
Abstract
The quality of care for children and adults in the United States is variable and often suboptimal. Approaches that improve the systems of care for entire patient populations are needed. The certifying medical boards can contribute to driving change by ensuring that improving care and outcomes for patients and families is the priority. The American Board of Pediatrics has catalyzed collaborative improvement networks, resulting in improved health outcomes for children, fostered partnerships with patients and families, and brought together key stakeholders to advocate for network improvement efforts for sickle cell disease as one action to address health disparities. Similar concerted efforts by certifying boards in collaboration with physicians and patients can improve the quality of care and lead to better patient outcomes.
Introduction
The quality of care for children and adults in the United States is variable and often suboptimal.1,2 Approaches that improve the systems of care for entire patient populations are needed. The certifying medical boards can contribute to driving change by ensuring that improving care and outcomes for patients and families is the priority. Several examples from the American Board of Pediatrics’ (ABP’s) quality journey over the last 2 decades highlight how boards can catalyze improvement efforts and drive results.
The History of Pediatric National Improvement Networks
In 2002, the ABP chartered a workgroup of quality improvement (QI) design experts and representatives from all pediatric subspecialties. This workgroup developed a framework for the “performance in practice” component of the nascent maintenance of certification (MOC) requirements with the explicit goal of improving child health outcomes rather than simply documenting compliance with certification standards.3 At that time, most QI efforts were short-term projects focused on improving care processes (e.g., providing an asthma action plan during clinic visits). Time-bounded, narrowly focused projects are important components of improving quality, but improving outcomes for populations of children required a QI network model. The improvement network model had the following essential elements:
• A specific aim to improve care.
• A national, multicenter, prospective approach to QI.
• Reduction of unnecessary variation by identifying, adopting, and testing best practices.
• Shared, valid, high-quality real-time data.
• Infrastructure support to apply improvement science.
• Public sharing of outcomes to spread best practices.
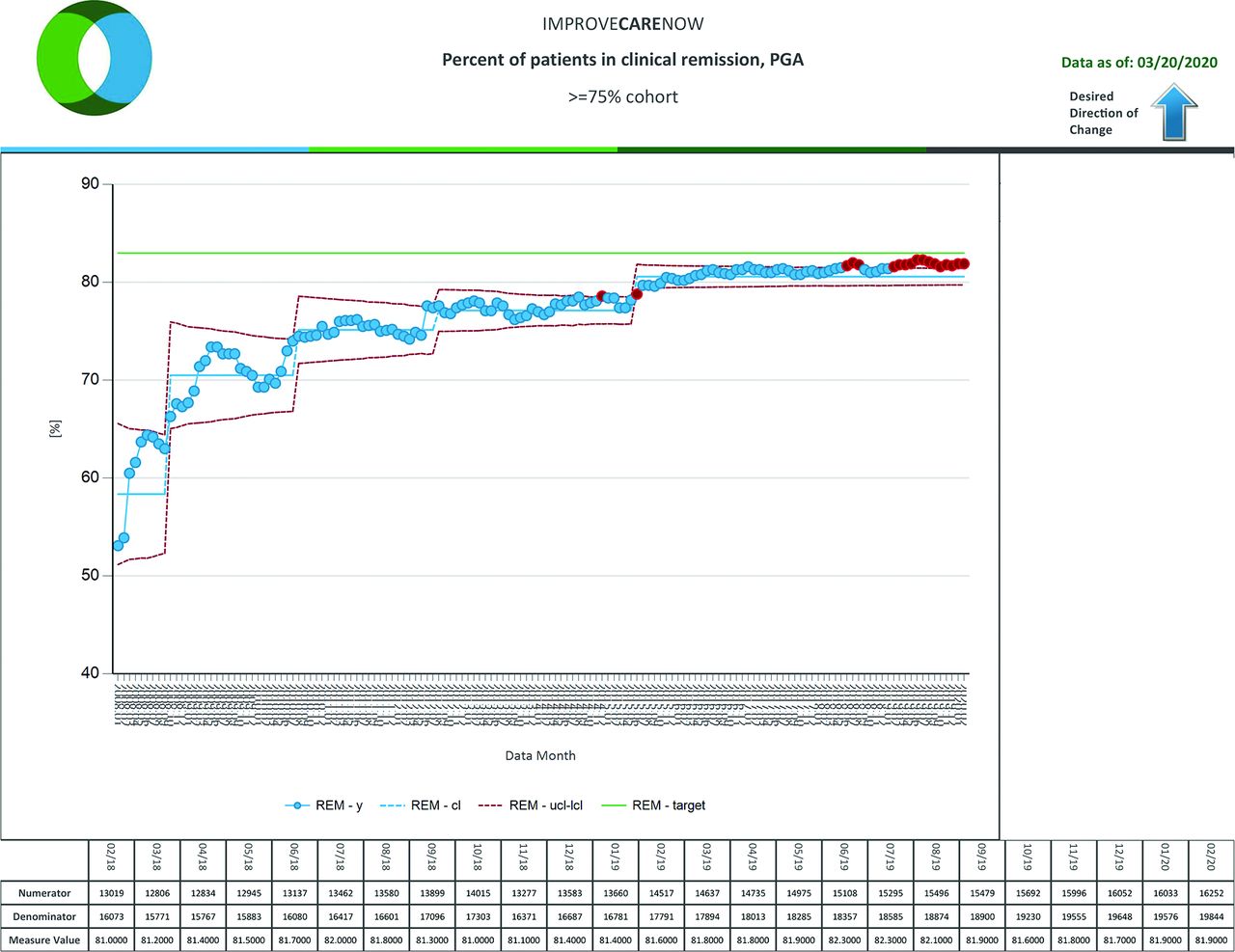
In 2007, the ABP provided seed funding for an improvement network in pediatric gastroenterology, later known as the ImproveCareNow (ICN) network, which focuses on improving care and outcomes in pediatric inflammatory bowel disease.4 The original participating centers standardized diagnostic assessment and treatment algorithms. Now, with more than 109 participating centers, ICN has improved the remission rate of children and adolescents with inflammatory bowel disease from 55% to 82% without the use of new medications (Figure 1).5 In addition to improved health outcomes,6,7 this network has documented multiple successes in care processes,8,9 patient engagement and coproduction,10 and the development of digital tools to improve clinical processes and data collection.11

Illustrates the increase in clinical remission for patients with inflammatory bowel disease (IBD) at ImproveCareNow Network centers between 2007 and 2019. The graph uses data from the ImproveCareNow registry for care centers that have enrolled more than 75% of their IBD patient cohort.
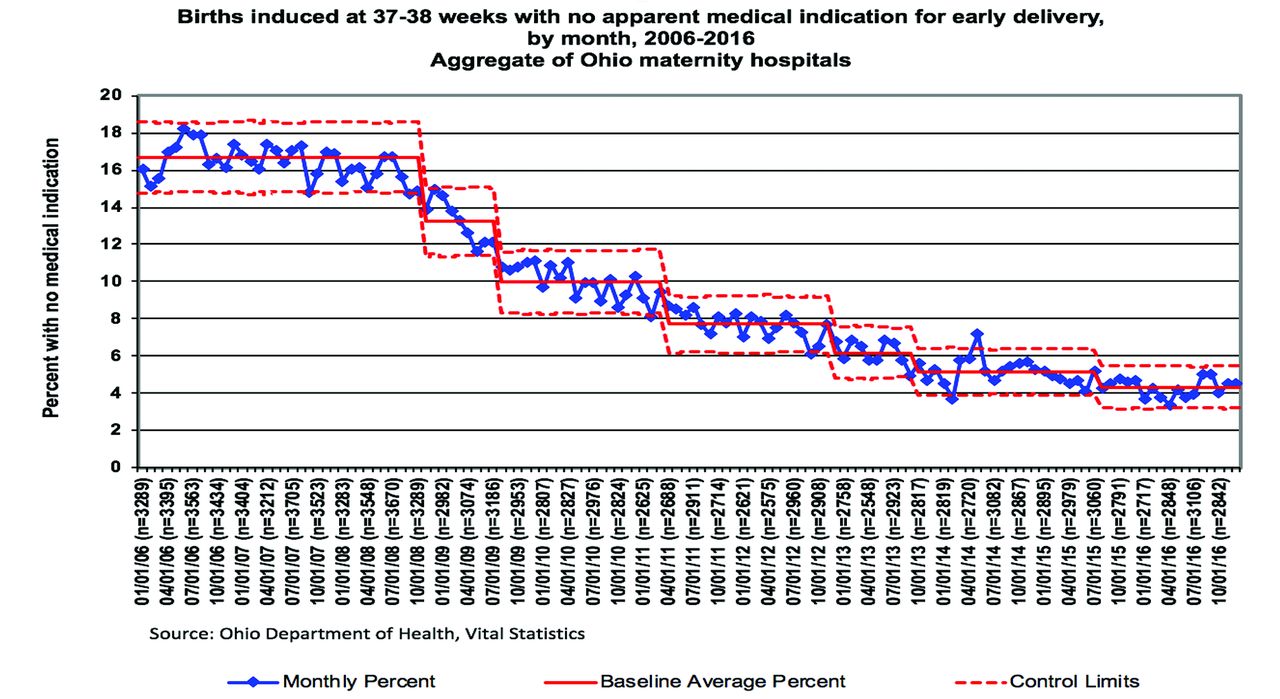
Several other networks have replicated the model successfully,12 including Solutions for Patient Safety (SPS), with 135+ participating children’s hospitals, which since 2012 has protected 12,722 children from serious harm (e.g., hospital-acquired conditions, unplanned extubations, and serious safety events) and has led to an estimated savings of nearly $175 million.13⇓–15 The 65 cardiology centers in the National Pediatric Cardiology Quality Improvement Collaborative (NPCQIC) have collectively decreased mortality by more than 40% among infants with hypoplastic left heart disease.16 The Ohio Perinatal Quality Collaborative (OPQC) has improved perinatal outcomes in several domains: reduced early elective deliveries by 75%17,18 (Figure 2), reduced late onset sepsis in preterm infants,19 reduced length of hospitalization for infants with neonatal abstinence syndrome,20 and reduced births of <32 weeks gestation by 6.6% through a statewide progesterone program.21 OPQC was selected as a mentor network for the development of the Centers for Disease Control and Prevention’s National Network of Perinatal Quality Collaboratives.22 These examples illustrate the success of the network model for many different populations, including inpatient safety, chronic conditions, rare diseases, and newborns.

Illustrates the decline in induced births between 37 and 38 weeks of gestation without medical indication, beginning in 2008 with the initiation of the Ohio Perinatal Quality Collaborative Early Elective Delivery project. The graph uses State of Ohio vital statistics data.
Network Methodology
Network funding comes from various sources. The chronic disease and safety networks are funded by site participation fees, philanthropic support, supplementary grants for research and innovation, and sponsorship of specific activities (e.g., network conferences). The perinatal quality collaboratives are usually supported by government grants.
Improvement networks use QI methods to promote ongoing learning within and across network sites. Networks have adapted the Breakthrough Series model23 by using face-to-face learning sessions, testing during action periods, and regular performance feedback so that quality efforts endure over years.
User-centered design and improvement science principles underpin network development.12,24 Co-production of the improvement program by patients, families, clinicians, and researchers is the critical principle of user-centered design. These stakeholders identify priorities, aims, outcome metrics, and practical approaches to test and implement improvement strategies collaboratively.
Initial network improvement efforts in pediatrics tended to be project focused, time-bounded, and pediatrician centric and emphasized changing clinician behavior. Over time, the networks recognized that improving outcomes for populations of children required addressing the systems of care and engaging all stakeholders (e.g., patients, families, clinicians, and researchers). The resulting culture of collaboration and trust is foundational to an improvement community that uses data to facilitate learning and sharing of best practices. With the inclusion of research into QI networks, the model is now known as the Learning Network model.12 This evolution was consistent with the development of the Institute of Medicine’s Learning Healthcare System model.25
QI and Learning Networks in Primary Care
The ABP has also actively promoted collaborative improvement programs in pediatric primary care. These include the American Academy of Pediatrics (AAP) national collaboratives on various topics, such as immunizations, asthma, developmental screening, and obesity prevention and treatment.26,27 Examples of successful AAP state chapter improvement efforts include the Alabama Child Health Improvement Alliance,28 the Ohio chapter,29,30 and the Vermont Child Health Improvement Program.31 In addition to the AAP, the National Improvement Partnership Network (NIPN) is the other major pediatric primary care network. In over 20 states, NIPN has developed durable state or regional collaborations to advance quality and to improve health care for children.32,33
Patient and Families as Network Partners
An important advance in the network improvement model was recognizing the necessity of an equal partnership with patients and families. Systems of care do not change effectively without engaging all the stakeholders. Thus, the networks changed from having patients and families as advisors to working with them as true partners. Outcomes of importance to patients and families are viewed equitably with those of importance to clinicians and researchers. For example, with parental input, the Autism Learning Health Network has prioritized addressing disruptive behaviors and quality of life for affected children. In the ICN network, young adult patients with ostomies collaborated with clinicians and published “A Guide to Gutsy Living” for teen peers.34 Parental input in NPCQIC made optimizing nutrition a key area of focus so that infants with complex congenital heart disease would be able to eat cake on their first birthday. Parents also asked pediatric cardiologists in NPCQIC to develop simple explanations of important findings from medical publications. These 1-page summaries for lay readers known as “Research Explained”35 live on both the network and parent organization web sites. Any research project using the network’s registry data must have a lay summary.
The ABP Partnership with Patient and Families
At an ABP-sponsored “Partnering with Patients and Families” conference, parents identified a significant gap in emotional health support for children with chronic conditions and their families. In follow-up, the ABP launched the “Roadmap Project” to optimize the resilience and emotional health of children with chronic conditions and their families.36 As part of this initiative, pediatricians, child psychologists, young adult patients, and parents of children with chronic conditions identify practical strategies and develop useful tools to help clinicians build competence in behavioral and mental health care. A pilot improvement collaborative with teams from 9 children’s hospitals launched in January 2020 to test various Roadmap strategies.
At another ABP Patient and Family conference, a mother of twins with sickle cell disease (SCD) asked the ABP CEO, “why isn’t there a Learning Network for SCD?” Data indicate that disparities in the care and outcomes of Black children with SCD include suboptimal antibiotic prophylaxis, pneumococcal vaccination, hydroxyurea use, transcranial doppler imaging, and transition of care planning from adolescence to adulthood.37,38 In response, the ABP has partnered with the American Society of Hematology, federal agencies, and SCD patient advocacy groups, to consider the development of an SCD Learning Network.
Developing a Learning Network for SCD is one effort to improve outcomes for a vulnerable and often underserved population. This can be part of an aggressive strategy to eliminate racial and ethnic disparities in health care.39⇓⇓–42
The Role of the Certifying Board in Catalyzing Improvement Networks
The ABP has used multiple strategies to achieve its “North Star” of improving of health outcomes for children, adolescents, and young adults. From the beginning, ABP leadership has championed the network model’s promise to improve health outcomes for children. In addition, a pediatrician expert in the design and implementation of QI networks (CL) has served as Senior Quality Advisor to the ABP.
Stakeholder convening and engagement has been another strategy. The ABP hosted meetings of subspecialty leaders and relevant professional organizations to share the network potential and early successes. These meetings spawned the networks for pediatric cardiology, rheumatology, and patient safety. The ABP subboard chairs worked with their professional organizations to publicize opportunities for network participation. Local engagement rose by making it possible for every pediatrician in the networks to earn MOC points.
Dissemination of the impact of Learning Networks has been a third strategy. A 2013, ABP meeting of patients, parents, clinicians, governmental leaders, payers, and professional organizations led to a supplement in the journal Pediatrics, namely, “Pediatric Collaborative Improvement Networks.”3 The ABP Annual Report, mailed to all ABP diplomates, highlighted collaborative improvement efforts in primary and subspecialty care.43 In addition, the ABP gives the Paul V. Miles Fellowship award annually to a pediatrician who has demonstrated excellence in improving the quality of care for children.44
The ABP process for providing Part 4 MOC credit for participation in collaborative improvement efforts is designed to foster clinician engagement. Network leaders submit the applications for improvement activities directly to the ABP or an approved Portfolio Sponsor organization. Many of the AAP state chapters and regional improvement partnerships serve as Portfolio Sponsor organizations. As part of the application, collaborative leaders define the level of participation required for a physician to be eligible to receive MOC Part 4 credit. In general, meaningful participation is defined as (1) implementing the project’s interventions, (2) reviewing the project’s measurement data, and (3) attending in-person or virtual team meetings. Verification of a physician’s participation occurs at the local level, and the project leaders award the Part 4 points on behalf of the ABP. The aim is for the ABP to support local QI and ensure physicians get credit for the meaningful improvement work they are doing within the context of their practice.
Conclusions
In summary, the ABP has catalyzed collaborative improvement networks, resulting in improved health outcomes for children; fostered partnerships with patients and families; and brought together key stakeholders to advocate for network improvement efforts for sickle cell disease as one action to address health disparities. Similar concerted efforts by certifying boards in collaboration with physicians and patients can improve the quality of care and lead to better patient outcomes.
Notes
This article was externally peer reviewed.
Funding: Dr. Lannon serves in a consulting role to the American Board of Pediatrics as Senior Quality Advisor.
Conflict of interest: Dr. Lannon is an inventor of technology to support Learning Health System Networks that has been licensed to Hive Networks by Cincinnati Children’s.
- Received for publication March 24, 2020.
- Revision received June 18, 2020.
- Accepted for publication June 22, 2020.
References
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- The History of Pediatric National Improvement Networks
- Network Methodology
- QI and Learning Networks in Primary Care
- Patient and Families as Network Partners
- The ABP Partnership with Patient and Families
- The Role of the Certifying Board in Catalyzing Improvement Networks
- Conclusions
- Notes
- References
- Figures & Data
- References
- Info & Metrics