
Abstract
Purpose: To review the literature on medication safety in primary care in the electronic health record era.
Methods: Included studies measured rates and outcomes of medication safety in patients whose prescriptions were written in primary care clinics with electronic prescribing. Four investigators independently reviewed titles and analyzed abstracts with dual-reviewer review for eligibility, characteristics, and risk of bias.
Results: Of 1464 articles identified, 56 met the inclusion criteria. Forty-three studies were noninterventional and 13 included an intervention. The majority of the studies (30) used their own definition of error. The most common outcomes were potentially inappropriate prescribing/medications (PIPs), adverse drug events (ADEs), and potential prescribing omissions (PPOs). Most of the studies only included high-risk subpopulations (39), usually older adults taking > 4 medications. The rate of PIPs varied widely (0.19% to 98.2%). The rate of ADEs was lower (0.47% to 14.7%). There was poor correlation of PIP and PPO with documented ADEs leading to physical harm.
Conclusions: This literature is limited by its inconsistent and highly variable outcomes. The majority of medication safety studies in primary care were in high-risk populations and measured potential harms rather than actual harms. Applying algorithms to primary care medication lists significantly overestimates rate of actual harms.
- Adverse Drug Events
- Electronic Prescribing
- Family Medicine
- Medication Safety
- Primary Health Care
- Systematic Review
Introduction
Medication-related errors in primary care have been estimated to cause many potentially unnecessary emergency department (ED) visits and hospitalizations.1 A commonly quoted estimate that appeared shortly after the Crossing the Quality Chasm report was that 27% of all ambulatory patients experienced an adverse medication event.2 There has always been controversy over how to define medication safety in primary care.3
It has been recognized that primary care is a well-connected agent in a complex adaptive system, and therefore it is inappropriate to apply simplistic linear quality measures to this care.4 High-value primary care could include other goals such as deprescribing in the elderly; patient-centered shared decision-making, where patients accept increased risks in one domain of their life to achieve an important outcome in another domain; and the influence of social determinants and comorbidities in patients with multiple chronic diseases.5⇓–7
Many of the early studies of medication safety in primary care were published before the electronic health record (EHR) era.8 One systematic review recognized the limits of EHRs as a source of actionable data to improve quality and safety.9 Other systematic reviews of safety in primary care list medication outcomes as “incidents” that included studies before the EHR era10 or developed problem-mapping approaches.11 No reviews were identified that explored more deeply the varied ways medication safety in primary care may be defined and measured, the relationship between perceived errors and patient harm, and more recently discussed concepts such as deprescribing and patient shared decision-making that may influence perceptions of medication safety events.
The aim of our study was to systematically review the literature on the definitions of and methodologies for measuring medication safety in primary care and to update estimates of the expected rates of adverse drug events (ADEs) in the EHR era. We were also interested in how considerations of deprescribing and patient shared decision-making impacted definitions and measurements of medication safety. For studies with interventions to improve medication safety, we evaluated ambulatory patients cared for by primary care physicians (PCPs) who prescribed medications from their clinics. Interventions could include any aimed to affect PCP prescribing. Outcomes could include any measure of medication safety or patient harm.
Method
Eligibility Criteria
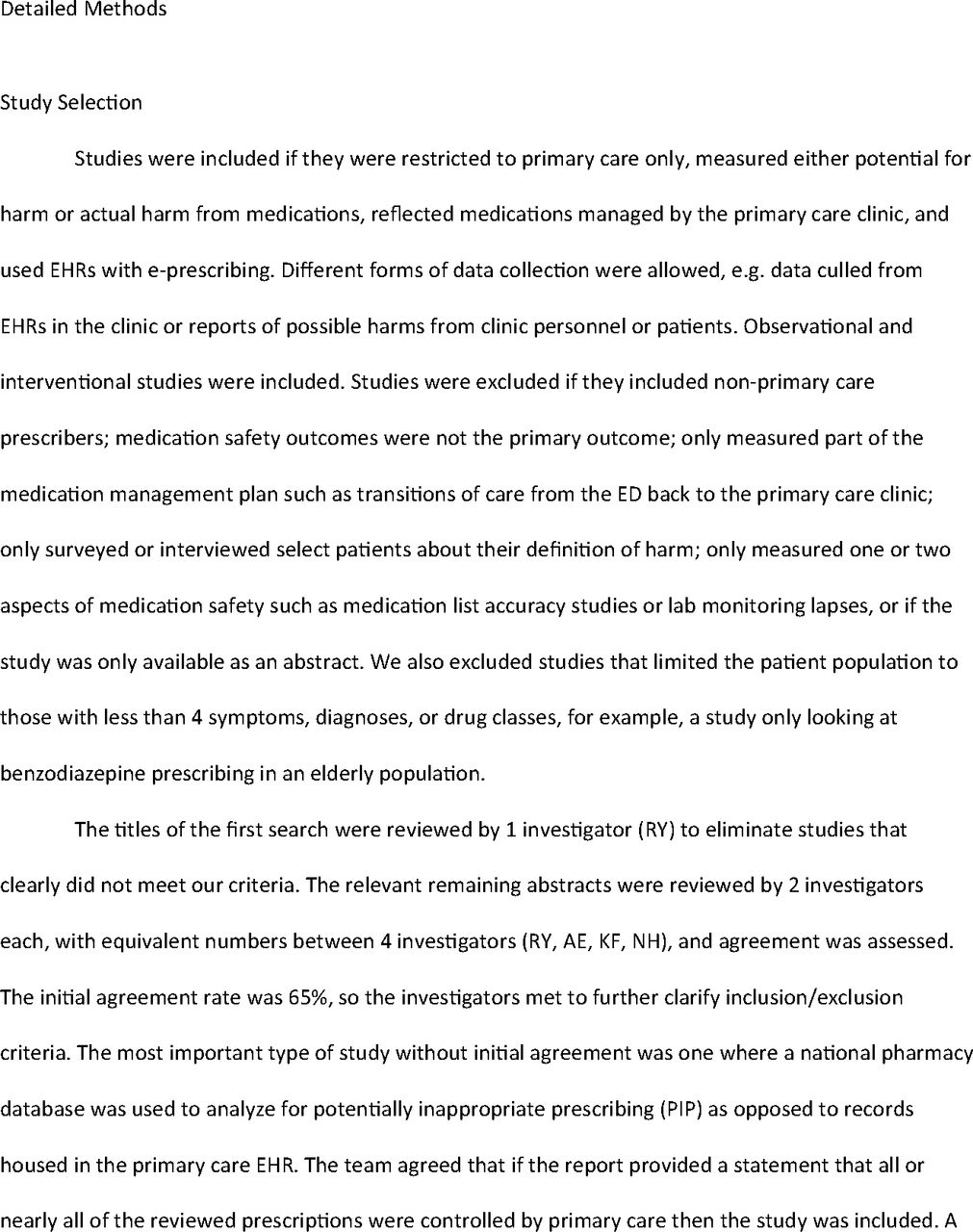
Studies were included if they were restricted to primary care populations only, measured either potential for harm or actual harm from medications, reflected medications managed by the primary care clinic PCPs, and used EHRs with e-prescribing. Noninterventional and interventional studies were included. Studies were excluded if they included nonprimary care prescribers, medication safety outcomes were not the primary outcome, they only measured part of the medication management plan such as transitions of care from the ED back to the primary care clinic, they only surveyed or interviewed select patients about their definition of harm, they only measured 1 or 2 aspects of medication safety such as medication list accuracy studies or lab monitoring lapses, or if the study was only available as an abstract.
Search Strategy and Study Selection
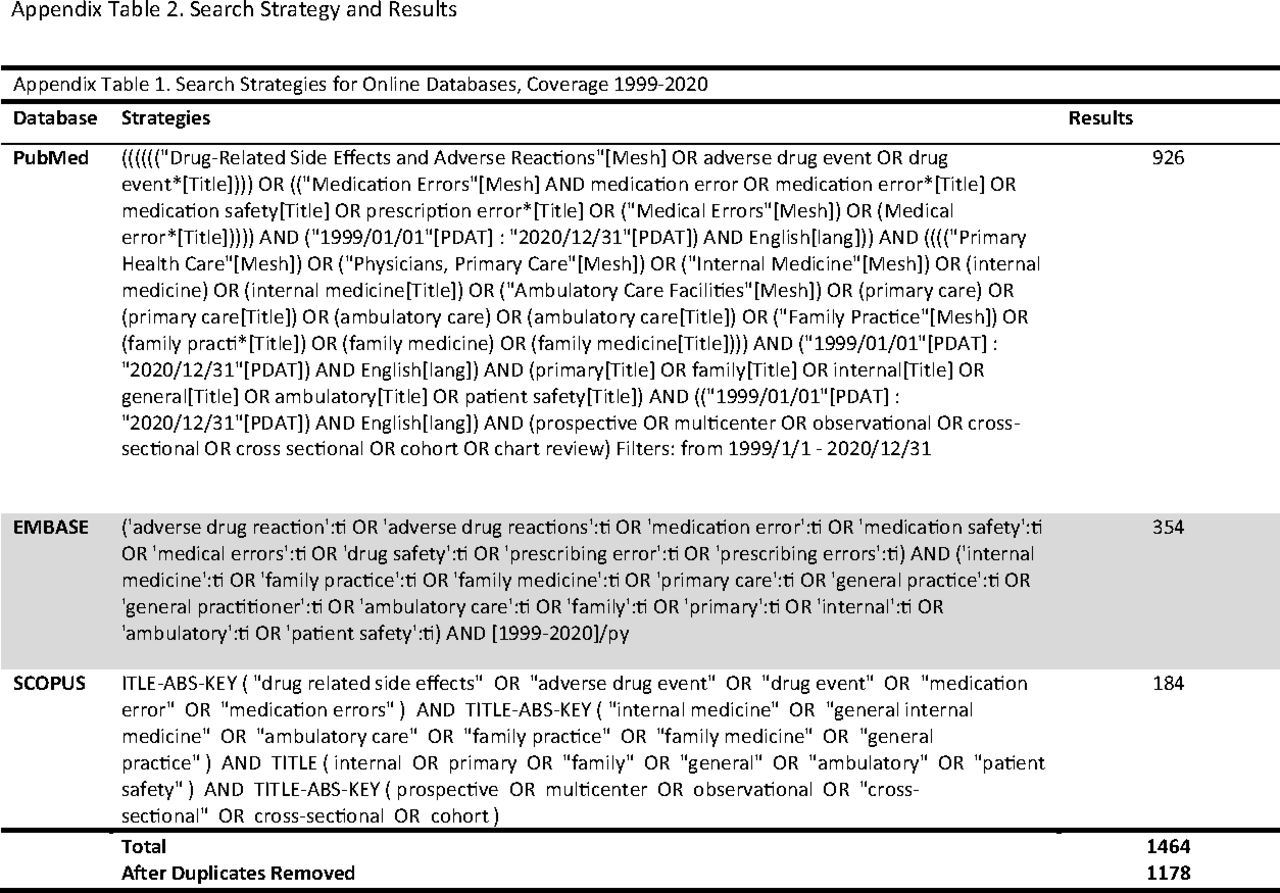
We searched the published literature from January 1999 to December 2020 using Medline, EMBASE, and SCOPUS for relevant English-language articles examining the rates and outcomes of medication errors in prescriptions written by PCPs for their clinic patients. The complete search strategy with keywords and other detailed methods is available in the supplementary online material.
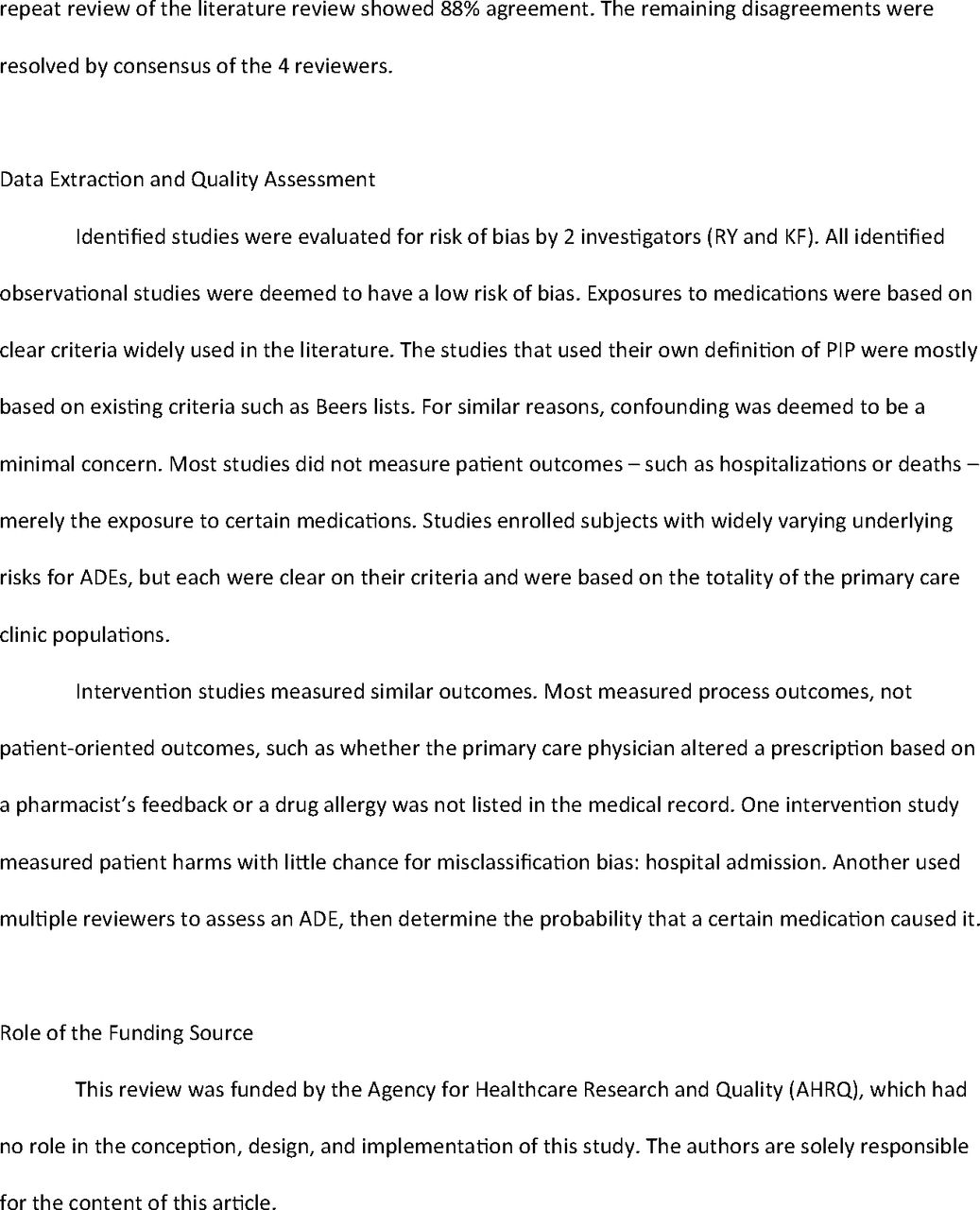
The titles of the first search were reviewed by 1 investigator (RY) to eliminate studies that clearly did not meet our criteria. The relevant remaining abstracts were reviewed by 2 investigators each, with equivalent numbers between 4 investigators (RY, AE, KF, NH), and agreement was assessed. The remaining disagreements were resolved by consensus of the 4 reviewers.
Data Extraction and Risk of Bias Assessment
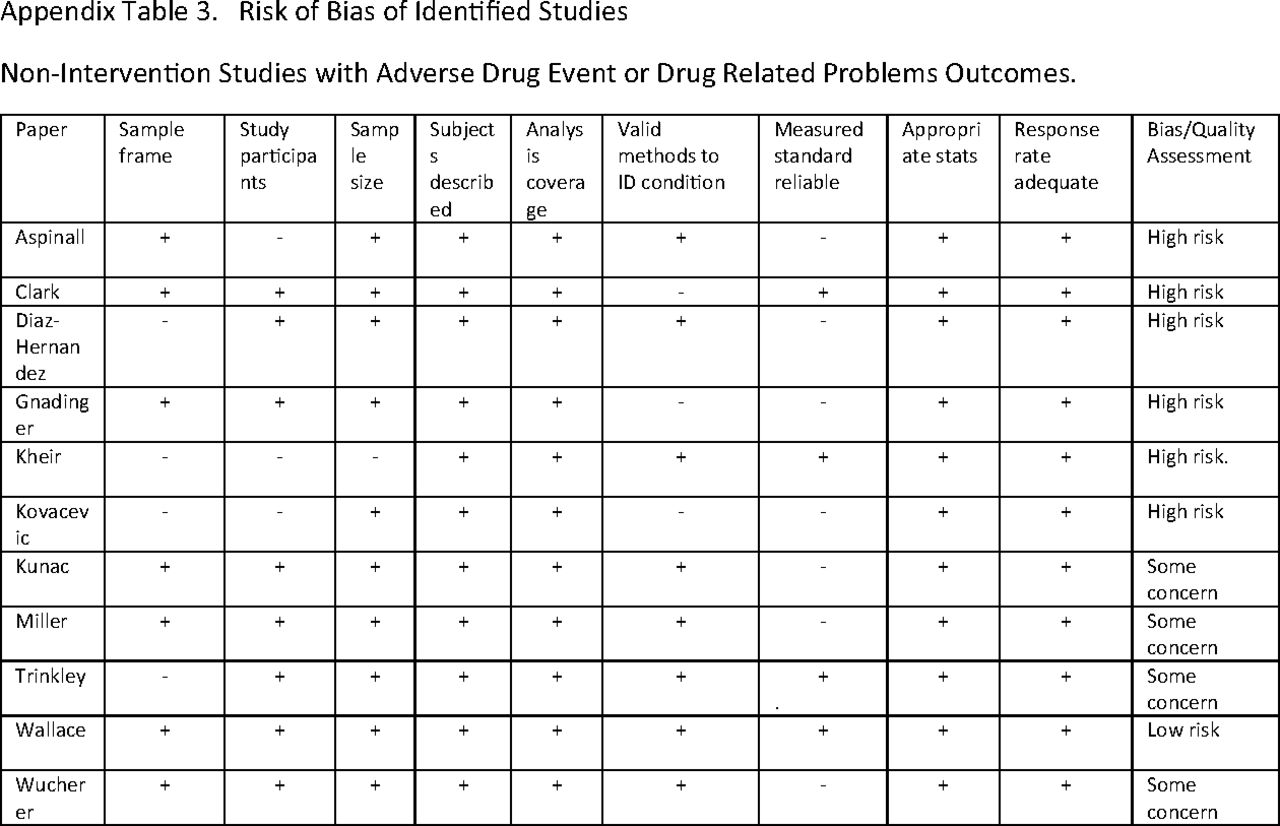
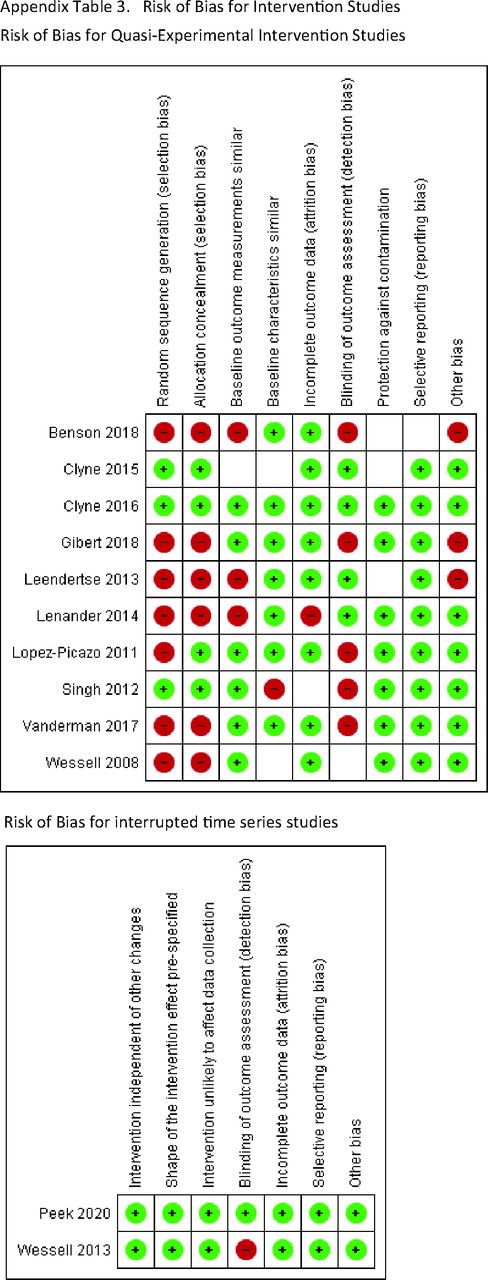
Identified studies were evaluated for risk of bias by 2 investigators (RY and KF). For nonintervention studies, risk of bias was based on the JBI Critical Appraisal Checklist for prevalence studies.12 Exposures to medications were based on clear criteria widely used in the literature. The quality of the studies was graded based on the Cochrane methodology.13 Interventional studies measured similar outcomes and were graded by the Cochrane Effective Practice and Organization of Care criteria for nonrandomized and interrupted time series studies.14 Most measured process outcomes, not patient-oriented outcomes, such as whether the PCP altered a prescription based on a pharmacist's feedback or a drug allergy was not listed in the medical record.
Data Extraction and Synthesis
Preliminary data were abstracted onto an Excel spreadsheet. Four reviewers took different sections of the primary sheet for further extraction and arbitration independently (2 per subsection). Any discrepancies were further analyzed and discussed by all 4 reviewers (RY, AE, KF, NH), until consensus was reached.
There was significant heterogeneity in the countries of origin, measures of medication safety, and intensity and style of data collection, so it was not appropriate to combine the data using meta-analysis. In addition, this review did not aim to provide a definitive summary statistic for the frequency of medication safety events but rather to show the range in measures and estimates. We also did not attempt to standardize different outcome reporting rates (per prescription, clinic visit, or patient over some longer period of time) to a single measure. Rather, our primary results were expressed in the original units of each study and therefore provide an assessment of broad trends.
We did not predefine concepts such as “high-risk” but reported the descriptions provided by the identified studies. We did not register this study with a database such as PROSPERO.
Results
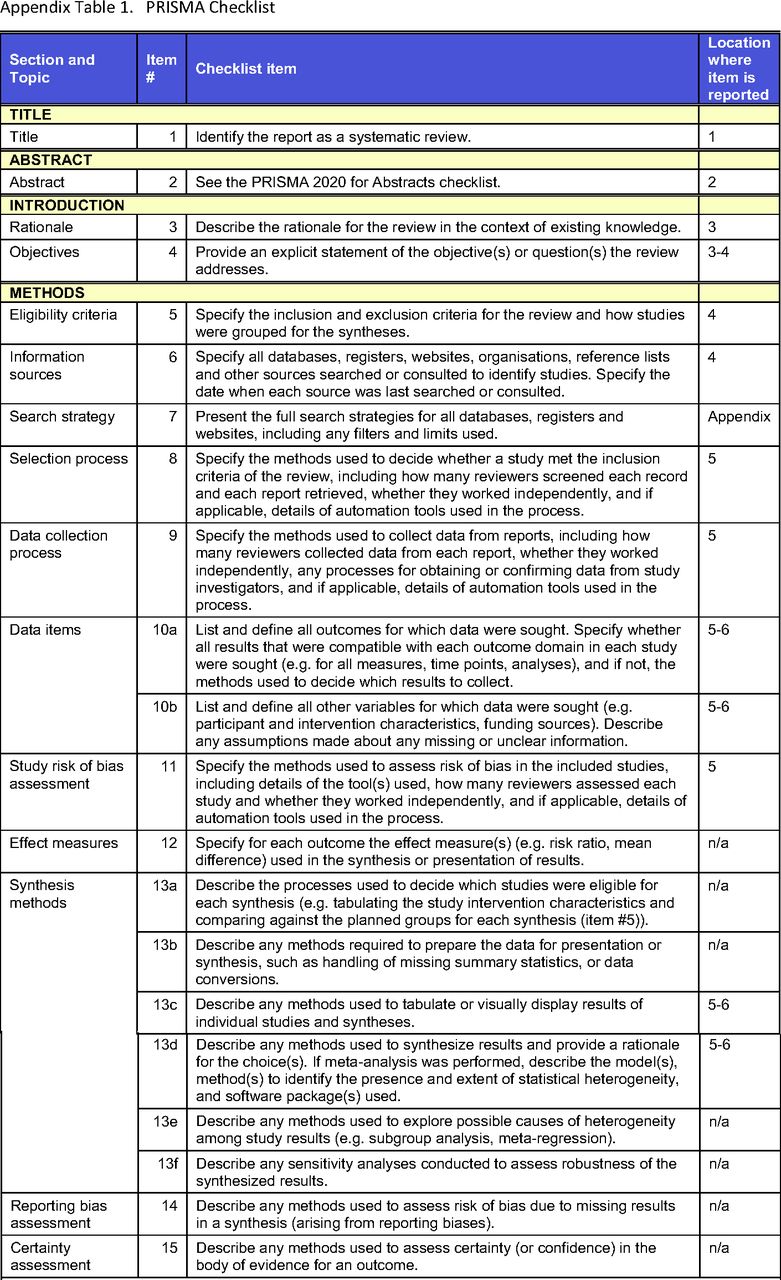
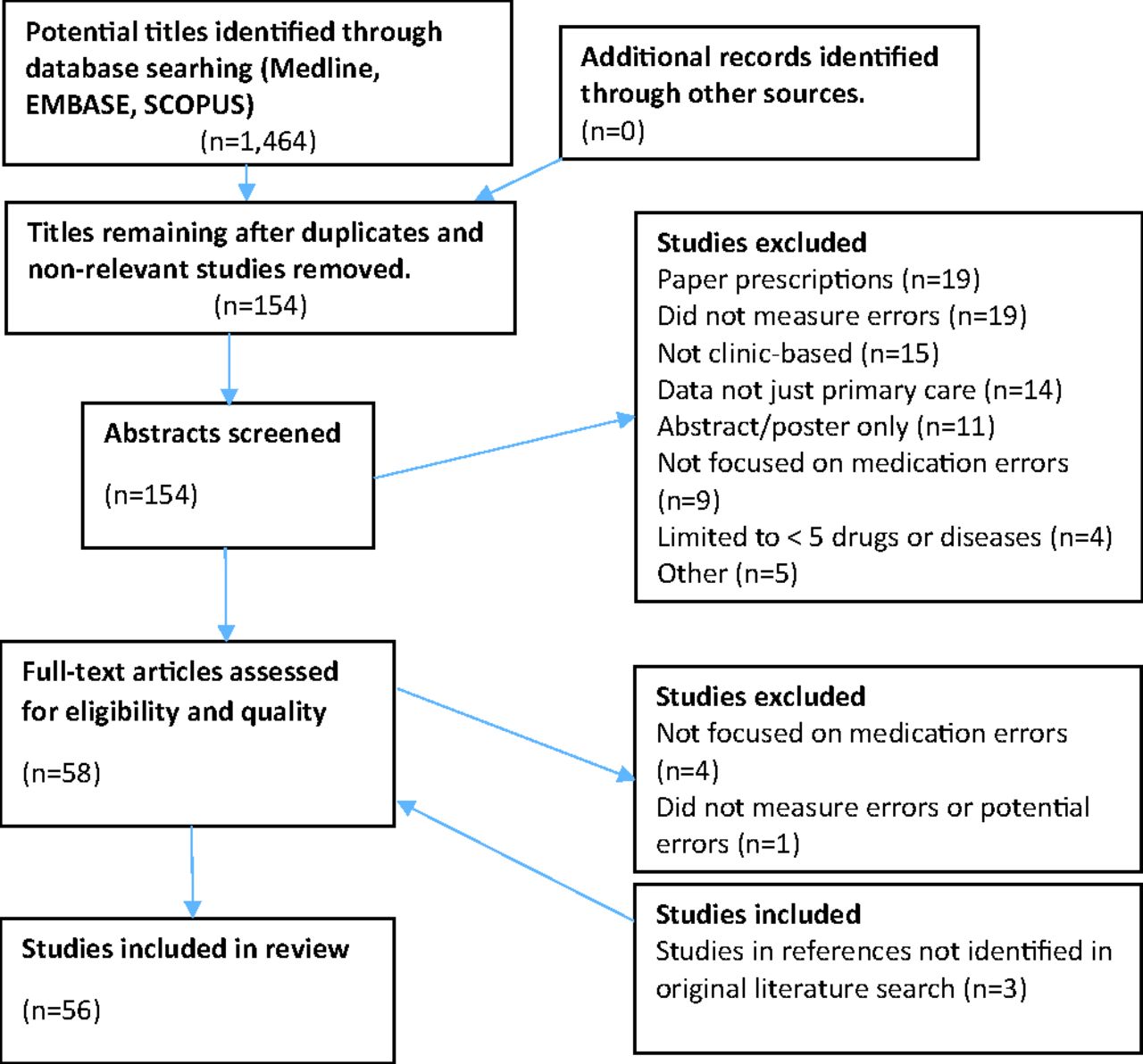
In all, 1464 articles appeared in the initial search. After reviewing titles, 154 articles were chosen for further review. Fifty-six articles met the search criteria and were included in the final analysis (PRISMA flowchart shown in Supplementary Figure 1).
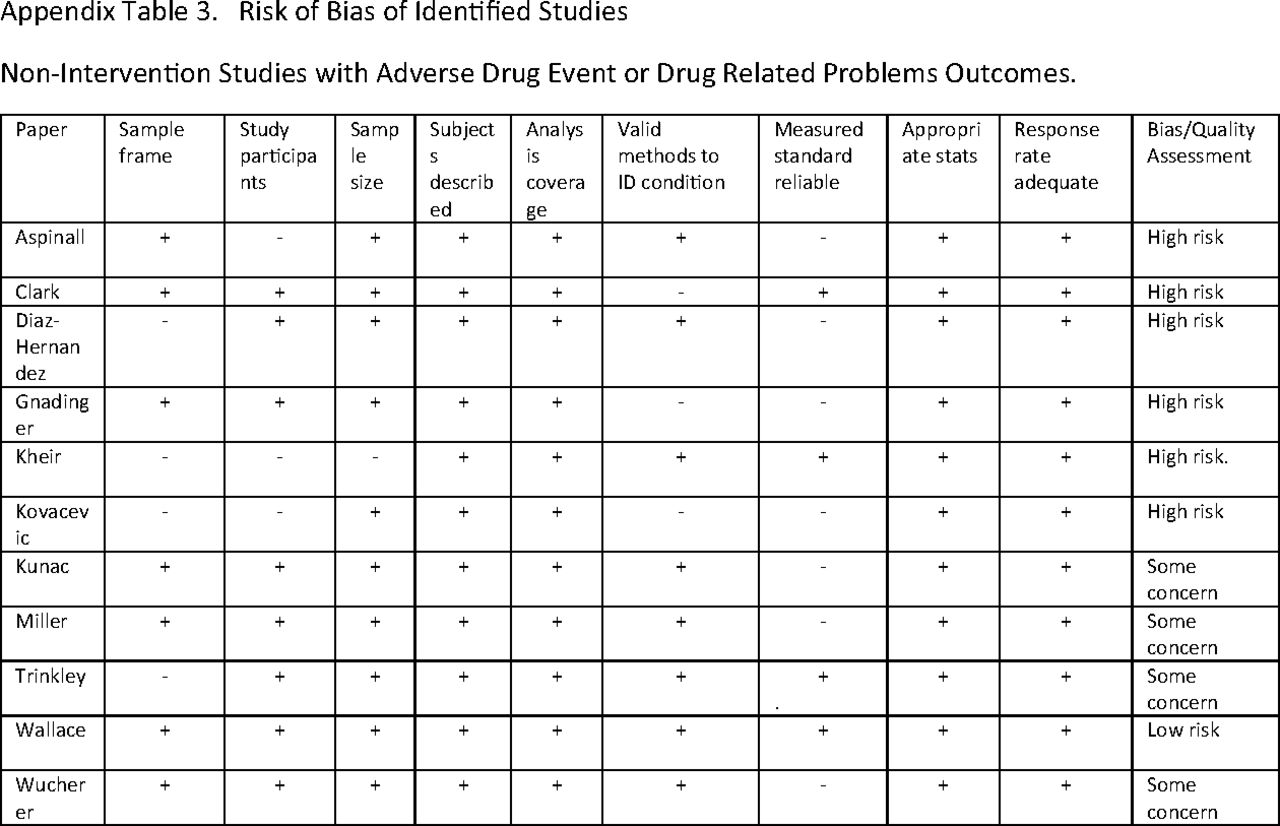
Forty-three studies were noninterventional (Table 1),15⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–58 and 13 included an intervention (Table 2).59⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–71 The noninterventional studies that measured potentially inappropriate prescribing/medications (PIPs) were all judged to be of low risk of bias because they included defined patient populations with clear process measure outcomes (whether or not a Beers list medication was on a patient's medication list, eg). The risk of bias assessment of noninterventional studies that measured ADEs or drug-related problems (DRPs) is shown in Supplementary Table 3. One of the 11 studies was judged to be of low risk of bias, 4 with some concern, 6 with a high risk of bias. Among the interventional studies, most also measured process outcomes, such as whether the PCP altered a prescription based on a pharmacist's feedback or a drug allergy was not listed in the medical record, not patient-oriented outcomes. The risk of bias table for each interventional study is presented in Supplementary Table 4. Only 1 study was judged to be of low risk of bias. The others had a high risk of bias.
Noninterventional Studies
Interventional Studies
The studies were performed all over the world: 31 in Europe,19,21,22,24⇓⇓⇓⇓⇓⇓⇓–32,38,39,41,46,51⇓⇓–54,56⇓–58,67 10 in the US,15,16,20,36,42,48,55,68⇓⇓–71 8 in Asia/the Middle East,17,23,34,35,40,43⇓–45 and 7 other.18,33,37,47,49,50,59 The majority of studies (30) used their own definition of error, often including some elements of the Beers or similar list.22,27,31⇓⇓⇓⇓⇓–37,39,40,43,44,46⇓⇓–49,54⇓–56,59⇓–61,63⇓⇓⇓⇓–68,71 Others used only the Beers list (14),17,18,23,25,38,41,42,45,50,52,53,56,69,70 screening tool of older persons' prescriptions (STOPP) (13),21,23,24,28⇓–30,41,50,51,53,56,57,62 screening tool to alert to right treatment (START) (5),21,28,30,41,57 and other definitions (9).15,16,19,20,26,52,56,58,64 The majority of the studies were in high-risk populations (defined by each study somewhat differently), generally patients ≥ age 60 and those taking ≥ 4 chronic medications (39).17⇓–19,21,23⇓⇓⇓⇓⇓⇓–30,33,36⇓–38,40⇓–42,45,46,50⇓⇓–53,56⇓⇓⇓⇓⇓⇓⇓⇓–65,67-71 The most common outcomes were PIPs (45),15⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–30,33⇓⇓⇓⇓–38,40⇓–42,44,45,50⇓⇓⇓–54,56⇓–58,60⇓⇓–63,65⇓–67,69-71 ADEs (12),20,32,36,39,44,47,49,55,56,58,64,68 and potential prescribing omissions (PPOs) (5).21,28,30,53,57
The rate of PIP varied widely (0.19% to 98.2% PIP rate overall; 4.9% to 98.2% for high-risk patients; 0.19% to 16% for a general patient population). The rate of ADE also varied widely (0.047% to 14.7% overall; 7.4% to 9.4% for high-risk patients; 0.047% to 14.7% for a general patient population). The ADE rate was sensitive to the method of data collection. Studies where physicians voluntarily reported ADEs to a registry had much lower rates (0.047% to 1.7%)32,39 than those collected by systematic or computerized record review (2.5% to 74%).20,36,55,56,58,64,68 The rate of PPO also varied widely (22.7% to 84.8%).21,28,30,53,57 The methods and results were too heterogeneous to quantitatively analyze (mainly due to different outcome measures used in defining medication errors in terms of PIPs, medication events, DRP, and other types; the outcomes were mainly reported as rates of medications reviewed but also included outcome frequencies per provider or per patient that were not convertible to rates.) In general, higher rates of PIP were found in studies of high-risk populations that incorporated multiple measurements of medication usage for each patient (1 year of clinic records, eg). Smaller PIP rates were seen in studies of general primary care populations over shorter time frames (examining the medication list in the EHR at 1 clinic visit or the prescriptions generated from 1 clinic visit).
A small subset of the studies (6/56 [10.7%]) reported actual harms (Clark et al32 reported adverse drug reactions but provided no further detail on harms.).20,29,49,55,56,64 In a study that may have included events not originating from the primary care clinic, 55/8171 (0.67%) of patients reported a severe ADE in the past 6 months and were hospitalized as a result (the hospitalization estimate was calculated from numbers in the article that only included 1 of 3 study periods).49 General practitioners judged 23.2% of the ADEs to be preventable. Another study, using its own definition of ADE, concluded that all ADEs were significant, and 0.2% of patients suffered a “serious or life-threatening” ADE (this is a good example of the subjectivity of these ADE measurements—in 1 of the 2 cases, the patient passed out and fell after a medication dose was reduced; in the other, a patient with a history of falls fell, went to the ED, and the X-rays were normal).55 A study using its own definition of ADE calculated that 1.7% of prescriptions had any level of ADE, with no further reporting of actual harm.32 Another study using its own definition of a medication incident reported an ADE rate of 0.047% of physician-patient contacts over 1 year.39
Three noninterventional studies correlated PIP findings with actual harm. One found no association between patients with ≥ 2 PIPs and harms such as ADEs, reduced quality of life, ED visits, or hospital admissions.56 One found an association between ≥ 2 PIP and a lower mean health-related quality of life utility (adjusted coefficient −0.09, SE 0.02, P < .001) and an increased risk in the expected rate of ED visits (adjusted IRR 1.85; 95% CI 1.32, 2.58, P < .001) but no difference in hospitalizations or other outcomes.29 One study in frail elderly greater than 80 years of age found an adjusted increased risk of hospitalization (HR 1.26) and mortality (HR 1.39) for underuse of medications but not overuse.57
One intervention study measured patient harms and found that the intervention had no impact on hospitalizations.64 Most intervention studies involved pharmacists reviewing patient charts or pharmacy data and making recommendations to the physicians, which were accepted to varying degrees (25% to 70%),59⇓–61,63⇓–65,67,68 less so with automated EHR reminders (5% to 21%).66,69 These recommendations were mostly process changes such as adding indications for the medications or ordering lab tests for routine monitoring.
No studies in our review considered patient shared decision-making processes or cases where patients accepted a degree of risk from a medication to achieve another goal more important to the patient. No studies measured other aspects of harms reported by patients in other studies to be important such as emotional discomfort;72,73 wasted time for patients, physicians, and the health care system;72,74,75 loss of relationship and trust in the clinician;73 and financial costs to patients, clinicians, and the health care system.74,75
Discussion
We found that actual harm from medication errors in primary care, versus potential for harm, is much lower than is commonly quoted (or projected) and rarely results in ED visits or hospital admissions. The existing literature does not take into account shared patient decision-making, accepted risk-benefit trade-offs, or deprescribing goals in the elderly, nor does it measure other patient-centered outcomes such as patient and caregiver hassles, cost, and loss of trust with the primary care team. The ranges of reported ADE and medication error rates illustrate the inadequacies of current evidence to suggest both the scope of medication error-related harms as well as how medication errors should be defined.
Limitations
There are limitations to the literature and our analysis. Most identified studies only measured PIPs and not patient harms. Medication lists were obtained from available clinic or national pharmacy records. There may have been discrepancies between the electronic reports and the medications that PCPs and patients considered to be the active list. In other studies, as many as 90% of the patients at home were found to have inaccurate medication information in their chart,76 and nearly half of patients experienced medication discrepancies during care transitions.77,78 We attempted to limit studies to only those where the chronic and acute medications were prescribed by PCPs. In studies using national pharmacy databases, it is possible that some of the prescriptions were written by non-PCPs. The studies also did not make distinctions between medications that were on the patients' medication lists that were heavily influenced by non-PCP physicians versus medications originally prescribed by the PCPs. The majority of studies self-described their patient populations as “high-risk,” though there were many variations of that definition.
Our study was limited to only the medication list and prescribing in the primary care center. We did not include other sources of medication safety concerns in primary care such as transitions from hospital or rehabilitation facilities. Therefore, our review might have missed important sources of medication safety concerns related to primary care. We limited our searches to our definition of studies in the EHR era. It is possible that relevant studies were missed using this strategy. We limited our searches to primary care terms. It is possible that relevant studies were conducted in primary care settings that did not use that keyword or a similar keyword such as family medicine. Our review did not include studies that defined a medication error as a chronic disease goal not achieved (such as a hemoglobin A1c for a diabetic patient)79 or where laboratory monitoring for adverse drug effects did not occur.80
Implications for Practice, Policy, and Future Research
When viewing harms from a patient's perspective, Kuzel et al found that 70% of reported harms were psychological, including anger, frustration, belittlement, and loss of relationship and trust in one's clinician, which are in contrast with physical harms such as pain, bruising, worsening medical condition, emergency visits, and hospitalizations.73 Such psychological harms were not reported in the studies in our review. Kuzel et al concluded that errors reported by interviewed patients suggest that breakdowns in access to and relationships with clinicians may be more prominent medical errors than technical errors in diagnosis and treatment.73
Perhaps medication safety should not even be conceptualized as complying with recommendations from medication lists such as Beers, STOPP, or START. Lai et al interviewed frontline clinicians and patients and found in both groups that safety was conceptualized more in terms of work functions involving grouping of tasks or responsibilities, rather than domains such as medications, diagnoses, care transitions, referrals, and testing.81 In addition not considered in the literature is the critical roles of patients and families beyond the prescribing actions by family physician. Review of hypoglycemic events resulting in ED visits showed that the most common precipitants were reduced food intake and administration of the wrong insulin product.82
A commonly used definition of an ADE was that there was at least a 50% chance that the symptom was related to the medication in question. However, most of the reported ADEs were mild, such as bruising when taking warfarin or constipation when taking a calcium channel blocker. Similar to our study focused on the primary care clinic, a recent randomized trial of care transitions from hospital to primary care found that in-home assessments by pharmacists with communication to the primary care team made no impact on ADEs or medication errors.83
In the intervention studies, we found that the impact on a prescriber to change medications is greater if there is personal communication by the pharmacist and the change requested by the pharmacist is relatively minor (such as adding the indication to the prescription or updating the medication list in the EHR) and uncommonly impacts major prescribing decisions such as whether the patient should take a drug at all. Perhaps shared decision-making processes help explain why PCPs ignore most computerized drug alerts84⇓–86 and why the intervention studies identified in this review made little to no impact on PIP rates. Even high-risk medications such as benzodiazepines are helpful in selective elderly patients, where the benefits likely outweigh the risks.87
Other studies of ambulatory care outside of primary care have measured actual harms. For example, Gandhi et al estimated that rates of life-threatening ADEs in a multispecialty group were 138/1000 person-years, but that only 11% were preventable.88 Most of the root causes of the preventable cases were patients that did not take their medications as prescribed, not PIP by prescribers.
Our findings share some conclusions with other reviews on medication safety in primary care, including most medication errors are “not clinically important”;89 ADEs are not usually preventable;90 computer decision support inconsistently affects PIP rates with no evidence it reduces patient harms91 and actually creates new sources of error such as alarm fatigue;92 and the variance of reported “medication errors” is large and a function of patient populations, methods, definitions, and the parts of the system studied—and interventions make little difference.93 Medication safety is not measured well with ADEs, because many are expected side effects of the medications and are not preventable. Safety is better conceptualized as a series of actions to perform, which is more analogous to aviation safety, and is consistent with how frontline primary care teams conceptualize safety.81 Our review confirms other observations that potential medication errors do not usually result in injuries or fatal outcomes,94 and conversely, just because a patient experienced an ADE does not mean that a medication error occurred. The Agency for Healthcare Research and Quality (AHRQ) first highlighted these distinctions in 2019, adding subcategories to ADEs such as preventable, potential, ameliorable, and nonpreventable.95 The vast majority of studies in our sample do not make these distinctions.
EHR-focused studies have found that alerts are ignored by physicians 90% of the time in adult ambulatory care,84 and acceptance rates of alternative recommendations to potentially inappropriate medications followed only 11.1% of the time.86 EHR alerts for coprescribing high-risk medication combinations such as benzodiazepines and opioids did not change prescribing practices.85 EHRs were found to be the root cause of medical errors at high risk for an adverse event in 14% of reported cases in an embedded practice-based anonymous reporting system.96 In summary, our review and other evidence concludes that alerts from computers suggesting medication changes to clinicians are most often ignored, implying that there are likely good reasons for patients to be on medications that computerized algorithms flag as high risk.97
Future for Primary Care Medication Safety Research
We make the following recommendations for future research and practice of medication safety in primary care.
All studies purporting to measure preventable ADEs (to use the AHRQ definitions) in the future should:
Include chart reviews of flagged cases. Potentially inappropriate prescribing rarely leads to actual physical harm.
Take into consideration patient shared decision-making, acceptance of risk-benefit trade-offs, and deprescribing goals in elderly patients and do not count these decisions as medical errors. Deprescribing is complex. Few studies have examined the success rate and safety of deprescribing, and there is a risk of relapse of symptoms.98 Deeper consideration should also be given to the critical roles of patients and families beyond the prescribing actions by PCP.
Include patient harms such as psychological injury, wasted time, unnecessary trips to health care facilities, and increased costs. To adjudicate and measure these outcomes, individual chart reviews will likely be necessary with judgement calls made by clinicians for each potential case. Also, patients can be asked directly if they believe their medications may be causing illness.99
For primary care practices trying to improve the quality of their care, voluntary reporting systems for clinicians, staff, and patients are feasible to guide understanding of potential quality improvement themes, though they are unreliable for absolute measures of errors or harms. Confidential reports appear to be superior to anonymous reports and may be more useful in understanding errors and designing interventions to improve patient safety.100
Primary care offices could possibly be made safer by changing work flows, improving the hectic environment, and allowing the primary care teams to have more time to review medication concerns.101 For example, a study examining how receptionists and general practitioners interact found potential sources of error that could be reduced with improved communication.102
Future studies designed to measure the effects of interventions on more serious physical harms caused by preventable ADEs will require thousands of high-risk patients, as rates are expected to be less than 1% of the study population per year.
There may be a role for a core outcome set to be developed for primary care medication safety (www.comet-initiative.org). The complexity of primary care and multifaceted nature of primary care prescribing outcomes make this a difficult task.
Appendix




Notes
This article was externally peer reviewed.
Funding: Agency for Health Care Research and Quality.
PROMIS Learning Lab: Partnership in Resilience for Medication Safety Federal Award Identification Number (FAIN): 1R18HS027277-01.
Conflict of interest: RAY discloses that he is the sole owner of SENTIRE, LLC, which is a novel documentation, coding, and billing system for primary care. The other authors report no conflicts.
To see this article online, please go to: http://jabfm.org/content/35/3/610.full.
- Received for publication August 9, 2021.
- Revision received December 27, 2021.
- Accepted for publication January 10, 2022.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}