
Article Figures & Data
Figures
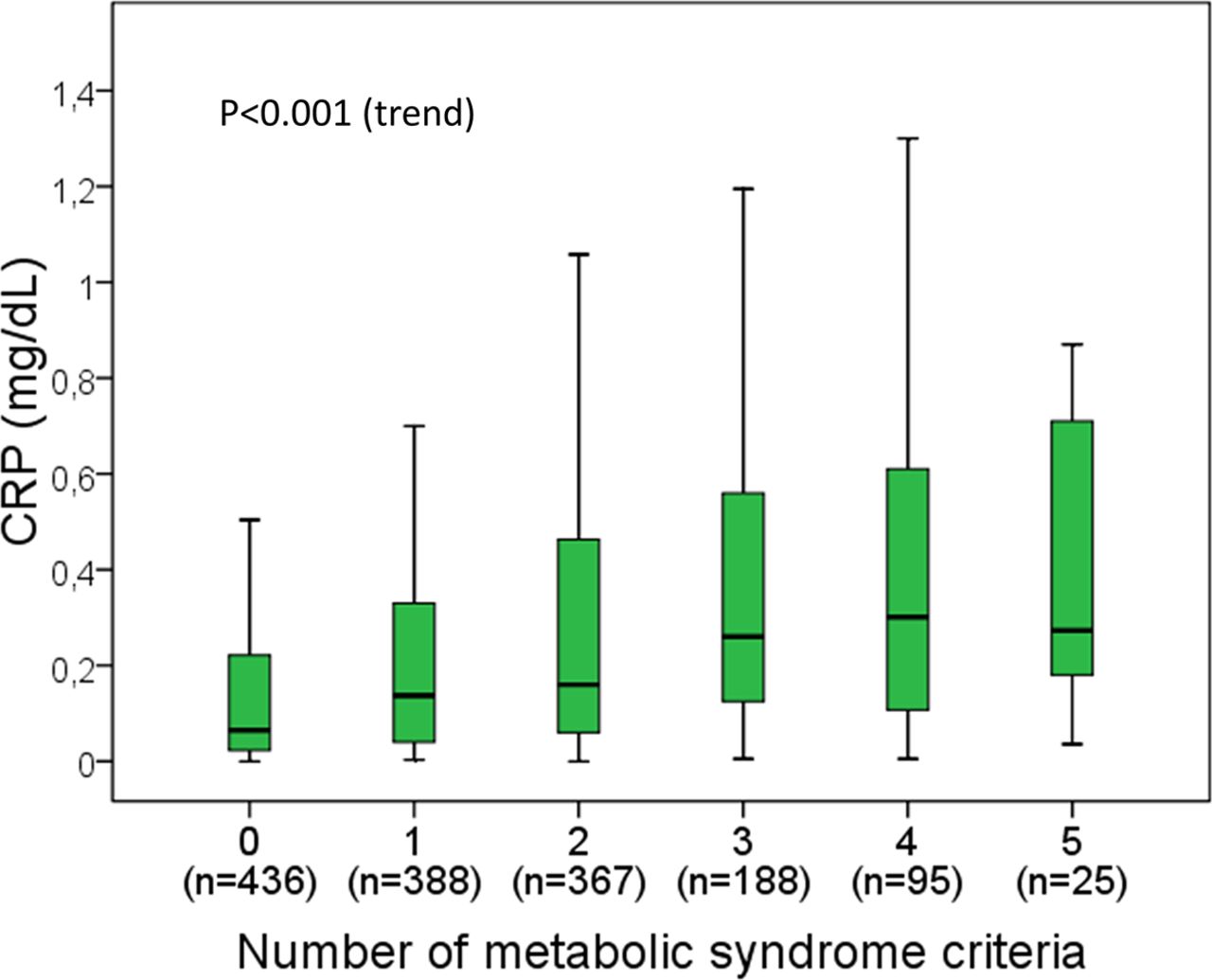
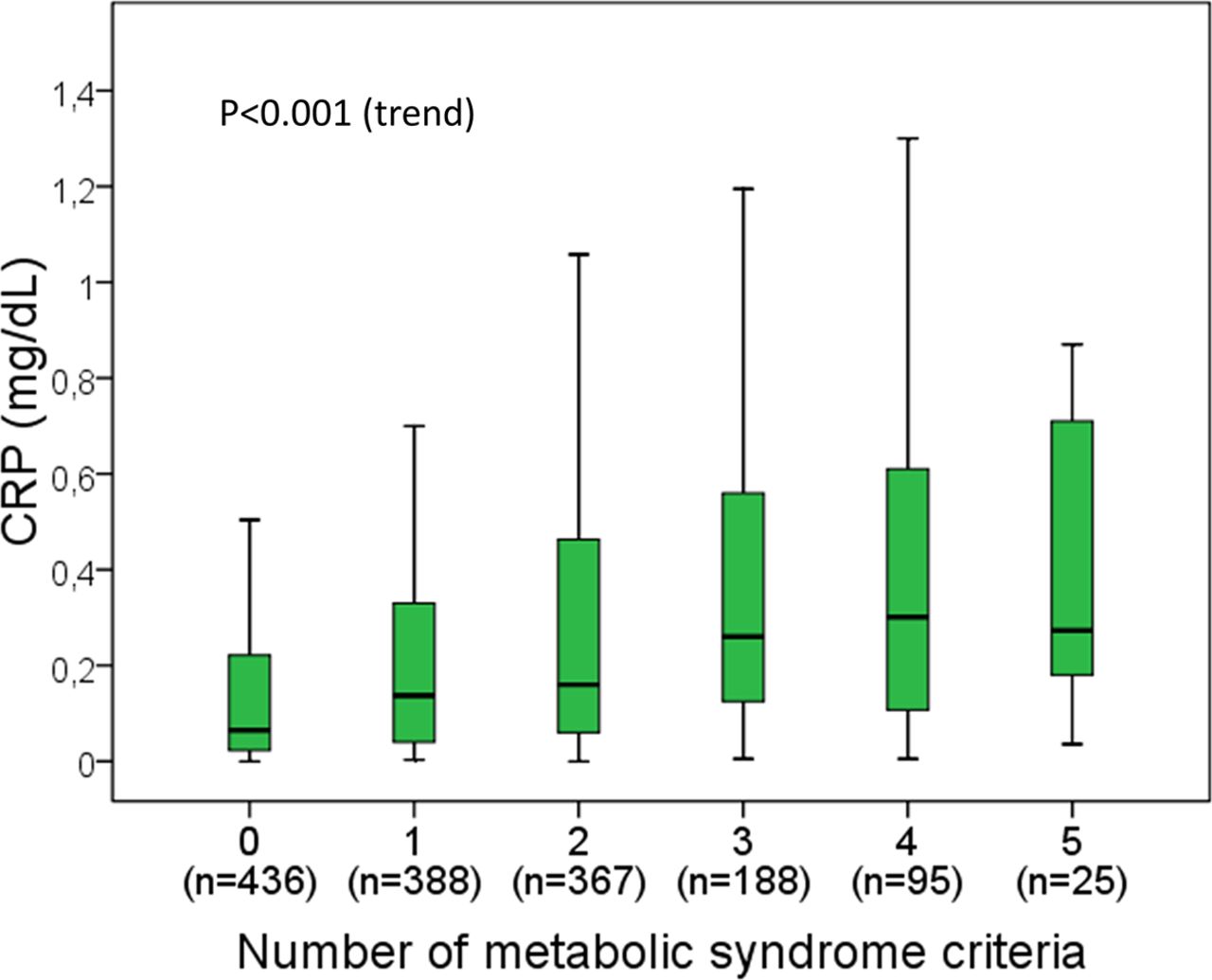
- Figure 1.
Boxplot of serum C-reactive protein concentrations in relation to the number of metabolic syndrome criteria. Outliers (values outside 1.5 times the interquartile range above the upper quartile and below the lower quartile) are not represented but are included in the analyses. P value was obtained with the Jonckheere-Terpstra trend test.
Tables
- Table 1.
C-Reactive Protein Concentrations According to Demographics, Lifestyle Factors, and Metabolic Abnormalities*
Factor N CRP (mg/dL) P value Sex Female 830 0.14 (0.04–0.42) Reference Male 669 0.13 (0.04–0.33) .186 Age (years) 18–35 295 0.09 (0.03–0.33) Reference >35–50 408 0.11 (0.04–0.35) .033 >50–65 388 0.17 (0.06–0.39) <.001 >65 408 0.18 (0.06–0.47) <.001 Alcohol consumption Abstainers 539 0.16 (0.05–0.46) Reference Light drinkers 591 0.11 (0.03–0.33) <.001 Moderate drinkers 239 0.15 (0.04–0.37) .146 Heavy drinkers 130 0.17 (0.08–0.43) .363 Smoking Never smokers 820 0.15 (0.05–0.41) Reference Ex-smokers 388 0.13 (0.04–0.34) .127 Current smokers 291 0.13 (0.04–0.36) .183 Physical activity Low 583 0.16 (0.05–0.46) Reference Moderate 548 0.14 (0.04–0.36) .017 High 368 0.11 (0.04–0.33) .005 Body mass index Normal weight 421 0.06 (0.02–0.17) Reference Overweight 567 0.13 (0.05–0.36) <.001 Obesity 511 0.25 (0.10–0.55) <.001 Metabolic syndrome No 1191 0.11 (0.04–0.33) Reference Yes 308 0.27 (0.12–0.59) <.001 CRP, C-reactive protein.
↵* Data are medians and interquartile (25th–75th percentile) ranges (in brackets). The normal range for serum CRP concentrations is 0–0.5 mg/dL (0–5 mg/L).
- Table 2.
Multivariate Analysis. Linear Regression of C-Reactive Protein (log10-Transformed) in Relation to Demographics, Lifestyle Factors, and Metabolic Factors
Factor Coefficient (SE) P value Sex (male) Female Reference NA Male −0.050 (0.035) .157 Age (years) 0.002 (0.001) .087 Alcohol consumption Abstainers Reference NA Light drinkers −0.114 (0.036) .001 Moderate drinkers −0.090 (0.048) .061 Heavy drinkers 0.013 (0.062) .829 Smoking Never smokers Reference NA Ex-smokers −0.029 (0.038) .445 Current smokers 0.087 (0.043) .042 Physical activity Low Reference NA Moderate −0.033 (0.035) .348 High −0.014 (0.040) .725 Body mass index (kg/m2) 0.045 (0.003) <.001 Metabolic syndrome No Reference NA Yes 0.073 (0.042) .084 Constant (intercept) −2.178 (0.107) NA CRP, C-reactive protein; NA, not applicable; SE, standard error.
* For the logarithmic transformation, we attributed an arbitrary value of 0.001 mg/dL to patients with undetectable CRP (n = 4).
† All listed covariates were entered into the equation.
‡ Covariates explained 17.4% of the CRP variability (R2, 0.174). The body mass index explained 15.7% of the CRP variability.
- Table 3.
Comparison of Demographics, Lifestyle Factors, Metabolic Abnormalities among Categories of Agreement and Discordance between C-Reactive Protein and Erythrocyte Sedimentation Rate Values
Factor Normal CRP Normal ESR (n = 1123) High ESR Normal CRP (n = 72) High CRP Normal ESR (n = 208) High CRP High ESR (n = 69) Sex (male)II 514 (45.8) 30 (41.7) 78 (37.5)* 33 (47.8) Age (years)¶ 50 (37–65) 64 (55–74)‡ 55 (42–67)† 64 (49–76)‡ Alcohol consumption (g/week)¶ 30 (3–130) 20 (3–85) 10 (3–90)* 13 (3–140) Smoking (current)II 223 (19.9) 12 (16.7) 36 (17.3) 11 (15.9) Physical activity (low)II 411 (36.6) 31 (43.1) 91 (43.8) 40 (58.0)‡ Body mass index (kg/m2)¶ 27.2 (23.9–30.6) 28.1 (25.4–31.7)* 30.0 (26.2–33.7)‡ 32.0 (27.0–35.6)‡ Metabolic syndrome (yes)II 185 (16.5) 24 (33.3)‡ 68 (32.7)‡ 23 (33.3)‡ Serum IL-6 (pg/mL)¶ <2 (<2–3.0) 2.2 (<2–4.1) 3.0 (<2–4.9)‡ 4.7 (2.3–8.7)‡ CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
↵* P < .05;
↵† P < .01; and
↵‡ P < .001 compared with the reference category (individuals with normal CRP and normal ESR).
fData available for 1472 individuals.
§ High CRP is defined as >0.5 mg/dL (>5 mg/L); high ESR is defined as >20 mm/h for men and >30 mm/h for women.
↵II Figures for sex, smoking, physical activity, and metabolic syndrome are absolute numbers and percentages (within parentheses).
↵¶ Figures for age, alcohol consumption, body mass index, and serum IL-6 are medians and interquartile ranges (within parentheses).
- Table 4.
Multivariate Analysis (Logistic Regression) of Factors Associated with Discordance between C-Reactive Protein and Erythrocyte Sedimentation Rate*,†
High ESR and normal CRP (n = 72) High CRP and normal ESR (n = 208) Factor OR (95% CI) P value OR (95% CI) P value Sex (male) 0.815 (0.448–1.481) .502 0.699 (0.483–1.012) .058 Age (years) 1.052 (1.034–1.071) <.001 0.998 (0.988–1.008) .695 Body mass index (kg/m2) 0.986 (0.930–1.045) .633 1.099 (1.064–1.136) <.001 CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; OR, odds ratio.
↵* High CRP is defined as >0.5 mg/dL (>5 mg/L); high ESR is defined as >20 mm/h for men and >30 mm/h for women.
↵† A total of 1472 cases were entered into the equations. The odds ratio (adjusted for all listed variables and alcohol consumption, smoking, metabolic syndrome, and physical activity).
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Re: C-Reactive Protein versus Erythrocyte Sedimentation Rate: Implications Among Patients with No Known Inflammatory Conditions
- Response: Re: C-Reactive Protein versus Erythrocyte Sedimentation Rate: Implications Among Patients with No Known Inflammatory Conditions
- Practical Clinical Topics, Digging Deeper into COVID-19, Social Determinants of Health, and Equity