
Abstract
Introduction: The ongoing COVID-19 pandemic initiated the implementation of numerous disease mitigation strategies aimed to prevent transmission of the SARS-CoV-2. Given the similarity in mode of transmission, we posit that these strategies have also had a collateral benefit in minimizing the transmission of influenza during the 2020 to 2021 season in California.
Methods: Five years of data including incidence of influenza-like illness (ILI), influenza hospitalization, and mortality related to influenza in California were analyzed.
Results: In each of these parameters, there was a marked decrease in influenza activity, suggesting the additional benefit of COVID-19 mitigation strategies on influenza prevention.
Discussion: Further study is recommended to determine which specific variables had greater impact on transmission of respiratory viruses, and therefore can be utilized to prevent future outbreaks of respiratory illness.
Introduction
A state of emergency was declared in California on March 4, 2020, after the first reported death of a California resident due to COVID-19. This began the implementation of several COVID-19 mitigation strategies to prevent transmission of the disease. This included the cancellation of large events, restaurant closures, mask wearing mandates, and travel bans, among others. These measures have had a profound effect on the course of pandemic, which has led many to infer the impact of these mitigation strategies on the transmission of other respiratory illnesses, such as influenza.1
Both influenza and SARS-CoV-2 are transmitted through respiratory droplets, most often through coughing or sneezing. For this reason, masks are an effective tool to mitigate respiratory virus transmission. Although there is controversy about the effectiveness of masks, numerous studies have shown that in general, mask-wearing has a protective effect against the transmission of respiratory viruses.2 Moreover, other social distancing strategies, such as school closures and travel bans, have obvious benefit in the reduction of both SARS-CoV-2 and influenza transmission.
Influenza makes a good candidate for study because of its year-to-year variability and distinct seasonality, which is driven mainly by climate. A complex interaction between alternating subtypes and antigenic drift determines yearly variation in subtypes and corresponding disease severity.3 Flu seasonality is typically defined by a significant increase in activity during the winter months. Despite its consistency, the dynamic seasonality of influenza is poorly understood. Emerging research suggests that the underlying factors contributing to influenza's cyclic epidemic cycle relates to seasonal variations in host health, temperature, and air travel which has a large spike during the winter months.3
Despite the widespread availability of a vaccine in the country, the disease burden of influenza continues to weigh heavily on the US. The CDC estimates that in the 2019 to 2020 season, influenza infected 35,000,000 Americans, caused 380,000 hospitalizations, and 20,000 deaths.4 Furthermore, the estimated average total economic burden on the US was $11.2 billion as of 2018.5 As the winter months of 2020 approached, both citizens and health care providers braced for the combined burden of both the new coronavirus and the seasonal flu. However, the anticipated peak of the flu season never came, perhaps preventing a catastrophic inundation of the US health care system.
In this study, we propose that the COVID-19 mitigation strategies employed in the state of California had a collateral benefit on preventing influenza infection and disease.
Methods
Data and figures were taken from the California Influenza Surveillance Program of the California Department of Public Health (CDPH), which publishes a weekly influenza surveillance report. The report from week 20 (May 16-May 22) of 2021 was used for this study. We analyzed values for influenza-like illness visits among patients seen by California sentinel providers, influenza-related hospital admissions, and deaths coded as influenza over the last 5 years (2016 to 2021). The start and end points coincide with the typical beginning and end of the flu season in California (Fall-Summer). These data were then analyzed for trends coinciding with each year's flu season. These 3 parameters serve as an appropriate proxy for influenza activity, as they cover a wide range of disease severity (ie, outpatient, inpatient, death).
Eighty-five sentinel providers participated in the influenza surveillance report, as of week 20 (May 16 – May 22) of 2021. Influenza-like illness (ILI) was defined as any illness presenting with fever (≥100 or 37.8), cough and/or sore throat, and the absence of a known cause other than influenza.
Data from Kaiser Permanente facilities in Northern California were also used to track rates of influenza hospital admission over the last 5 years. Admission diagnosis including keywords: “flu,” “influenza,” “pneumonia,” and other similar words were used to identify pneumonia and influenza related admissions (P&I admissions). The total number of P&I admissions was divided by the total number of hospital admissions occurring in the same period (2016 to 2021) to estimate the percentage of P&I admissions. In addition, the CDPH notes that admissions due to pregnancy, labor and delivery, birth, and outpatient procedures were excluded from the denominator.
Influenza mortality data were obtained from death certificates. The CDPH defined influenza-related death as any death field on a death certificate that included influenza. The total number of death certificates mentioning influenza was then divided by the total number of all cause deaths during the same time period (2016 to 2021). The CDPH notes that influenza-coded deaths are not necessarily laboratory-confirmed and thus are an underestimate of all influenza-associated deaths.6
Vaccination data over the last 5 years were also analyzed to determine how changes in vaccination coverage may have affected trends in the incidence of influenza. Data were collected from the CDC National Center for Immunization and Respiratory Diseases (NCIRD) FluVaxView, which is publicly available at no cost on the agency website. We acknowledge that our interpretations do not reflect the views of the US Government, Department of Health and Human Services, or Centers for Disease Control and Prevention. Data for patients age 6 years and older were included, as this is the recommended age for flu vaccination. End-of-season rates of vaccination coverage was estimated using May as an end point, when the flu season typically ends in America. Percent coverage was determined by dividing the number of documented seasonal influenza vaccinations over the total number of respondents.7 Only vaccination data for seasonal influenza were used. H1N1 vaccination data were omitted as it does not follow the same seasonality as influenza A and is therefore not relevant to this study.
Results
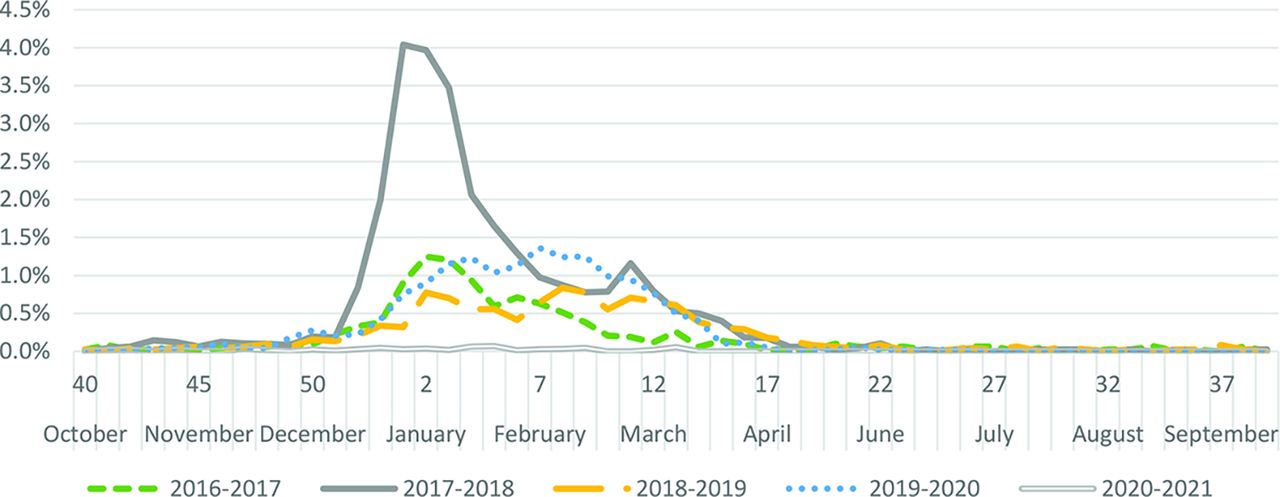
Figure 1 illustrates a dramatic decline in percentage of influenza-like illness (ILI) visits among patients seen by California sentinel providers between 2016 and 2021. Influenza season occurs in the fall and winter months, peaking typically in February, as is shown in the figure. In the 2020 flu season, however, the rise of ILI ends at a comparatively low peak in February 2021 and subsequent decline in following months. A similar trend is observed in hospitalization due to influenza. In comparison to previous flu seasons, 2020/2021 saw only twenty-eight ICU hospitalizations, 6 ICU admissions, and 2 deaths among persons diagnosed with influenza on admission. 6

Percentage of influenza-like illness visits among patients seen by California sentinel providers, 2016 to 2021. Source: California Influenza Surveillance Program's weekly report (week 20: May 16, 2021 – May 22, 2021). Eight-five sentinel providers provided data to the study. Numerators and denominators were not publicly available. Seasonal baseline was calculated using a regression model applied to 5 years of data before the COVID-19 pandemic.
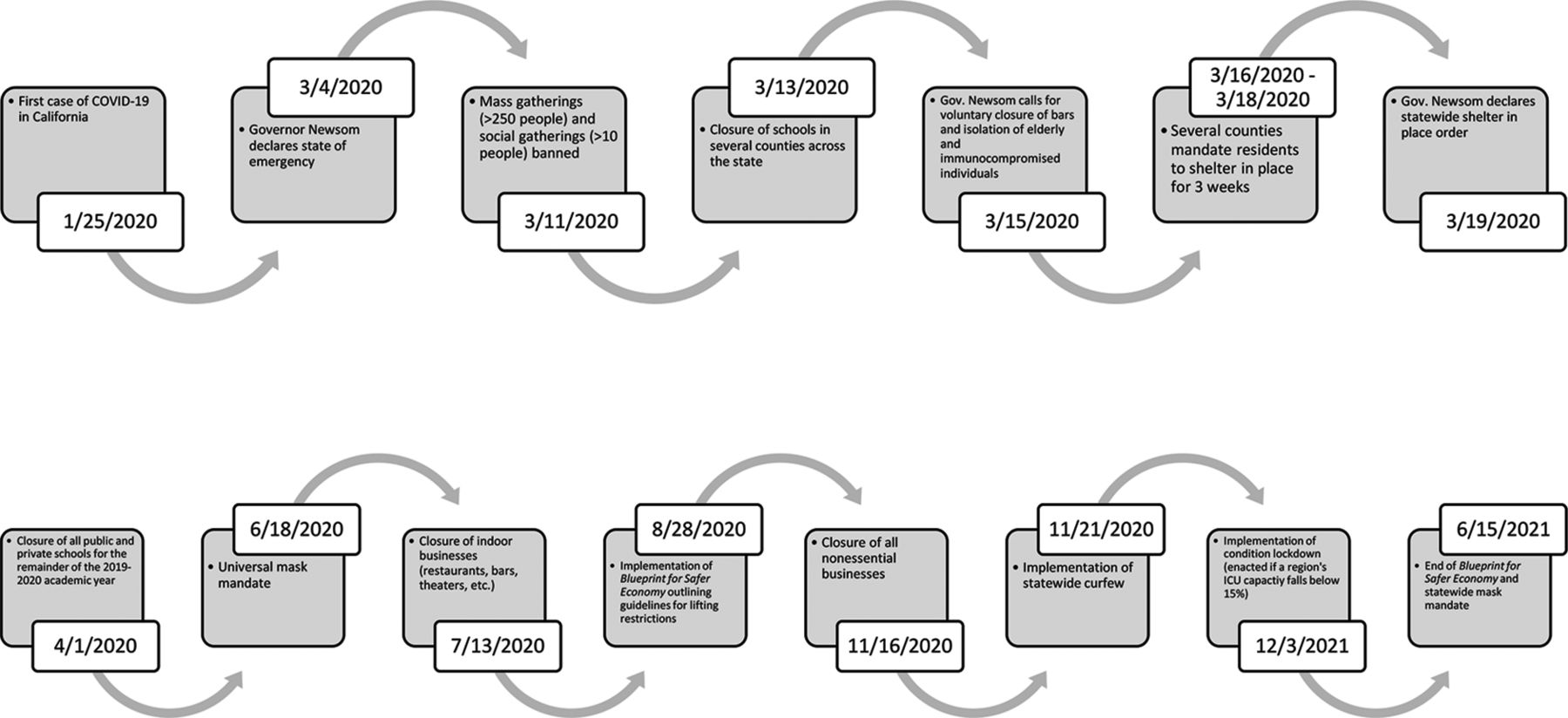
Figure 2 illustrates the timeline of the implementation of COVID-19 mitigation strategies in California. Spanning from early March 2020 to June 2021, both state and local governments gradually implemented various mitigation measures.8 In comparing Figures 1 and 2, it is evident that these implemented measures correlate with the relatively low incidence of influenza at each time point.

Timeline of California COVID-19 mitigation policies. Source: CalMatters. Major events in the implementation of COVID-19 mitigation strategies are mapped onto a timeline overlapping with the 2020/2021 flu season. Although policies continued to change afterward, the end of California's Blueprint for Safer Economy Program was used as an endpoint since it coincides with the end of a typical flu season.
Figure 3 shows the percentage of influenza-coded deaths occurring in California from 2016 to 2021. The 2020/2021 flu season also shows a dramatic decrease in influenza-associated mortality. During week 20, no influenza-coded deaths were reported. The 2020/2021 season in total included only fifty influenza-coded deaths. Thirty-three (66%) of influenza-coded deaths occurring in the 2020/2021 season were persons aged 65 or older.9

Percentage of influenza-coded deaths occurring in California among California residents, 2016 to 2021. Source: California Influenza Surveillance Program's weekly report (week 20: May 16, 2021 – May 22, 2021). Numerators and denominators were not available. Influenza-coded deaths were coded as deaths in California which included influenza in the cause of death field on the death certificate. This sum was then divided by the total number of deaths in California in the same time period to achieve the values shown in the figure. California Department of Public Health (CDPH) notes that influenza-coded deaths are not necessarily laboratory-confirmed cases of influenza, and therefore these values underestimate the true number of influenza-associated deaths.

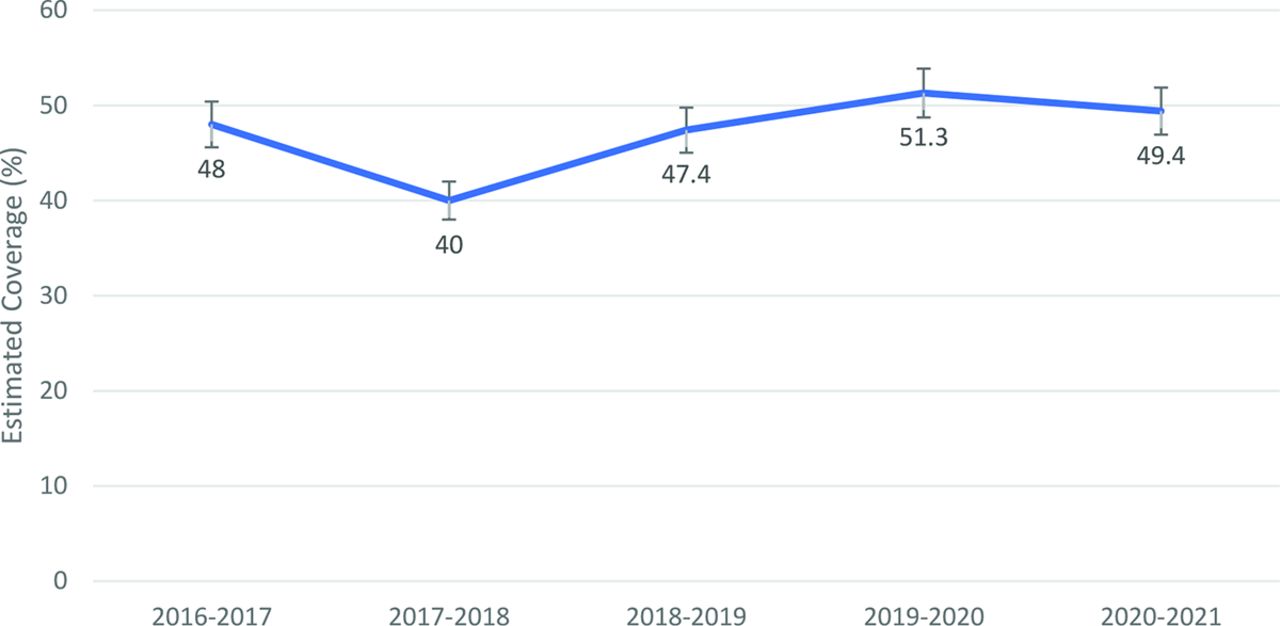
End-of-season influenza vaccination coverage in persons ≥ 6 months, California. Source: CDC National Center for Immunization and Respiratory Diseases (NCIRD) FluVaxView. Sample size in each year was as follows: 2016 to 2017: 8010, 2017 to 2018: 10,838, 2018 to 2019: 9857, 2019 to 2020: 7935, 2020 to 2021: 9129).
We also analyzed California influenza vaccination coverage in persons aged 6 months and older over the last 5 years. These data shown in Figure 4 were collected from the CDC National Center for Immunization and Respiratory Diseases (NCIRD) FluVaxView. These values represent estimated end-of-season rates of vaccination using May as an endpoint, when the flu season typically ends in America.7
Discussion
A significant downward trend was observed in the number of influenza cases, number of hospitalizations due to influenza, and mortality due to influenza in 2020-21. We think that COVID mitigation strategies could have contributed to the decrease in incidence of influenza in California. The decline in influenza cases during the pandemic is not limited to California. In Taiwan, a similar study concluded that disease prevention measures, hospital preparedness and response, and public awareness and compliance in response to COVID-19 provided collateral benefits of significant reduction of severe influenza, S. Pneumoniae, and deaths due to pneumonia.10 Studies show a disruption in many respiratory viruses, including influenza, during the COVID-19 pandemic in the United States as a whole. Similar trends are seen in decline of laboratory-confirmed influenza hospitalization, as well as reduced diversity of subclades relative to previous years.11
There is evidence to suggest that relaxation of COVID-19 mitigation strategies led to late outbreaks of influenza, which had been previously controlled. In Cambodia, influenza season typically occurs from May to July, however much like California, influenza circulation was much lower than previous years. Sovann et al. found that in Cambodia, where COVID-19 restrictions had been eased in June and July 2020, an outbreak of influenza occurred in August 2020, which is atypically late in the season.12 This further supports the link between influenza and COVID-19 mitigation strategies.
1 limitation of this study is that in the calculation of percentage of ILI, hospitalization, and mortality due to influenza, the denominator (total number of patients) was likely affected by the pandemic. Although the CDC report did not include these numbers, it is possible that both office visits and hospital utilization may have decreased in response to limited health care access and hospital capacity during this time. This may account for part of the decrease in ILI and influenza hospitalization. Similarly, all-cause mortality increased in 2020 due to COVID-19, which may have skewed the percent mortality due to influenza in that year. It is unclear, however, whether these limitations wholly account for the dramatic decline in influenza that occurred in 2020. In addition, the hospitalizations due to influenza in Kaiser Northern California hospitals included “pneumonia” admissions. This skews the data because pneumonia has multiple etiologies that do not relate to influenza.
We also explored the possibility that the COVID-19 pandemic changed vaccination behavior. The CDC's report on the subject concluded that 35% of respondents reported that they were more likely to receive the influenza vaccine because of the COVID-19 pandemic. By contrast, 11% of respondents reported being less likely to receive the influenza vaccine because of the pandemic.13 As shown by the end of the flu season in May 2021 there appeared to be no significant change in vaccination status from the previous year.7 Therefore, these differences are unlikely to account for the decline in influenza in 2020/2021.
Acknowledgments
We thank the California Department of Public Health and California Influenza Surveillance Program for their data and figures. We would also like to thank the physicians who participated in their surveys, which allowed us to conduct this study.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/4/680.full.
- Received for publication November 1, 2021.
- Revision received January 25, 2022.
- Accepted for publication January 27, 2022.




{kind=link}
{kind=link}
{kind=link}
{kind=link}