
Article Figures & Data
Figures
- Figure 1.
Workflow of practice facilitation in the Healthy Hearts in the Heartland (H3) initiative. Abbreviations: PF, practice facilitator; QB, QuickBase; NU, Northwestern University; ABCS, aspirin use, blood pressure, cholesterol, and smoking.
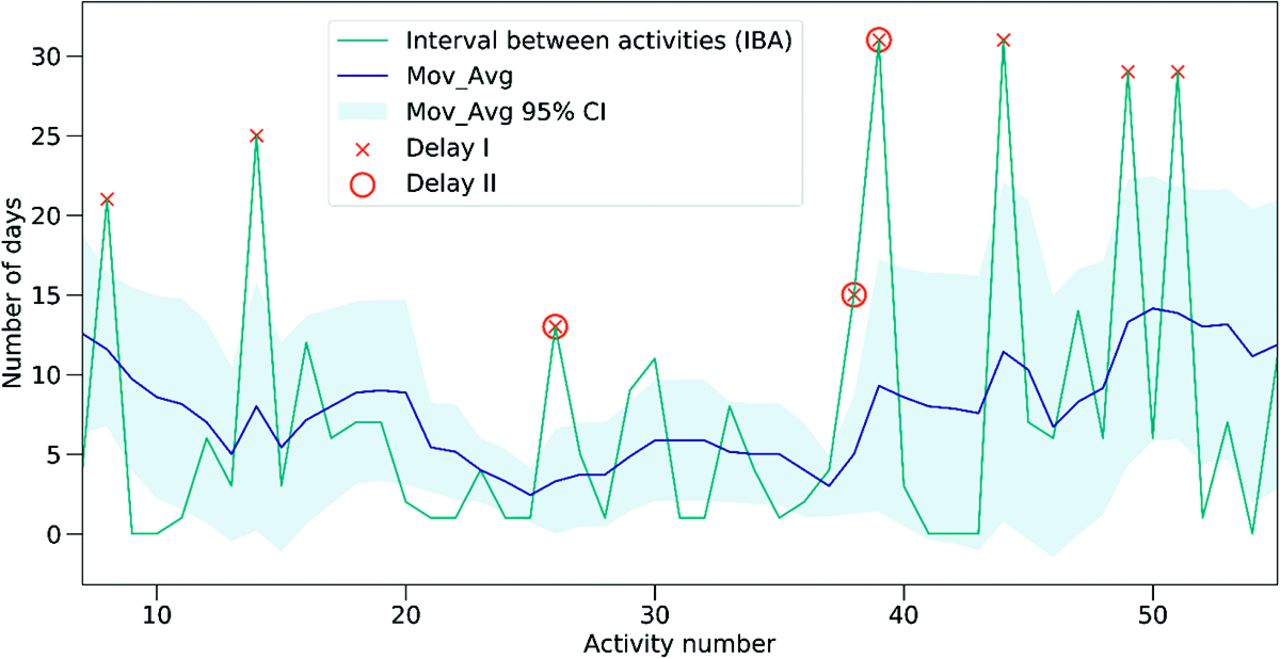
- Figure 2.
Example practice (#117) activities and delays. This Figure illustrates the mechanism by which the 2 types of delays are identified. If the interval between activities (IBA) is higher than the Z-score (described in Methods, Step 2), a delay will be detected. X-axis is the sequence number of each activity; Y-axis is the number of days between activities; Mov_Avg is the moving average results of IBA; Mov_Avg 95% CI is the 95% confidence interval of the Mov_Avg results.



Tables
- Table 1.
Characteristics of 226 Practices in Illinois, Wisconsin, and Indiana Participating in the Healthy Hearts in the Heartland (H3) Initiative across 4 Waves in 2016
Characteristics N (%) Number of practices by wave Wave 1 42 (18.6) Wave 2 40 (17.7) Wave 3 67 (29.6) Wave 4 77 (34.1) Clinicians, n Solo practice 67 (29.6) 2−5 103 (45.6) 6−10 34 (15.0) 11−15 10 (4.40) 16−20 12 (5.30) State Illinois 152 (67.3) Wisconsin 22 (9.7) Indiana 52 (23.0) The 4 waves were the randomization conditions of the study. The waves determined when a practice started receiving the 12-month intervention. Practices in Wave 1 started from the first quarter of 2016; wave 2 started from the second quarter of 2016, and so on. The four waves were reported separately because the starting and end dates were different.
Wave 1 Wave 2 Wave 3 Wave 4 Total Total number of Delay I* 84 44 142 131 401 Total number of Delay II† 45 25 84 63 217 Median No. of Delay I per practice (IQR) 2 (1 to 3) 1 (0 to 2) 2 (1 to 3) 2 (1 to 2) 2 (1 to 3) Median No. of Delay II per practice (IQR) 1 (0 to 2) 0 (0 to 1) 1 (0 to 2) 1 (0 to 1) 1(0 to 1) IQR, interquartile range.
The 4 waves were reported separately because the starting and end dates were different.
↵* Delay I was calculated based on Z score > 1.282, which corresponds to a one-tailed 90% confidence interval. Delay I is identified if the interval between activities (IBA) deviates from the practice's normal pattern of facilitation activities.
↵† Delay II was calculated based on Z-score > 1.645, which corresponds to a one-tailed 95% confidence interval. Delay II captures a larger deviation from the normal pattern compared to Delay I. Delay I is more sensitive to detecting delays than Delay II and could capture more instances of infrequent facilitation activities.
- Table 3.
Barriers to Practice Facilitation and Quality Improvement Intervention (Source: Practice Facilitators' Notes)
Domain Barriers N (%) Practice-related barriers Lack of time and staff 378 (44.37) EHR-related issues 136 (15.96) Lack of buy-in/engagement 133 (15.61) Other* 59 (6.92) Staff turnover 51 (5.99) Workflow issues 29 (3.40) Implementation-related barriers Technical issues 37 (4.34) Lack of guidelines 12 (1.41) Lack of reimbursement 8 (0.94) Lack of language diversity of intervention materials 9 (1.06) ↵* Examples include low resources, lack of investment, clinic construction, patient issues, and logistic issues.
EHR, electronic health record.
Variable Delay I Delay II Beta (95% CI) Beta (95% CI) Practice-related barriers Lack of time & staff 0.16 (0.08, 0.24)* 0.08 (0.02, 0.14)* EHR-related issues 0.29 (0.14, 0.44)* 0.13 (0.02, 0.24)† Lack of buy-in/engagement 0.19 (0.01, 0.36)† 0.15 (0.02, 0.27)† Staff turnover 0.48 (0.15, 0.82)* 0.31 (0.06, 0.55)† Workflow issues 0.06 (−0.37, 0.48) 0.20 (−0.10, 0.51) Other 0.26 (−0.04, 0.56) 0.15 (−0.07, 0.36) Implementation-related barriers Technical issues 0.18 (−0.23, 0.60) 0.04 (−0.36, 0.34) Lack of guidelines 0.55 (−0.25, 1.34) 0.10 (−0.48, 0.67) Lack of reimbursement 0.59 (−0.46, 1.64) 0.54 (−0.21, 1.29) Lack of language diversity of intervention materials 0.61 (−0.20, 1.43) 0.25 (−0.34, 0.84) Intervention ID Category Measure Component 1 A. Point-of-Care Clinical Decision Support Aspirin Reminder to order aspirin/antiplatelet drug for pts with IV.D (or CVD) 2 A. Point-of-Care Clinical Decision Support BP Alert staff to a patient with uncontrolled blood pressure 3 A. Point-of-Care Clinical Decision Support Cholesterol Alert for a lipid panel (or cholesterol) in ASCVD (or IV.D, or CVD) 4 A. Point-of-Care Clinical Decision Support Cholesterol Alert for a lipid panel (or cholesterol) in diabetes mellitus 5 A. Point-of-Care Clinical Decision Support Cholesterol Alert for a lipid panel in general population (low risk patients) 6 A. Point-of-Care Clinical Decision Support Cholesterol Reminder to order a statin in ASCVD (or IV.D, or CVD) 7 A. Point-of-Care Clinical Decision Support Cholesterol Reminder to order statin in diabetic patients 8 A. Point-of-Care Clinical Decision Support Cholesterol Alert to order a statin in pts with LDL 190 9 A. Point-of-Care Clinical Decision Support Cholesterol Alert to order statin in general population with increased risk (based on a risk calculator) 10 A. Point-of-Care Clinical Decision Support Aspirin Reminder to order aspirin for primary prevention in appropriate patients 11 A. Point-of-Care Clinical Decision Support Smoking Reminder for intervention in tobacco users or smokers 12 B. Other Clinical Decision Support Activities BP Orders/patient instructions/patient education for home BP monitoring 13 B. Other Clinical Decision Support Activities Cholesterol Patient education on cholesterol and/or cholesterol treatment 14 B. Other Clinical Decision Support Activities Cholesterol Standing orders for lipid profiles 15 B. Other Clinical Decision Support Activities Smoking Patient education on tobacco cessation 16 C. Practice Workflows BP Blood pressure measurement protocol 17 C. Practice Workflows BP Blood pressure treatment protocol 18 C. Practice Workflows BP Workflow for patient to report home blood pressures 19 C. Practice Workflows Smoking Tobacco use/smoking assessment part of intake or rooming process 20 C. Practice Workflows Smoking Clinic based tobacco use/smoking interventions 21 D. Reports on ABCS Performance Aspirin Metric for use of aspirin or another antithrombotic therapy in IV.D 22 D. Reports on ABCS Performance BP Metric for blood pressure control among patients with hypertension 23 D. Reports on ABCS Performance Cholesterol Metric for cholesterol treatment or control 24 D. Reports on ABCS Performance Smoking Metric for tobacco use assessment and brief intervention 25 E. Lists of Patients Not Meeting ABCS Measures Aspirin List of patients with IV.D not meeting aspirin/antithrombotic measure 26 E. Lists of Patients Not Meeting ABCS Measures BP List of patients with uncontrolled blood pressure 27 E. Lists of Patients Not Meeting ABCS Measures Cholesterol List of patients needing cholesterol measurement and/or treatment 28 E. Lists of Patients Not Meeting ABCS Measures Smoking List of tobacco users/smokers 29 F. Population Management Outreach Aspirin Outreach to patients with IV.D not on aspirin or another antithrombotic 30 F. Population Management Outreach BP Outreach to patients with uncontrolled hypertension 31 F. Population Management Outreach Cholesterol Outreach to patients who need cholesterol measurement or statin prescription 32 F. Population Management Outreach Smoking Outreach to tobacco users or smokers 33 F. Population Management Outreach Cholesterol Outreach to patients with increased CVD risk who are not on a statin for primary prevention 34 G. Population Management Community Resources BP Referral to community pharmacist for hypertension medication management 35 G. Population Management Community Resources Other Referral to HealtheRx resource BP, blood pressure; LDL, low-density lipoprotein; CVD, cardiovascular disease; ASCVD, atherosclerotic cardiovascular disease; IVD, Ischemic vascular disease.
Id Code Sub-Codes 1–Practice-related barriers 1-1 Lack of time/staff Scheduling issues Providers/Staff were busy/on vacation/personal issues (e.g., family emergency)
Competing demands/priorities Limited time for QI activities Lack of staff/staff burnout
1-2 Lack of buy-in/engagement Providers negative attitudes/belief
Lack of engagement/leader support/interest1-3 EHR-related issues EHR update/change
Outdated EHR/data infrastructure
Facilitators had no access to EHR1-4 Other Low resources
Lack of investment
Patient issue
Clinic construction
Logistic issues1-5 Staff turnover Staff turnover 1-6 Workflow issues Clinical workflow
Teamwork/Collaboration issues
Communication inefficiency2–Implementation-related barriers 2-1 Technical issues Delays in data extraction/access
Lack of proper document, such as BAA2-2 Lack of guidelines Lack of guidance on EHR documentation
Insufficient guidelines on data extraction2 to 3 Lack of reimbursement Lack of reimbursement 2 to 4 Lack of language diversity of intervention materials Most intervention materials are in English EHR, electronic health record; BAA, business associate agreement.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- What AHRQ Learned While Working to Transform Primary Care
- The Effects of Major Disruptions on Practice Participation in Facilitation During a Primary Care Quality Improvement Initiative
- The Most Frequently Read Articles of 2020
- Improving the management of type 2 diabetes through large-scale general practice: the role of a data-driven and technology-enabled education programme
- The Changing Face of Primary Care Research and Practice-Based Research Networks (PBRNs) in Light of the COVID-19 Pandemic