
Article Figures & Data
Figures
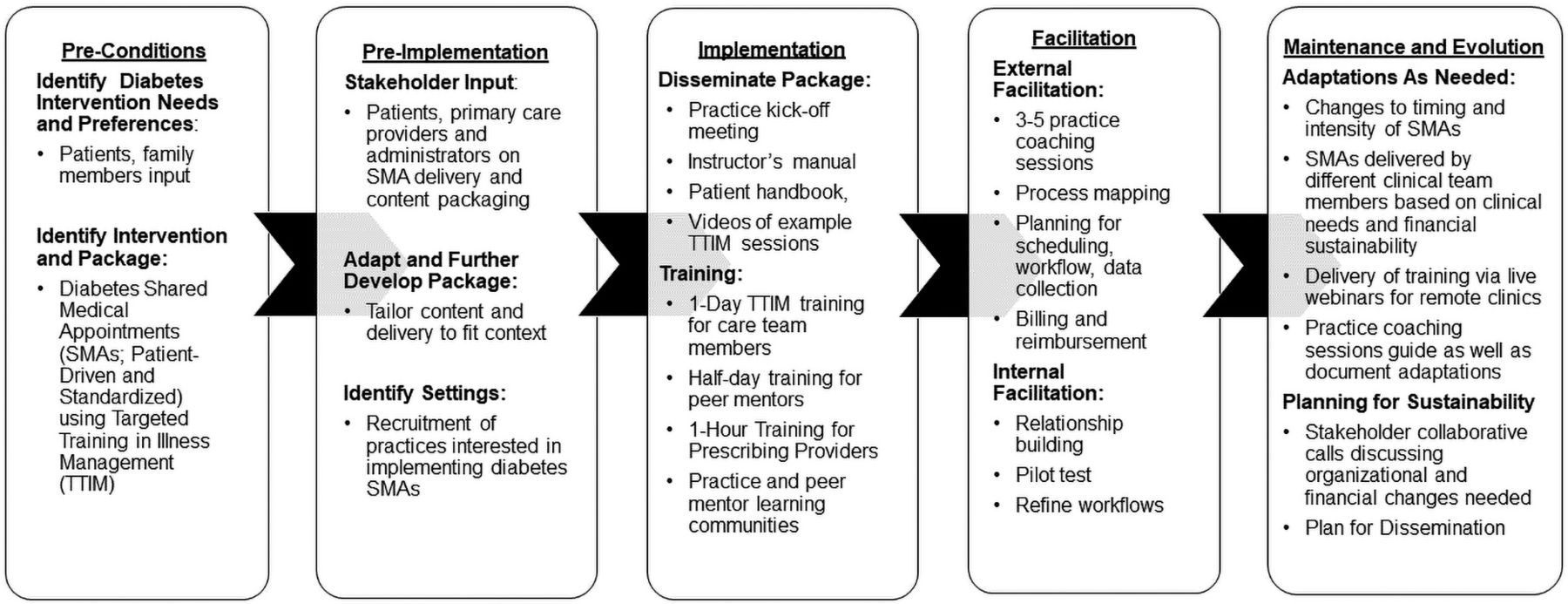
- Figure 1.
The enhanced Replicating Effective Programs framework for Invested in Diabetes Study planning and adaptations. Abbreviation: SMAs, shared medical appointments.
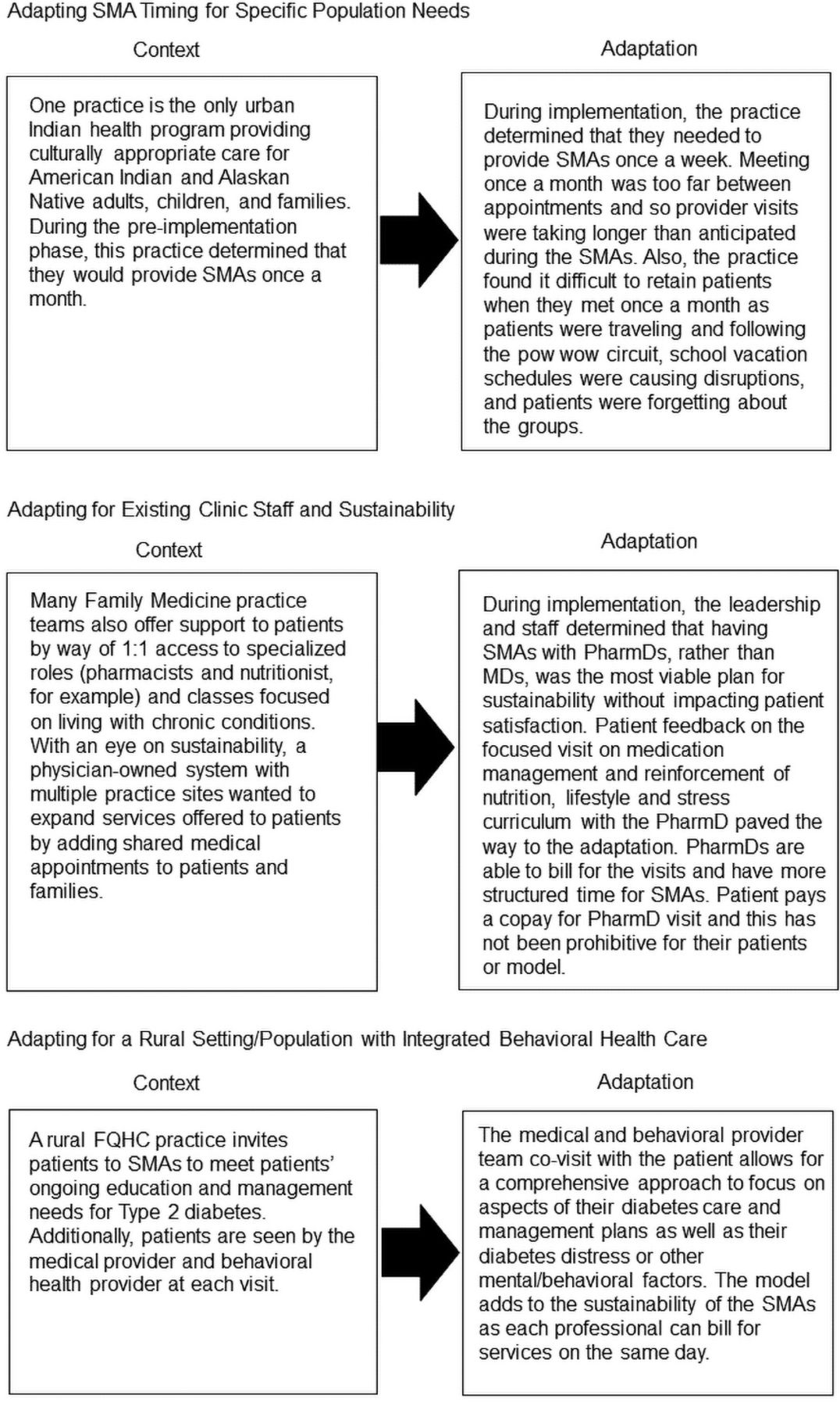
- Figure 2.
Case vignettes of adaptations to fit practice characteristics. Abbreviations: SMA, shared medical appointments; FQHCs, federally qualified health centers.


Tables
Contextual Characteristics Overall (n = 22) Patient-Driven Condition (n = 11) Standardized Condition (n = 11) Difference across Conditions* Practice type, N (%) federally qualified health centers 12 (54) 5 (45) 5 (45) P = 1.00 Practice location, N (%) P = 1.00 Urban 17 (77) 9 (82) 8 (73) Rural 3 (14) 1 (9) 2 (18) Suburban 2 (9) 1 (9) 1 (9) Estimated no. of diabetes patients, median (range) 549 (90–4000) 500 (90–4000) 576 (214–2112) P = .48 Latino patients > 10%, N (%) of practices 10 (67) 5 (63) 5 (71) P = 1.00 Minority patients > 20%, N (%) of practices 13 (87) 5 (71) 8 (100) P = .20 Payer mix, median (range) Private insurance FFS or preferred provider organization 11 (3–70) 12 (3–64) 10 (5–70) Private managed care 11 (5–35) 15 (10–20) 10 (5–35) Medicare 19 (2–60) 20 (9–30) 14 (2–60) Medicaid 40 (2–63) 30 (5–60) 55 (2–63) Other public insurance 3 (0–5) 3 (0–5) 3 (0–5) Self-pay or uninsured 10 (0–92) 6 (0–92) 10 (3–36) Unknown 0 (0–10) 0 (0–10) 0 (0–5) Other 4 (0–100) 0 (0-0) 9 (0–100) Private (FFS + managed care) > (Medicare + Medicaid + other pub) 3 (19%) 2 (29%) 1 (11%) P = .55 No. of clinicians with prescribing privileges, median (range) 8 (2–65) 7 (2–39) 8 (3–65) P = .39 No. of staff eligible to be health educator, median (range) 2 (1–6) 2 (1–6) 3 (1–6) P = .79 No. of behavioral health providers by level of training (interviewees) Doctorate level: 3; Master's level: 10; other: 4; unknown: 2 Doctorate level: 2; Master's level: 5; other: 3; unknown: 1 Doctorate level: 1; Master's level: 5; other: 1; unknown: 1 Previous experience with SMAs, N (%) 10 (45) 5 (45) 5 (45) P = 1.00 PCMH PM†, median (range) PM data capacity 79 (39–100) 89 (50–100) 77 (39–96) P = .26 PM team-based care 75 (35–100) 80 (50–100) 75 (35–95) P = .27 PM quality improvement processes 82 (7–100) 82 (50–100) 82 (7–100) P = 1.00 PM population management 70 (0–100) 70 (50–100) 73 (0–90) P = .62 - Table 2.
Baseline Practice Culture Assessment Scores among All Clinicians and Staff in Participating Practices
PCA Category PCA Scores* Difference between Conditions† Overall Patient-Driven Practices Standardized Practices Work culture, mean ± SD 70.4 ± 14.6 (n = 432) 70.2 ± 15.1 70.8 ± 13.9 P = .66 Change culture, mean ± SD 71.5 ± 15.5 (n = 433) 72.0 ± 14.5 70.8 ± 16.8 P = .44 Chaos, mean ± SD 35.1 ± 16.9 (n = 432) 34.6 ± 16.0 35.8 ± 18.1 P = .46 - Table 3.
High-Level Intervention Adaptations to Targeted Training in Illness Management Intervention Content and Context for Delivery in Primary Care
Intervention Content Personnel Format Setting and Population Original TTIM Twelve 1-hour sessions with content focused on skills building and self-management of diabetes and SMI Delivered by study nurses and peer educators Group-format with standardized topic order Research setting for patients with diabetes and SMI Adapted TTIM Six 2-hour sessions with content focused on skills building, stress and coping, and self-management of diabetes, with optional SMI content Delivered by practice staff: health educators, behavioral health providers, and peer mentors (differs by condition) Group-format with standardized topic order or topic order selected by patients; 1:1 visits with prescribing provider for medication management Primary care setting for patients with diabetes (± co-occurring mental health conditions) SMI, serious mental illness; TTIM, Targeted Training in Illness Management.
- Table 4.
Intervention Content and Delivery Adaptations across the Replicating Effective Programs Phases
Intervention Content and Delivery Adaptations Replicating Effective Programs Phases Preconditions Phase Selection of intervention content Stakeholder input prioritizes mental and physical health content Selected TTIM curriculum based on inclusion of diabetes self-management and mental health focus Specification of core elements for delivery of SMAs Stakeholder input prioritizes patients selecting topics, peer mentors, and involvement of behavioral health professionals Selected TTIM based on inclusion of peer educators Pre-implementation Phase Content adaptations: reordering elements and adjusting timing Repackaged and reordered content into 6 2-hour modules (vs original 12, 1-hour modules) Divided content and training material for standardized versus patient-driven SMA conditions. Adjusted timing to fit experience of interventionists In patient-driven condition, provided instructions for reordering content to fit cohort-specific preferences In standardized condition, manual provides instructions on duration of each topic; patient-driven manual provides suggested time only Content adaptations: removing elements Removed ongoing TTIM illness management phase Changed TTIM manual language to focus more on a primary care population rather than SMI population Less focus on serious mental illness, with now-optional mental health elements Content adaptations: adding and substituting elements General stress and coping module substituted for primary care population in lieu of Diabetes and Serious Mental Illness module PROs and instructions for addressing PROs as part of tailoring content to patients added Translation of TTIM instructor's manual and patient handbook to Spanish Emphasized medical management of diabetes Updated stress management tips with infographic from the American Heart Association “Fight Stress with Healthy Habits” Added 1:1 visits with prescribing provider for medical management In patient-driven condition, behavioral health provider and peer mentor instructions added Up-to-date diabetes management, nutrition, and physical activity content substituted Delivery adaptations: personnel Delivered by practice staff: health educators, behavioral health providers, peer mentors (differs by condition) Added PharmD as eligible for prescribing provider Implementation Phase Content adaptations: packaging and visual appeal Use of icons and text formatting to guide reader through use of the instructor's manual Professional graphic design for visuals for patient handbook and PowerPoint slides Developed two versions of instructor manual based on study condition (standardized vs patient-driven SMA) Practice facilitation adaptations Expanded beyond initial 5 planned sessions to meet practices' needs for additional support Developed system to prioritized practice facilitation outreach based on practice implementation progress Training adaptations Offered remote and multiday trainings in addition to full-day in person trainings Incorporated role play into trainings Group facilitation instructions added PRO, patient-reported outcomes; SMA, shared medical appointments; TTIM, targeted training in illness management; SMI, serious mental illness.
Contextual Factors Invested in Diabetes Practice Characteristics Corresponding Adaptations Data capabilities and population management All practices had electronic health records
Some had registries to help identify eligible patients
Varied experience with PRO collection and useSimplified eligibility criteria for patients (any adult with Type II diabetes, no exclusion criteria) for ease of identification
Ensured PROs were relevant to clinical care and SMA discussionsPayer mix Practices vary in payer mix, with different billing and reimbursement practices Informed guidelines for frequency of prescribing provider visits (at every session/1st/last only etc)
Provided documentation templates and common billing codes used for diabetes SMAsPrior experience with SMAs Some practices had prior experience delivering and billing for diabetes SMAs Informed intensity of technical assistance, plans for process mapping; practice coaches spent more time with helping practices determine SMA workflows and staffing Team-based care Practice all had behavioral health
Some were fully integrated with behavioral health providers and experienced with integrated team-based care; others had collocated care where the behavioral health provider operated independently of the primary care providerInfluenced plans to include behavioral health providers in trainings alongside health educators (in patient-driven condition) and adaptations to mental health and stress and coping content Patient populations Practices delivering care to >10% Hispanic/Latino patients opted to provide SMAs in Spanish
Patients vary in prior diabetes education, resources, and literacySpanish language TTIM materials and Spanish-speaking peer mentors and health educators made available
Optional TTIM content with basic vs more advanced information and skills, with instructions to practices for selecting content most appropriate for their patients (e.g., basic carb counting vs glycemic index content)Practice culture Practices had moderate-to-high chaos and moderate-to-strong change culture; high chaos practices more sensitive to burden and resources Influenced decisions about how to reduce burden to practices and how much technical assistance was required from the coach Practice location and size Practices vary in size, urban, suburban, and rural
Native American population that travels ≥50 miles for primary care servicesInformed flexibility/adaptations around frequency/duration of sessions, expected size of cohorts, and number of sessions Practice clinician and staff availability Practices vary in number and type of clinicians and staff available to deliver SMAs Influenced adaptations to health educator and prescribing provider eligibility criteria, frequency of prescribing provider visits PRO, patient-reported outcomes; SMA, shared medical appointments; TTIM, targeted training in illness management.




{kind=link}
{kind=link}