavirus responsible for the current global pandemic that has severely disrupted all spheres of health care delivery.1⇓⇓⇓–5 The surge in emergency department visits and hospitalizations has been well reported yet most patients have been treated in primary care facilities and cared for at home.6⇓⇓–9 Surprisingly, there are relatively few reports originating from office-based practice settings. Data from hospital settings have been instrumental in guiding diagnostic and treatment practices, however these data are from severely symptomatic individuals and are not necessarily representative nor entirely relevant to the broad spectrum of symptoms seen in primary care clinics.10 Primary care assumes the role of first contact with the health care system and will be the “first in and last out” of the pandemic including the management of any collateral damage caused by the pandemic.11 Even after surge of the pandemic has waned, and hospitals return to business as usual, primary care physicians remain caring for an extraordinary variety of symptoms and sequels of COVID-19.8,12,13
Hispanic and other minority populations are underrepresented in published literature despite data that show disparate outcomes these groups.11,14 Hispanics represent 18% of the population in the United States yet they make up 34% of new coronavirus cases.15 They are 1.7 times more likely to contract COVID-19 than their non-Hispanic white counterparts, as well as 4.1 times more likely to be hospitalized COVID-19 and 2.8 times more likely to die from COVID-19.16 For many reasons that we still do not fully understand, the Hispanic population has had worse outcomes than any other racial group and extant literature is primarily descriptive and goes no further than begging the question as to why differences in outcomes exist.17 Therefore, studies involving minority persons are not only critical for hypothesis generation and testing to develop health policy and treatment strategies which make outcomes more equitable. The present study, although descriptive, provides further insights into the specific characteristics of COVID-19 infection in the Hispanic patient, and the impact the infection has on their lives.
Alivio Medical Center is a nonaffiliated, free-standing, Point of Care medical center in Indianapolis Indiana serving a low-income Hispanic community. Herein, we describe a Hispanic cohort of patients presenting to our center during the COVID-19 pandemic.
Methods
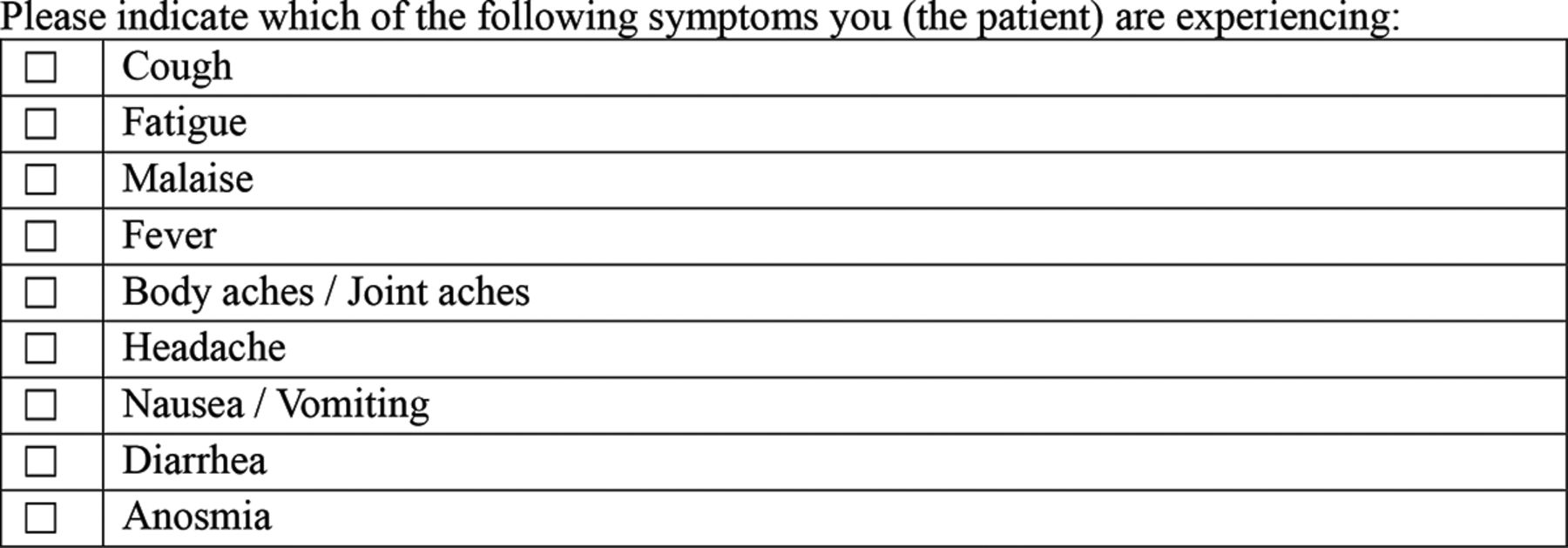
The Western IRB approved this study and granted a waiver of consent (Sponsor: Alivio Medical Center; IRB Pr #: 20210840; Work Order #: 1 to 1404432-1). All study staff in this investigation spoke Spanish fluently and conducted interviews, collected demographic and socioeconomic information and provided treatment in the Spanish language. All patients entering Alivio Medical Center between May 9,2020 and July 31, 2020, were evaluated for SARS-CoV-2 infection using a medical questionnaire for symptoms suspicious for COVID-19 administered by a trained health care professional. Those answering affirmative to 1 or more of the questions were triaged to an isolation and infection containment area (Figure 1). Patients isolated were evaluated by an experienced provider to determine if COVID-19 testing was warranted. Those individuals who underwent SARS-CoV-2 testing were included in this cohort for evaluation. Parameters that guided the decision to do COVID-19 testing were based on expected covid symptoms. However, like any system, at times patients were mis-triaged. For example, a patient with rheumatoid arthritis and is having an arthritis fare was mis-triaged into the COVID clinic because of the source of the joint pain was not clear.
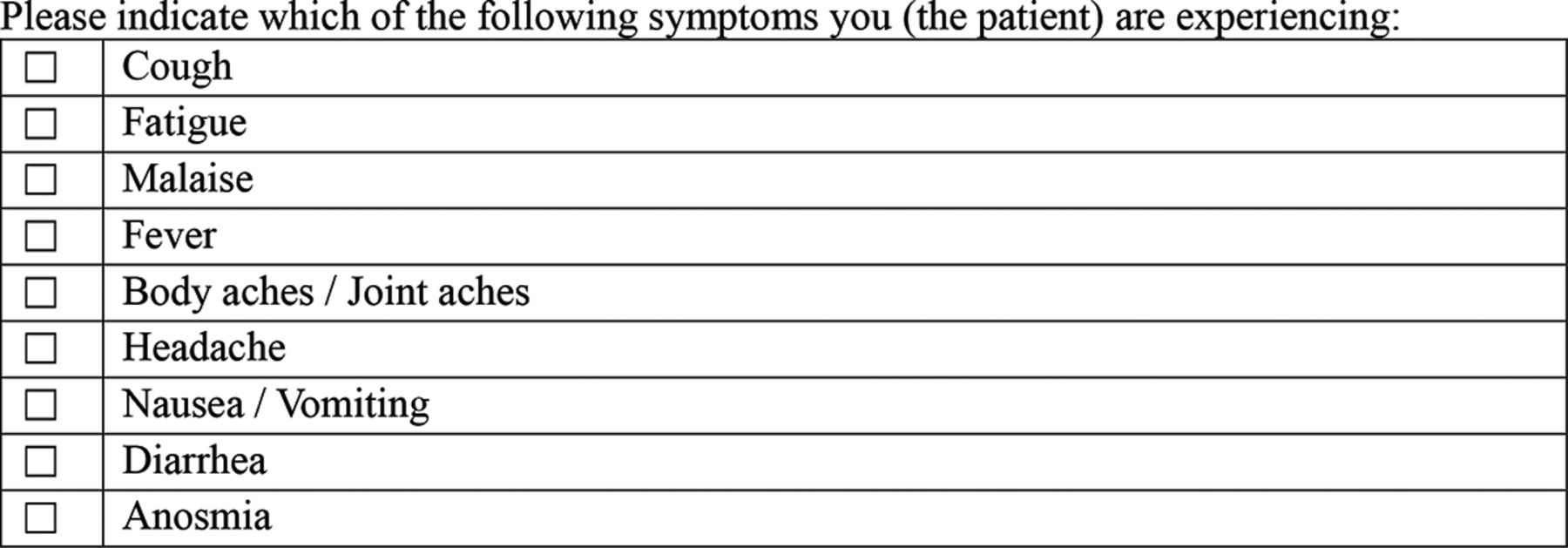
Screening tool for recording patient symptoms.
Electronic medical records in iSalus were used to compile patient's baseline demographics, comorbidities, medications, laboratory, and socioeconomic data. Chest radiographs and clinical course was documented. Socioeconomic data such as employment status, time to recovery, and missed work was collected by self-report in response to an interview by our study staff.
The primary means of testing for COVID-19 infection in this cohort was via polymerase chain reaction (PCR) from anterior nasal swab samples or a rapid antibody test from a finger prick. The PCR test was the Bridge Diagnostics SARS-CoV-2 PCR Method which is performed using an automated version of the ThermoFisher Scientific TaqPath SAR-CoV-2 Combo Kit. The Bridge Diagnostics SARS-CoV-2 PCR Method was tested on both positive and negative samples of varying collection media. This testing method showed 100% concordance of results.
Subjects selected for the detection of SARS-CoV-2 antibodies (IgM and IgG) were tested using the point of care CLUNGENE® SARS-CoV-2 VIRUS IgM/IgG Rapid Test Cassette lateral flow immunoassay (LFA). The CLUNGENE® Test has been commercially available in the US under an FDA approved Emergency Use Authorization (EUA201121) and Europe (CE Mark reference 02PBJ267 dated March 9, 2020) (FDA, 2021). The CLUNGENE® test has been previously studied, including the use of the test in the offices of general practitioners, evaluating the presence of antibodies in convalescent plasma donors, and how the test performs at a point of care facility.18⇓⇓⇓⇓⇓⇓⇓–26 The test employs 1 drop (∼ 10 µL) of whole blood added to a well followed by 2 drops of buffer. Results are available in 15 minutes. The specificity of the assay has been reported as 100%, the sensitivity has been reported at 96.77% with no false-positive results due to infections or vaccinations unrelated to the SARS-CoV-2 virus.27 For the present analysis, a test was considered positive if IgM, IgG, or both antibodies were present.
Baseline characteristics are presented as mean SD or median and interquartile range (IQR) depending on the normality of their distribution. Differences in means were determined by Student's t test and proportions between groups were compared with the χ2 test. Statistical analyses were performed on STATA/S.E. 11.0 (StataCorp, College Station, Tx).
Results
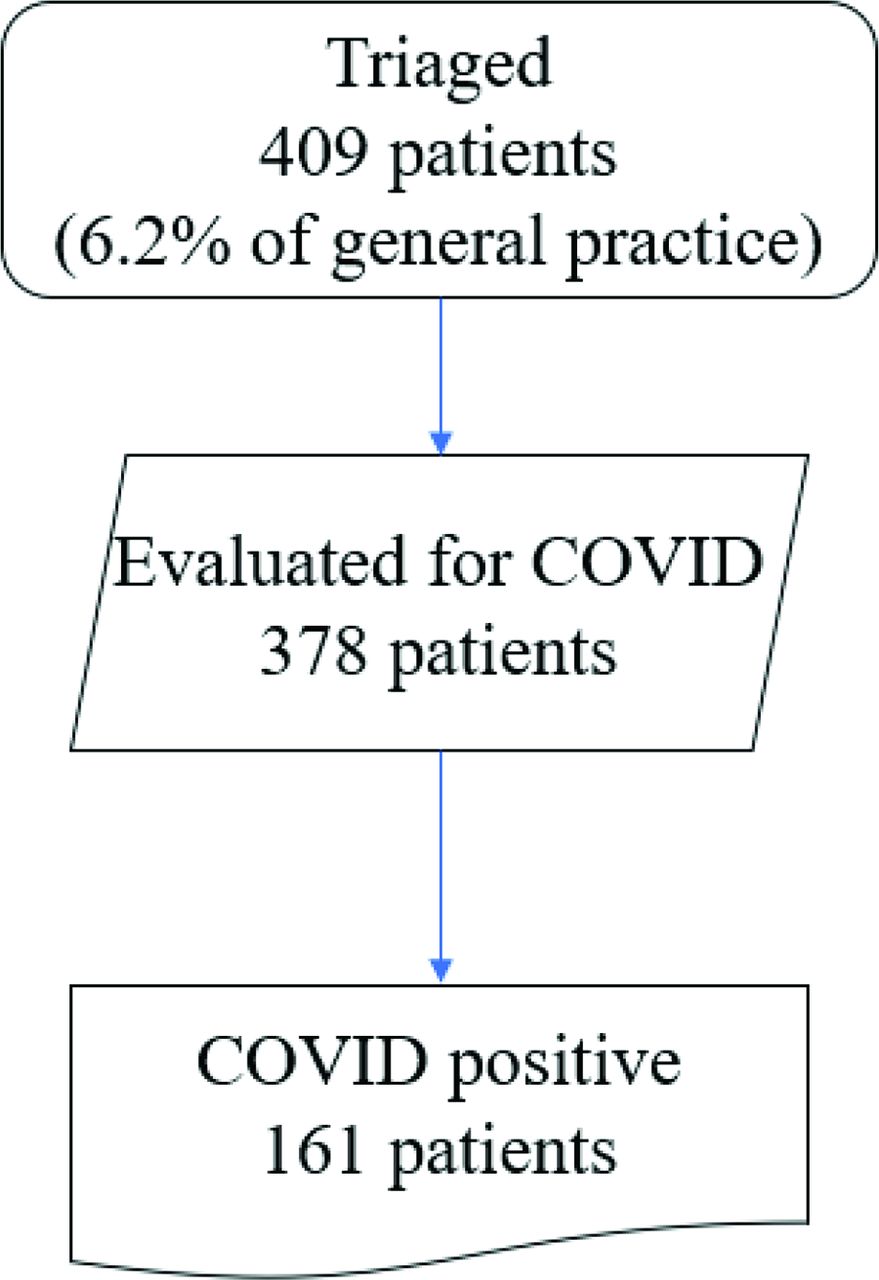
Between May 9, 2020, and July 31, 2020, there were 6616 patient visits to Alivio Medical Center of which 409 were triaged to a patient isolation and containment area if they responded in the affirmative to 1 of the symptoms (Figure 1); triage was determined by an experienced medical assistant who administered a series of questions modeled after those recommended by the CDC. Subjects were triaged to an isolation and containment area if they responded in the affirmative to 1 of the questions. Out of this subset of 409 patients, 378 unique Hispanic individuals were evaluated for COVID-19; all patients included in this analysis were Hispanic. Of these 378 tested patients, 161 (42.6%) tested positive by a PCR test or serologic antibodies (Figure 2); 161 is 2.4% of the general practice. Only those who underwent diagnostic testing, n = 378, are included in the following analysis (Table 1); the remaining 31 were mis triaged and omitted from the study.
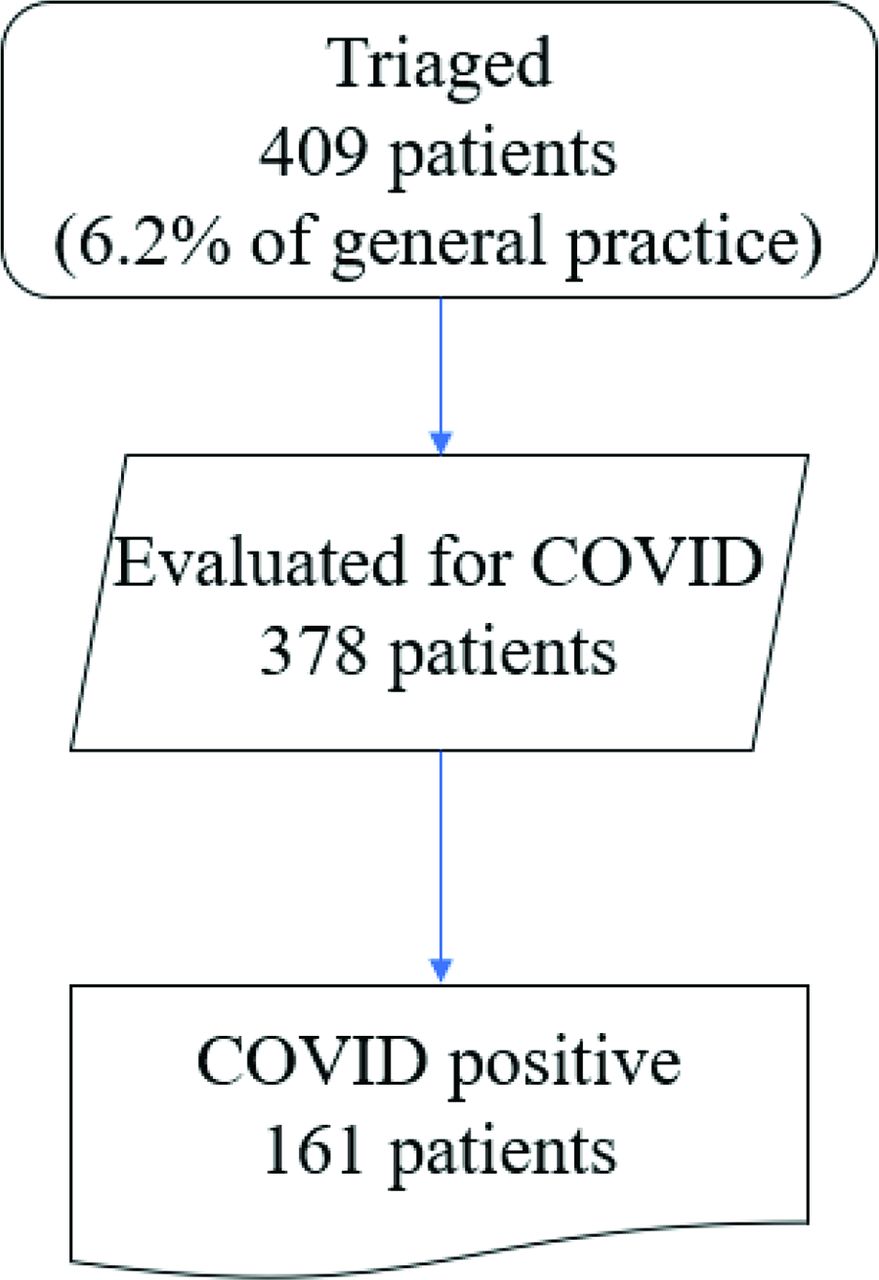
Patient sets. Most patients presenting for medical care in a primary care setting during a pandemic do not have COVID-19. Out of 6616 patient visits, 409 patients were triaged to our isolation and containment area.
Demographics and Vital Signs of Hispanic Patients Tested for COVID-19 at Alivio Medical Center
Of the individuals tested (Table 1), the mean age was 39.4 ± 23.7 years, and the majority were men, 238, (63%). The cohort was predominantly free from chronic disease with relatively few patients endorsing diabetes mellitus, n = 27, 7.3%. Individuals testing positive for COVID tended to be slightly older, 40.9 ± 12.2 versus 38.2 ± 13.0 years, P = .039 and presented later in their disease course 3.1 ± 1.2 versus 5.9 ± 1.2 days, P < .00001 than those with negative tests.
Patients presented to Alivio with a wide range of symptomatology from severely ill to totally asymptomatic. There were 230 patients tested for symptoms and 148 patients tested for other reasons such as contact tracing or to return to work after recovered infection; 1(1) patient was not classified as either symptomatic or nonsymptomatic (Figure 3). The overall positivity rate for patients' symptoms was 37%. For symptomatic patients, their symptoms were clustered into 5 broad groups (Table 2).

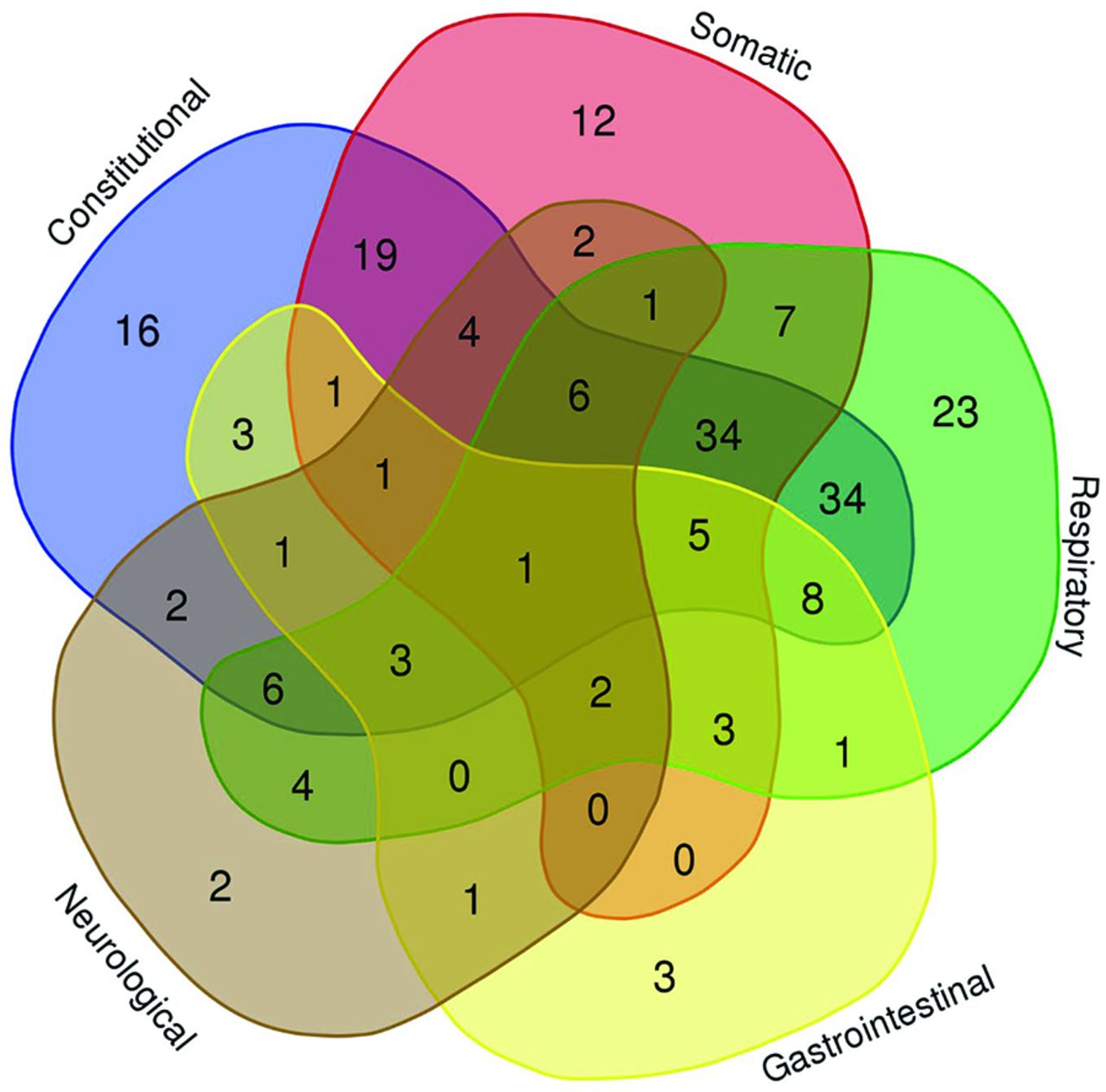
Venn Diagram scatter plot of symptoms clusters. N = 204 patients had 1 or more symptoms in the above categories. Sore throat was not a symptom of the initial variant of COVID-19, thus the omission from this figure. This figure was generated using the Venn diagram webtool from Bioinformatics & Evolutionary Genomics (http://bioinformatics.psb.ugent.be/webtools/Venn/).
Symptom Clusters for COVID-19 Positive Patients
There were 230 patients exhibiting symptoms. The most common groups were constitutional n = 143 (62%) and respiratory n = 136 (59%), followed closely by somatic n = 97 (42%). Neurological n = 34 (15%) and Gastroenterological n = 28 (12%) was least represented (Figure 3). No single group was particularly diagnostic of COVID. However, patients who presented with symptoms distributed across multiple groups were more likely to test positive, P = .0001, χ2 = 20.8. For example, a patient presenting with symptoms distributed across all 5 clusters had an 82.4% chance of testing positive while a patient with only symptoms limited to a single group had only a 27.5% chance of testing positive.
Compared with symptomatic patients, those without symptoms were slightly younger 37.5 ± 1.1 vs 40.6 ± 0.82, P = .02, more likely to have had a close contact with COVID-19 positive person 31.5% vs 9.6%, P < .001 or required a clearance to return to work, 77.3% versus 24.5%, P < .001. Indeed, nearly half, 44.8%, of this Hispanic cohort requested some form of proof disease-free status in order return to employment. Others expressed anxiety about being infected and requested testing for reassurance.
We also sought to investigate some the socioeconomic aspects of the tested patient population; this data were collected as part of the normal patient intake. The majority worked construction, factory, or warehouse (50.7%) jobs with the remainder distributed among food service, housekeeping, landscaping, and delivery jobs. Sixty-one of the 378 (16.2%) had health insurance and only 7 were unemployed. Among employed individuals who had COVID-19 and were symptomatic, 97% reported missing work for a mean of 36 ± 24.8 days, median 30 (IQR 21 to 42) days. Further, more than half of the patients, 57%, had prolonged symptoms, fatigue, sleeplessness, brain fog, and low energy beyond 30 days the most prominent of which was the description of low energy which persisted even after returning to work. Note: the distribution of the sociodemographic characteristics of the study population was the same as the group that was not tested.
Discussion
We studied a cross-section of Hispanic subjects who entered a primary POC setting to examine changes in workflow processes, patient presentation, and the economic and health impacts during a pandemic. There are several novel findings. First, although this patient population had a high prevalence of disease burden, most patients sought care for reasons other than COVID-19; most patients come to our urgent care facility for a variety of adverse health symptoms. Further, triage implementation can effectively screen between infected and noninfected persons and permit care of noninfected persons; the triage process was able to identify 42.5% of suspected cases (161 of 378), showing the efficacy of this protocol (See Figure 1). Second, although individual symptoms (eg, fever) have a relatively poor predictive value for the diagnosis of COVID, symptoms spread across multiple system clusters were better predictors of positivity in Hispanic patients. However, clusters of symptoms may provide better predictors for positivity; in multivariable modeling the only significant (P < .05) is the clusters of symptoms. Third, infected individuals are likely to experience substantial job and wage loss, and fourth, even after returning to work, more than half of our Hispanic patients are experiencing prolonged symptoms.
Workflow Dynamics
One of the first observations we found was that even in the middle of the pandemic, the majority of our patient visits were from noninfected persons presenting for routine care. Although it is beyond the scope of the present manuscript to compare those presenting for routine care with those presenting for COVID-related reasons, we realize that in our community we are the first point of contact for a broad spectrum of patients: those with suspected COVID-19, patients with test confirmed COVID-19 (with or without symptoms), patients in contact with suspected or confirmed cases, patients anxious about COVID, and patients with non-COVID-19 health care needs. By creating a point-of-entry triage system, early isolation, and containment of potentially infected persons, safe in-person delivery of health care to all persons through the pandemic was able to be maintained. This assuages the concern for collateral damage to the health of a population due to abandoned or postponed routine care.
Symptom Clustering
We use a standardized treatment approach based on symptom clustering by dedicated frontline personnel that have developed subject matter expertise.28 Hence the variability in patient management is limited thus improving the efficiency of patient flow and outcomes. Clustering of symptoms demonstrates the truly syndromic nature of this disease with its myriad faces. Individual symptoms seem to have relatively poor diagnostic ability. Our findings are consistent with Dixon et al, who found that most individual symptoms had a positive predictive ability of less than 50%.28 However, grouping symptom combinations into 5 general systems has better diagnostic and prognostication properties. Hence, in our population the cumulative burden of symptoms is a more reliable predictor of COVID-19 than any individual symptom.29 For example, a patient with diarrhea, body aches, fever, and anosmia are much more likely to be infected than 1 with cough alone. After an extensive literature review, we have not been able to identify differences of symptoms clusters between race groups.
Beyond diagnostic uses, we found symptom clustering to be important in treatment algorithms. Treatment protocols for most patients with mild to moderate COVID are supportive and tailored to alleviate system-specific symptoms. For example, a person presenting with fever and somatic complaints can be treated with Tylenol and or nonsteroidal whereas 1 presenting with gastroenterology symptoms would have their liver enzymes evaluated and treated with intravenous fluids and an antiemetic.30 Most importantly, patients with symptoms clustering into the respiratory system deserve special attention and the most intensive management. We aggressively use early use of oxygen at home for silent hypoxemia, aggressive management pneumonia, dexamethasone31 and inhaled steroids, bronchodilators and pulmonary physiotherapy to reduce V/Q mismatch.32 Thus, clustering also can guide resource allocation.
COVID-19 in a Hispanic Population
The present cohort was made up of a primarily Spanish-only speaking, young, working Hispanic population. They were mostly uninsured (87%) and were employed in factories or other service-based industries deemed “essential.” Our sick patients missed more than a month of work and more than 1-half of this population had mild to moderate ongoing symptoms even after returning to work. Thus, the so-called “long haulers” may be more prevalent in the Hispanic population than that reported in other groups. The prevalence of prolonged symptoms is reported at 10%, whereas our data reports up to 57%.7,33 For example, other minority groups have been found to be more likely to experience post-COVID-19 symptoms such as breathlessness.34,35 Our data deem to indicate that prolonged COVID-19 symptoms are prolonged in the Hispanic patient population and it deserves to be investigated further. More work is needed to truly estimate the economic impact of the pandemic on urban Hispanics.
Our nonsick patients often required testing before being able to return to work. The finding that most of our patients were deemed essential workers, and therefore exempt from the state public health directives to stay home, is not surprising but may, in part, explain why this population had higher infection rates than other groups. Multigenerational housing, close working conditions, and poor ventilation in the factories and warehouses are well known and contributory.
In the Midwest, COVID-19 deaths increase with the proportion of Hispanic residents per county. Other reports have found that monolingual Spanish speakers were more likely to have higher rates of COVID-19. Indeed, limited English proficiency is associated with lower health literacy and increased susceptibility to misinformation. Pragmatically speaking, we devoted a lot of resources into presenting a linguistically appropriate, culturally relevant, nonpoliticized, and demythologized message to our patient population. We feel that organizations such as ours with bilingual providers will be essential to future outbreaks. We believe further studies – such as this 1 – are needed to better understand the true economic impact of the pandemic in the Hispanic communities across the United States.
Testing Strategies in Primary Care
Another challenge that primary care faces in a pandemic is offering the most appropriate diagnostic test to patients along a severity spectrum from totally asymptomatic to acutely ill. Understanding the strengths and weaknesses, that is, the time dependent sensitivities and specificities, of each test and tailoring the approach to each patient is important not only for making the diagnosis but also for managing expectations of the patient.36,37 Nucleic acid-based tests are obviously the gold standard in the acutely ill person but even these have important limitations. For example, there is a decay in the sensitivity of reverse transcriptase polymerase chain reaction to detect virus particles after approximately a week after exposure and the false negative rate at 3 weeks is 50 to 60%.38
We have found that the presence of antibodies is often comforting to the patients as there is a great deal of anxiety surrounding both the facts and the myths of the virus. The consolation of seropositivity, even after vaccination, helps to assuage the fears of reinfection. However, the presence of antibody cannot yet prognosticate risk of recurrent infection.39,40 In our own practice, we have seen seropositive individuals revert back to seronegative. The significance of this is unknown. Ongoing investigations are underway to understand the duration and the neutralizing ability of antibodies as well T-cell-mediated responses generated from natural or vaccine-derived immunity, especially as new coronavirus strains emerge. Clearly, a 1 test-fits-all strategy is doomed in a primary care facility. Careful attention to emerging strains as well as emerging technology will be critical to best serve the many needs of our patients.
Limitations
There are several limitations that merit mentioning. The first is that we did not use a universal testing strategy and therefore asymptomatic patients may have been admitted to areas outside our infectious containment area. This choice was made because of the notoriously high false negative rates in both PCR and serologic tests in the recently infected but not yet symptomatic individuals. During the 3-month study period, only 1 staff member became infected. The staff members had their temperature taken daily on entry into the clinic. The questionnaire was posted in the clinic where it was easily seen. All members of the staff were tested if they exhibited 1 or more of the symptoms or if they exhibited a fever. Hence, we maintain that this was an effective containment strategy.
Another limitation was that PCR and antibody tests were not available throughout the entire study period. Although PCR and antibody tests were available from 5/9/2020, they were used very selectively because the turnaround time was up to 4 to 5 days and were not very helpful in making decisions at the point of care. Our strategy evolved and we assimilated new testing processes as new technology became available during the pandemic. Finally, this is a small study, but it represents granular data from urban-based point of care practice serving a minority community.
Conclusions
This report represents a real-world experience managing Hispanic patients in a primary care practice in Indiana, United States, during a global pandemic. The present study provides insights into the specific characteristics of COVID-19 infection in the Hispanic patient and the impact the infection has on their lives. Early and rapid diagnoses are critical to mitigate the health and socioeconomic impact of COVID-19 on patients. Offering a variety of test options to meet the severity of symptoms along with information that bypasses language barriers are effective first steps to improving care in these communities. Our Hispanic population is even more susceptible to the impact of COVID-19 as they often lack insurance encouraging professional health care services, have greater chances of extended sickness durations and long-COVID symptoms, and cohabitate in multi-generational housing leading to further spread of the disease.
We feel that the dissemination of information from primary care organizations such as ours will be critical for preparing for the future pandemics. Patient flow strategies were adapted to ensure care of infected and noninfected individuals. A comprehensive testing strategy was used to best accommodate symptomatic and asymptomatic individuals. And treatment strategies were determined based on a symptom clustering approach. Whether our management strategies resulted in fewer hospitalizations is not yet known but is currently under active investigation. The hard-won lessons should be retained for better preparedness for all invested parties; public, patients, providers, and policy makers.
Notes
This article was externally peer reviewed.
Funding: This is an investigator sponsored manuscript and funded entirely internally from Alivio Medical Center.
Conflicts of interest: There are no conflicts or competing interests to declare. Christopher Lamb, PhD, has worked with the manufacturers of SARS-CoV-2 tests for Emergency Use Authorization submissions to the US FDA.
To see this article online, please go to: http://jabfm.org/content/35/4/686.full.
- Received for publication April 15, 2021.
- Revision received July 23, 2021.
- Revision received August 1, 2021.
- Revision received January 22, 2022.
- Accepted for publication February 24, 2022.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Use of a rapid triage assessment tool to discriminate the need for hospitalisation in patients with severe COVID-19 infection presenting to an outpatient clinic: a single-centre, prospective cohort study
- Family Medicine Researchers Explore the Social Determinants of Health, COVID-19 Issues, and Cancer Survivor Care