
Abstract
Although solo and small practices are a vital part of primary care, the proportion of family physicians reporting working in practices with 5 or fewer providers declined from 15% to 11% for solo and 37% to 34% for small (2 to 5 providers) practices from 2014 to 2018. These decreasing trends are concerning, mainly when a low proportion of family physicians have solo practices in rural locations given the access to care challenges in these underserved populations.
- Access to Health Care
- Child Health
- Epidemiologic Studies
- Family Medicine
- Family Physicians
- Primary Health Care
- Private Practice
- Vulnerable Populations
Small and solo practices have been the traditional organizational structure for care delivery in the United States, but widescale consolidation is threatening their viability. Studies have demonstrated that small practice size is associated with fewer preventable patient hospitalizations and better access to care for patients.1 On the other hand, a larger practice size may allow for more leveraging power with payers, more capital for infrastructure improvements, such as electronic health records, and greater access to shared resources such as imaging centers or specialists.2,3 A growing number of recent family medicine graduates prefer to work in large practices for a better work-life balance and to avoid the administrative burdens and other responsibilities associated with owning a practice.3,4 It is unclear if these advantages lead to fewer family physicians (FPs) in small and solo practices.
We used the 2014 to 2018 American Board of Family Medicine (ABFM) Family Medicine Certification Examination Application data on practice size of respondents' primary practice. We calculated the proportion of FPs seeking to continue their certification reporting solo, small (2 to 5 physicians and clinicians), medium (6 to 20), and large practice size (≥20) for the entire 2014 to 2018 sample and stratified by the rural-urban location of their primary practice. We used the Cochrane-Armitage test to determine significant differences in trends in proportions across years in each of the practice size categories.
A total of 35 625 FPs providing direct patient and continuity care (we excluded FPs who reported emergency department/hospital as their primary practice site) were included in the analysis sample. (Figure 1). The number of FPs per year in the sample ranged from 5525 to 8216. We observed a steady decline in the proportions of solo (14% to 11%, P < .01) and small (36% to 32%, P < .01) size practices in urban areas. In rural areas, there was a decrease of 5 percentage-points in FPs reporting solo practices, but the share of FPs in small practices remained nearly the same over time.
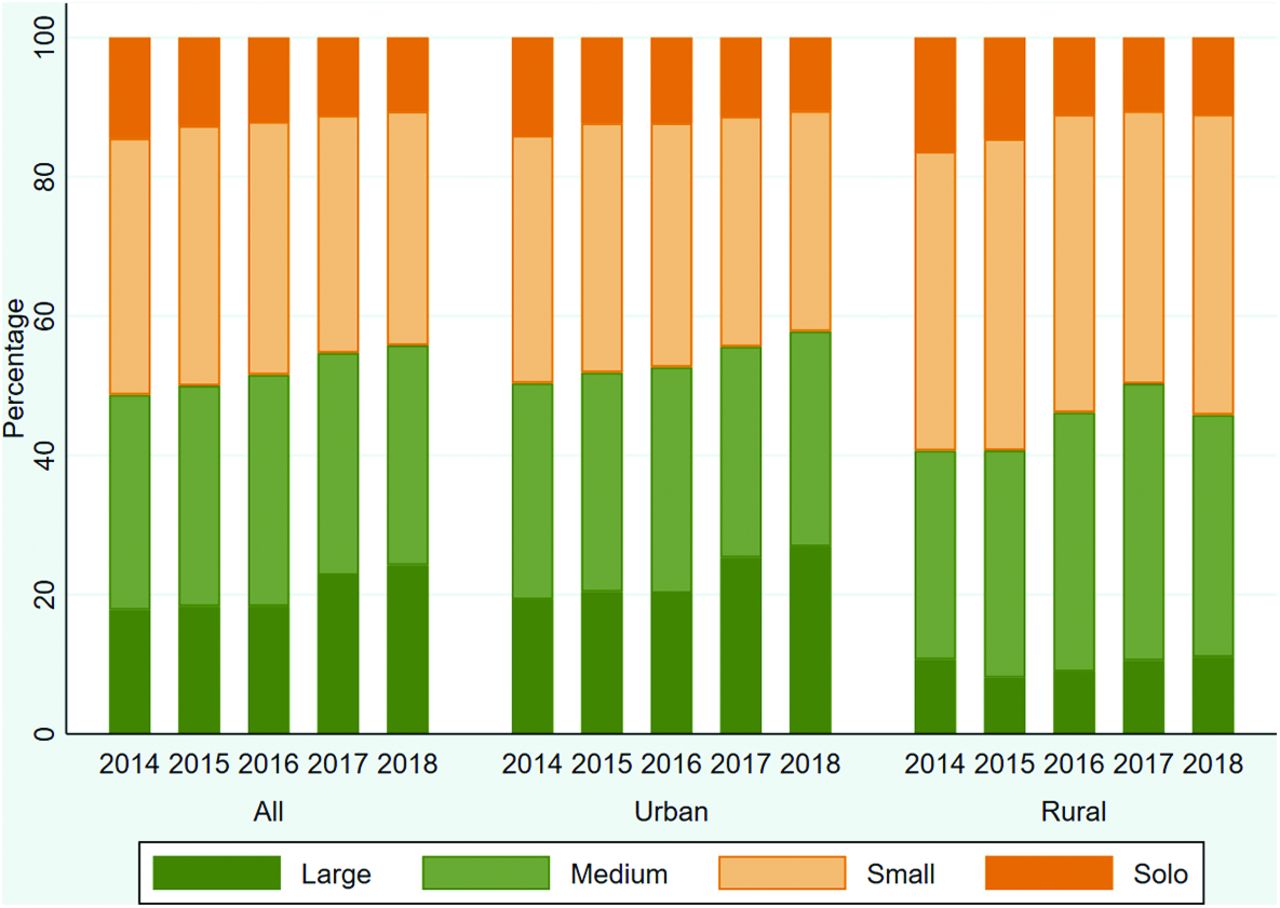
Trends in percentage of family physicians recertifying with The American Board Of Family Medicine who report size of their primary practice (2014 to 2018). Source: American Board of Family Medicine Certification Examination Application Survey (2014 to 2018, N=35 625; 2014, n=8216; 2015, n=8386; 2016, n=7137; 2017, n=6361; 2018, n=5525). Analytical sample restricted to family physicians in direct patient care and providing continuity of care (Large, 20 or more providers; Medium, 6-20 providers; Small, 2-5 providers).
We find that FPs practicing in solo and small practices decreased over time in urban and solo practices in rural areas. These results are consistent with a previous study that demonstrated a 31% relative decrease in FPs in solo practices from 1992 to 2013 (16% to 11%).5 These findings may reflect the ongoing trends in consolidation, which disproportionately affects rural practices that may have fewer resources to sustain market pressure. The current Coronavirus disease-19 (COVID-19) pandemic could exacerbate the decline in solo and small practices further, putting many practices at risk of closure. As this study is based on survey data, there may be reporting bias the practice size may not reflect the true structure of the practice. For instance, family physicians in large practices may have either reported the local clinic unit size as practice size or the large primary practice size.
Whether this trend will have an impact on the quality of care overall is debatable, since previous studies have been mixed on practice size and quality of care.6,7 But understanding the mechanisms behind the loss of small and solo practices, whether it be by consolidation or physician choice, will likely help maintain the diversity of organizational structures in primary care.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: nothing to disclose.
To see this article online, please go to: http://jabfm.org/content/34/2/266.full.
- Received for publication August 31, 2020.
- Revision received October 30, 2020.
- Accepted for publication November 4, 2020.




{kind=link}