
Article Figures & Data
Figures
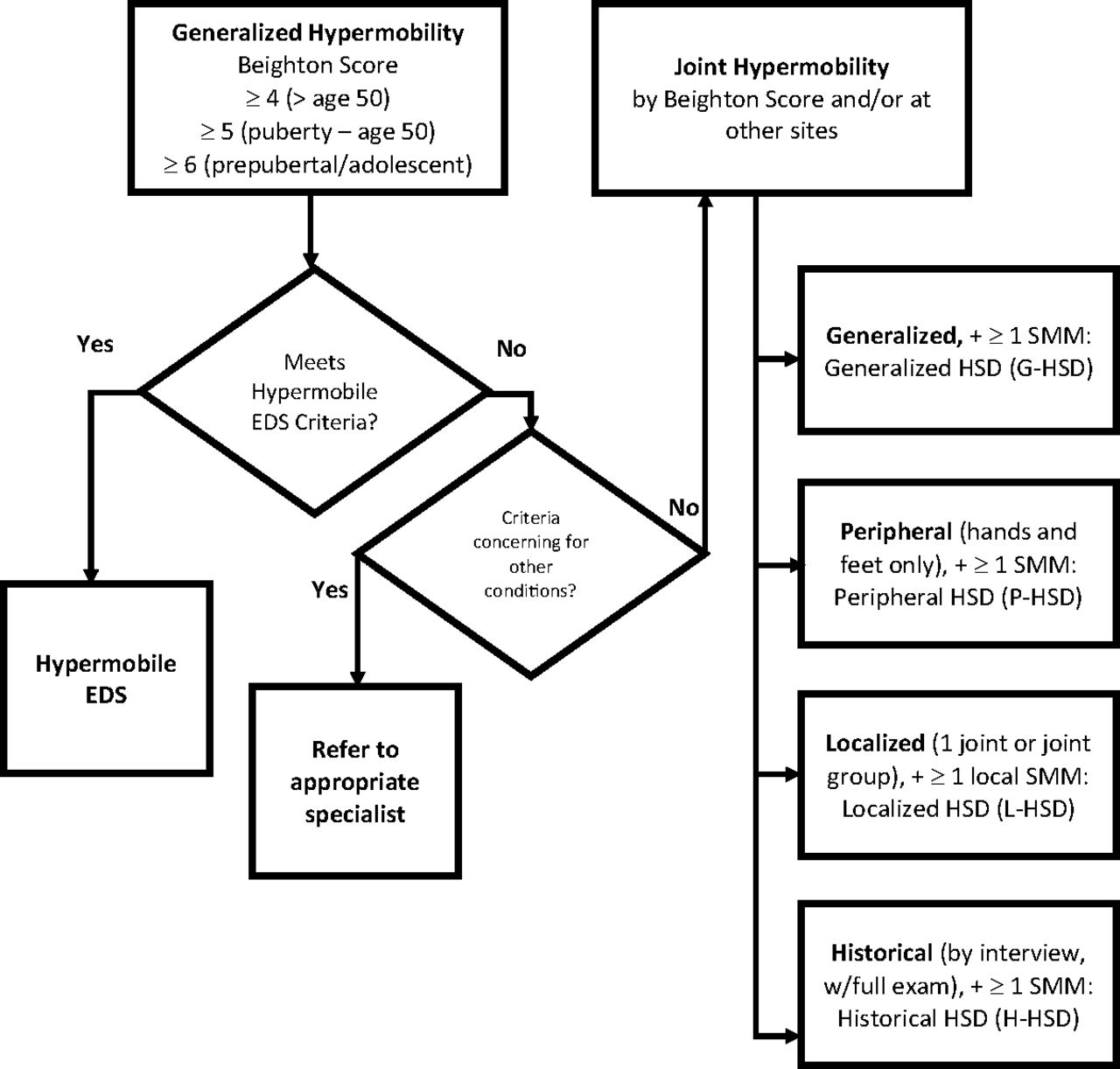
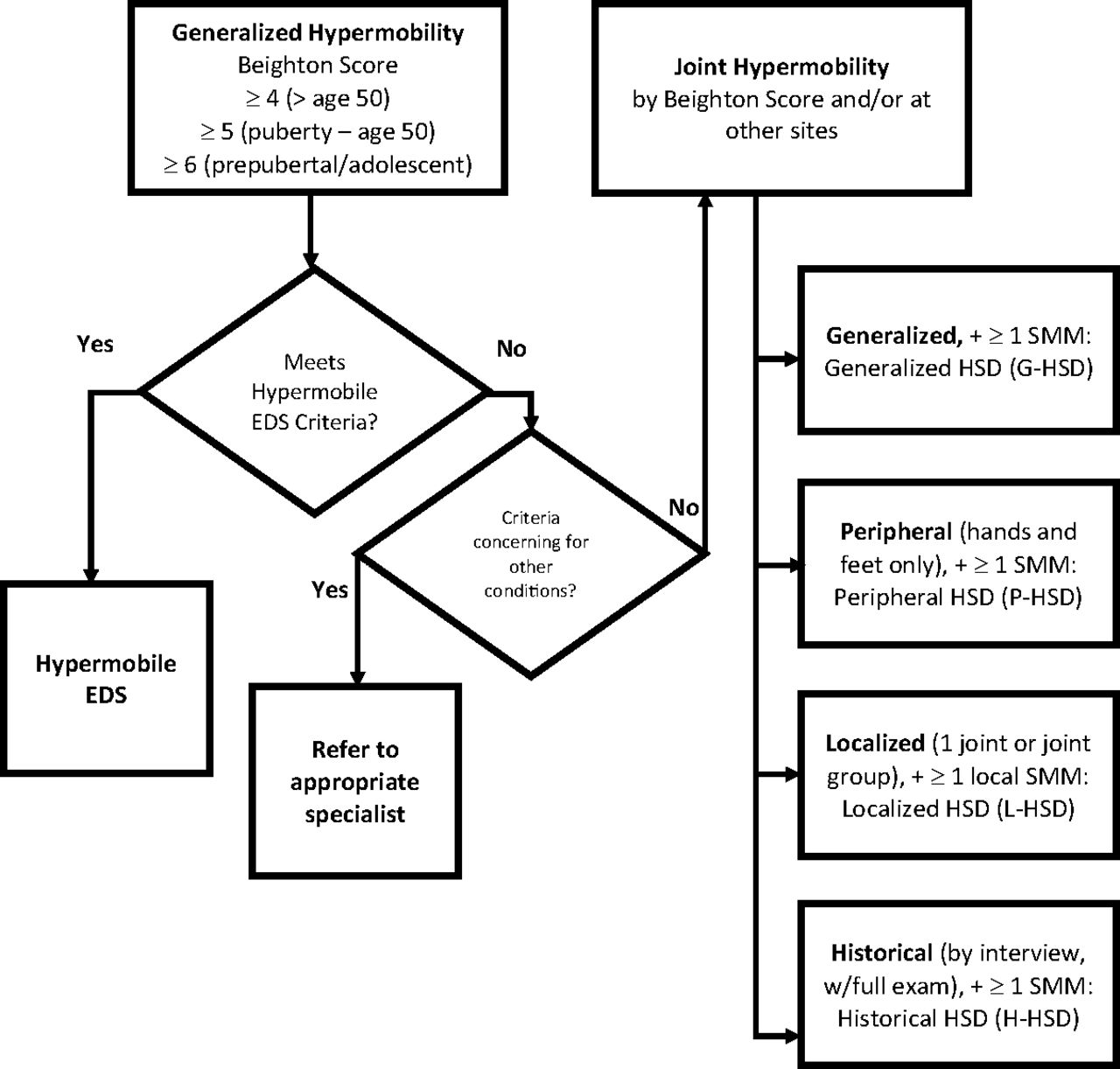
- Figure 1.
Diagnosing disorders of joint hypermobility: distinguishing hypermobile Ehlers-Danlos syndrome and the hypermobility spectrum disorders. Abbreviations: hEDS, hypermobile Ehlers-Danlos syndrome; EDS, Ehlers-Danlos syndrome; HSD, Hypermobility spectrum disorder.
Tables
Can you now (or could you ever) place your hands flat on the floor without bending your knees?
Can you now (or could you ever) bend your thumb to touch your forearm?
As a child, did you amuse your friend by contorting your body into strange shapes or could you do the splits?
As a child or teenager, did your kneecap or shoulder dislocate on more than one occasion?
Do you consider yourself double jointed?
Adapted from Hakim and Grahame. R.1 Can place hands flat on the floor without bending the knees 1 point Right Left Can passively dorsiflex the fifth metacarpophalangeal joint to 90° or greater 1 point 1 point Can oppose the thumb to volar aspect of forearm 1 point 1 point Can hyperextend the elbow 10° or more 1 point 1 point Can hyperextend the knee 10° or more 1 point 1 point Adapted from Fikree et al. 2 Criterion 1—generalized joint hypermobility Beighton score __/9 · ≥ 6 for prepubertal children and adolescents · ≥ 5 for pubertal men and woman to age 50 · ≥ 4 for men and women over age 50 If Beighton score is 1 point below age-specific cutoff, affirmative answer to 2 of the following questions will meet criterion 1. · Can you now (or could you ever) place your hands flat on the floor without bending your knees? · Can you now (or could you ever) bend your thumb to touch your forearm? · As a child, did you amuse your friends by contorting your body into strange shapes or could you do the splits? · As a child or teenager did your shoulder or kneecap dislocate on more than one occasion? · Do you consider yourself “double jointed”? Criterion 2—2 or more of the following (A, B, or C) must be present Feature A (5 must be present)
· Unusually soft or velvety skin
· Mild skin hyperextensibility
· Unexplained striae distensae or rubae at the back, groins, thighs, breasts, and/or abdomen in adolescence, men or prepubertal women without a significant gain or loss of body fat or weight
· Bilateral piezogenic papules of the heel
· Recurrent or multiple abdominal hernia(s)
· Atrophic scarring involving at least 2 sites and without the formation of truly papyraceous and/or hemosideric scars as seen in classical EDS· Pelvic floor, rectal, and/or uterine prolapse in children, men, or nulliparous women without a history of morbid obesity or other known predisposing medical condition
· Dental crowding and high or narrow palate
· Arachnodactyly, as defined in one or more of the following: (1) positive wrist sign (Walker sign) on both sides, (2) positive thumb sign (Steinberg sign) on both sides
· Arm span-to-height ratio >/= 1.05
· Mitral valve prolapse mild or greater based on strict echocardiographic criteria
· Aortic root dilation with Z-score > +2
Feature B
· Positive family history; 1 or more first-degree relatives independently meeting the current criteria for hEDS
Feature C (must have at least 1)
· Musculoskeletal pain in 2 or more limbs, recurring daily for at least 3 months
· Chronic, widespread pain for >/= 3 months
· Recurrent joint dislocations or frank joint instability, in the absence of traumaCriterion 3—all of the following prerequisites MUST be met · Absence of unusual skin fragility, which should prompt consideration of other types of EDS · Exclusion of other heritable and acquired connective tissue disorders (CTDs), including autoimmune rheumatologic conditions. In patients with an acquired CTD (eg, lupus, rheumatoid arthritis, etc), additional diagnosis of hEDS requires meeting both features A and B of criterion 2 (chronic and/or instability) cannot be counted toward a diagnosis of hEDS in this situation. · Exclusion of alternative diagnoses that may also include joint hypermobility by means of hypotonia and/or connective tissue laxity. Alternative diagnoses and diagnostic categories include, but are not limited to, neuromuscular disorder (eg, Bethlem myopathy), other hereditary disorders of the connective tissue (eg, other types of EDS, Loeys-Dietz syndrome, Marfan syndrome), and skeletal dysplasias (eg, osteogenesis imperfecta). Exclusion of these considerations may be based upon history, physical examination, and/or molecular genetics testing, as indicated. Skin hyperextensibility
Velvety skin texture
Striae (stretch marks)
Easy bruising
Prolonged bleeding (with normal coagulation workup)
Poor wound healing
Atrophic-appearing scars (wide, papery, hypopigmented)
Neurologic Migraine headache
Tension-type headache
Dysautonomia
Postural orthostatic tachycardia syndrome
Upper limb paresthesias (carpal or cubital tunnel syndromes, thoracic outlet syndrome)
Gastrointestinal Abdominal pain
Hiatal hernia
Gastroesophageal reflux disease
Irritable bowel syndrome
Dysphagia
Nausea
Constipation
Crohn's disease
Psychiatric Anxiety
Depression
Insomnia
Gynecologic Pelvic pain
Dysmenorrhea
Urinary stress and/or urge incontinence
Other Temporomandibular joint disorders
Chronic fatigue syndrome
Exercise intolerance
Postexercise malaise
HSD, Hypermobility spectrum disorder.
Case 1 Follow-up
You diagnose Jennifer with Probable hEDS. You get an echocardiogram and an ophthalmologic exam, which are both normal, making a diagnosis of Marfan syndrome unlikely. You discuss possible referral to a genetic counselor with her family, but decide against referral due to the normal exams. The consensus with the family following the meeting is that Jennifer has a presentation consistent with hEDS, for which she meets the 2017 international diagnostic criteria. You refer Jennifer to occupational and physical therapy with an emphasis on postural stabilization and joint protection, avoiding most resistance and isometric exercises. She follows up in 1 month and describes mild improvement in her symptoms. You decide to continue with the current management.Case 2 Follow-up You diagnose Sonja with HSD and refer her to a physical therapist with experience working with HSD patients, to focus on core stability and exercise tolerance. Additionally, she enters a course of osteopathic manipulative treatment, twice monthly for 3 months, and is restarted on and titrated to a higher dose of duloxetine (60 mg/d) to address central pain sensitization and improve mood. She is referred for cognitive-behavioral therapy (CBT) to address anxiety and improve coping strategies. On follow-up 3 months later, she reports significant improvement, with resolution of headaches and brain fog. Her fatigue has improved but not resolved. She continues to suffer from neck and back pain, though with decreased severity and frequency. She feels optimistic that with continued physical therapy, CBT, adequate rest, progressive exercise, and osteopathic treatment, she has found a path forward that promises to empower her to manage her symptoms. She understands that HSD will make her more prone to repetitive stress injury and the importance of maintaining an active lifestyle, including regular stability and core strengthening. HSD hEDS EDS, Other Joint hypermobility • • • Chronic pain • • • Musculoskeletal pain in more than 2 limbs, back ≥ 3 months • • • Recurrent joint dislocations • • • Recurrent hernias, uterine and rectal prolapse • • • Marfanoid habitus • • • Mild skin hyperextensibility, striae, atrophic scarring • • • Skin fragility, pronounced hyperextensibility • Cardiovascular autonomic dysfunction • • • Mild cardiovascular findings (mild mitral valve regurgitation, aortic root dilation) • • Severe cardiovascular findings (aneurysms, arterial rupture) • Positive family history • • Molecular genetic findings • HSD, Hypermobility spectrum disorder; hEDS, hypermobile Ehlers-Danlos syndrome; EDS, Ehlers-Danlos syndrome.
Modality Comments Joint braces and musculoskeletal taping May help stabilize joints Biofeedback to improve posture Improve joint symptoms and proprioception Osteopathic manipulative treatment Reduce joint pain, improve proprioception, increase blood flow. Avoid treatment more than 3 times per week due to potential for increasing joint laxity. Prolotherapy Injections in the tendon or ligamentous attachment can trigger a brief inflammatory response and subsequent reparative cascade to generate new collagen and strengthening the relaxed connective tissue. May also reduce pain from increased joint stability. TENS unit May be helpful for muscle pain Compressive clothing Compression stockings may help combat orthostatic intolerance and tachycardia. Compression garments may help support loose joints and provide additional proprioceptive input. Orthotic shoe inserts May improve underlying proprioceptive abnormalities, improve ankle/foot/knee alignment, reduce joint pain and risk of sprains or other injuries. Exercise40 Core and joint stabilization.
Caution with activities that can cause overstretching like yoga or gymnastics.
Closed kinetic chain exercises (like biking or elliptical trainer).
Care to avoid overtraining.
Patient Resources Ehlers-Danlos Society (www.ehlers-danlos.com)
Hypermobility Syndromes Association (www.hypermobility.org)
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- One-year effectiveness of high-load compared with low-load strengthening exercise on self-reported function in patients with hypermobile shoulders: a secondary analysis from a randomised controlled trial
- The Most Frequently Read Articles of 2021
- Family Medicine Research on Health Equity, Addiction, and Eating Breakfast--Just for Starters