
Article Figures & Data
Figures
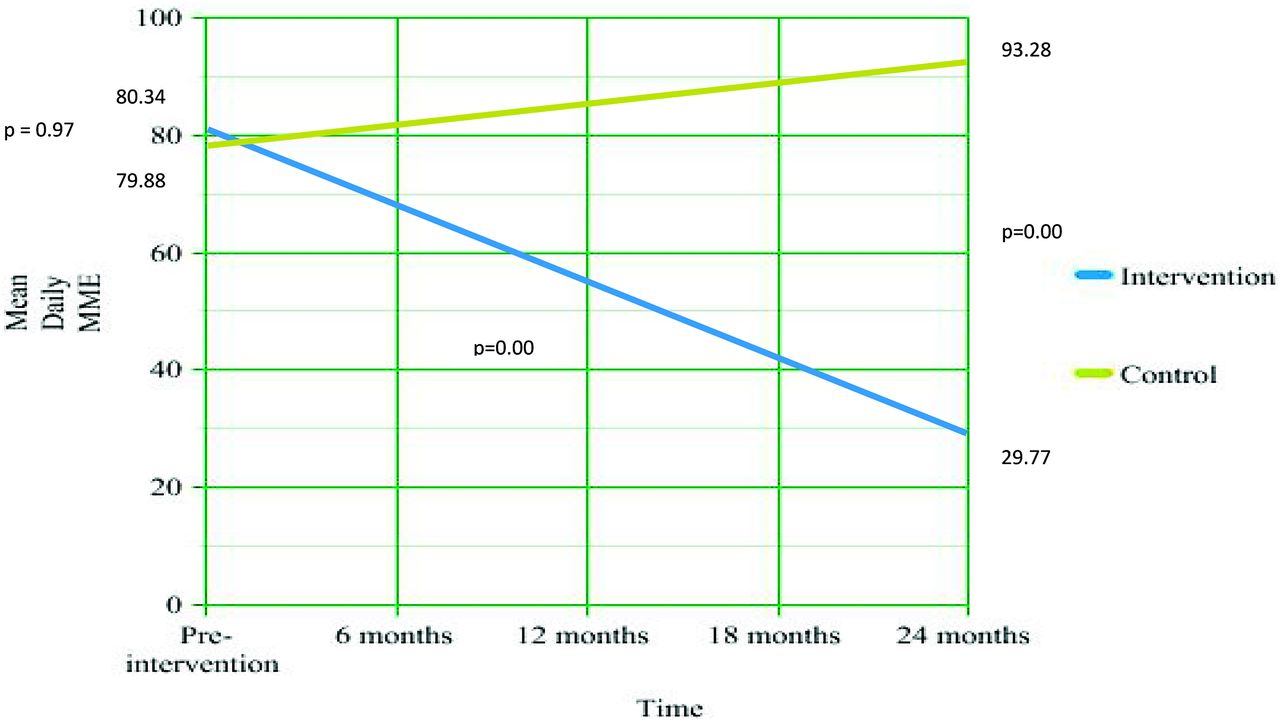
- Figure 1.
Change in opioid mean daily Morphine Milligram Equivalents (MME) among rural chronic non-cancer pain patients over time (n = 186).
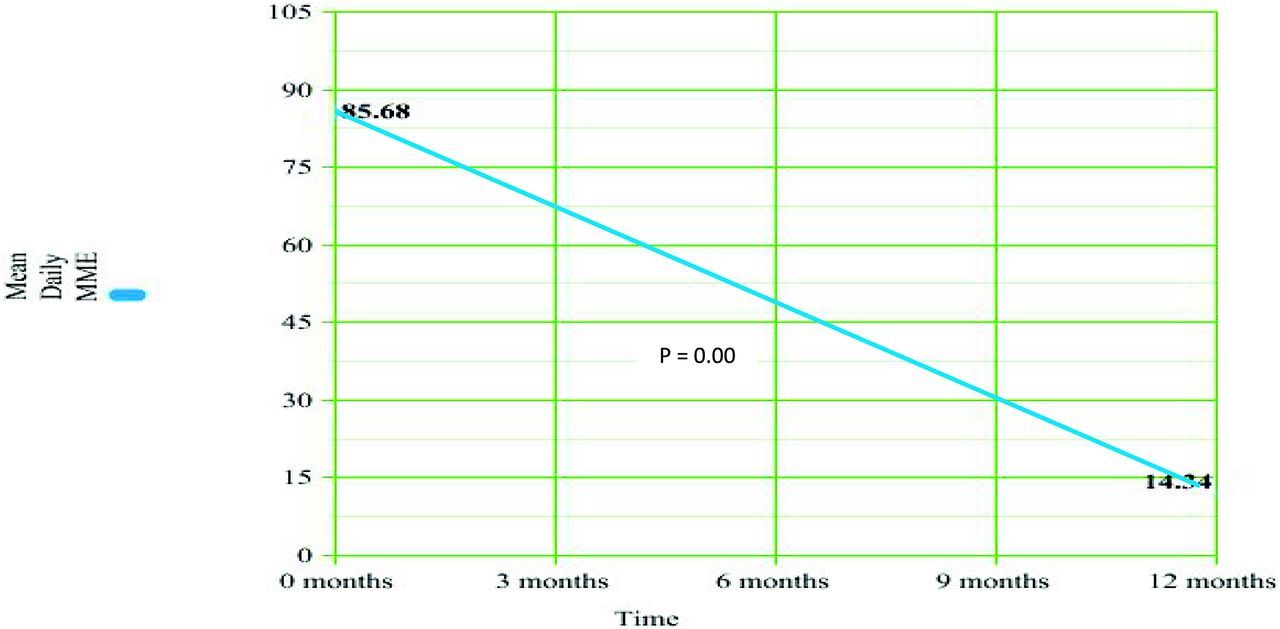
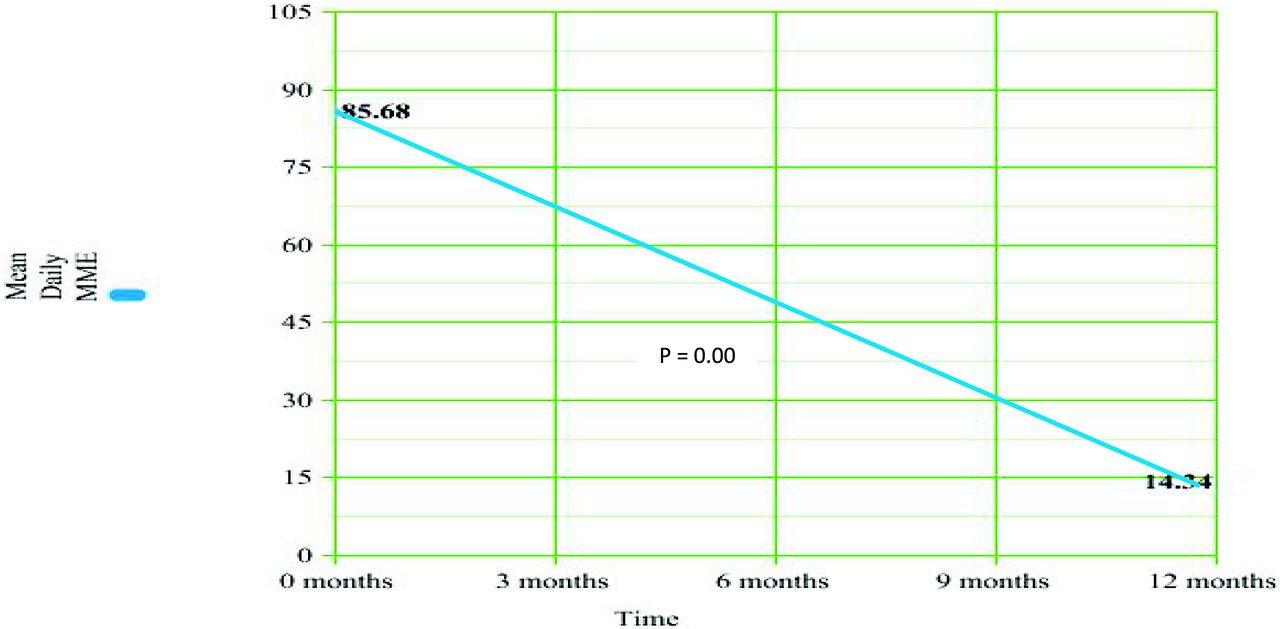
- Figure 2.
Change in opioid mean daily Morphine Milligram Equivalents (MME) in rural chronic non-cancer pain patients during 1 year cross over phase (n = 93).
Tables
- Table 1.
Components of the Comprehensive Opioid Reduction Protocol for Rural Chronic Non-Cancer Pain Patients: Original Intervention and the Crossover Arm (n = 186)
Opioid Reduction Protocol During Original Intervention Opioid Reduction Protocol During Crossover Phase Risk assessment including: high dose opioids (>90 MME); medical co-morbidities (sleep apnea, COPD, etc.); Psychiatric comorbidities and concurrent use of benzodiazepines or carisoprodol. Same Intervene in high-risk cases: Naloxone co-prescribing if patient is over 50 MME: rapidly taper of carisoprodol; Immediately begin opioid or benzodiazepine taper for patients on both. (benzo cannot be stopped or tapered rapidly due to risk of seizures); assessing for OUD and referring for MAT. Same Patient education provided via an 8-week psycho-educational support group, handouts, and provider counseling during individual appointments. Patient education provided via handouts and provider counseling during individual appointments: no educational support group “Universal Precautions”: All patients received opioid agreement; random urine drug screens (UDS) and monthly checks of online, state-wide prescription drug monitoring program. Same Treatment of psychiatric comorbidities (depression; anxiety; insomnia; PTSD; nicotine dependence). Same Maximizing non-pharmacological pain treatments (physical therapy; osteopathic manual medicine; massage; acupuncture; transcutaneous electrical nerve stimulation (TENS); joint and trigger point injections. Same Maximized non-opioid pharmacologic treatments where possible (NSAID; SNRI; TCA; Gabapentinoids; topical analgesics). Same Goal to taper all patients under 90 MME and most under 50 MME. Not expected to stop opioids completely. Goal to taper all patient to the lower threshold of 30 MME or to stop opioids entirely High-risk patients who refused to taper were referred to pain specialty for consideration of MAT Automatic referral to pain specialty for patient who: were on 90 MME or more; were on opioids and benzodiazepine; who had significant medical comorbidities (sleep apnea; COPD) Completed over 2 years Completed over 1 year COPD, Chronic obstructive pulmonary disease; MME, Morphine Milligram Equivalents; OUD, Opioid Use Disorder; MAT, Medication-Assisted Therapy; PTSD, Post-traumatic Stress Disorder; NSAID, Nonsteroidal Anti-Inflammatory Drugs; SNRI, Serotonin-norepinephrine Reuptake Inhibitors; TCA, Tricyclic Antidepressants.
- Table 2.
Description of Psycho-Educational Group for Rural Chronic Non-Cancer Pain Patients
Description of Psycho-Educational Group Development Developed by clinic providers in consultation with pain psychologist Time frame One 90-minute session per week for 8 weeks Staffing family physician assistant and registered nurse Group size 6–12 patients Format Welcome; patient self report on application of last week's topic; didactic presentation; gentle stretching, relaxation techniques and mindfulness practice; questions and weekly assignment Topics Types of pain; Risks of opioids and mitigation strategies including naloxone; bio-psycho-social-spiritual basis of pain; Realities of chronic pain and pain management; pain pyramid; role of inflammation, anti-inflammatory diet and smoking cessation; maximizing non-medication pain treatments; maximizing non-opioid pain medications; treatment of depression, anxiety and insomnia; Importance of physical activity; role of spirituality - Table 3.
List of Demographics for Our Rural Chronic Non-Cancer Pain Patients: Differences Between the Intervention and Original Control Group before Intervention (n = 186)
Demographic Variable Intervention (n = 93) Control (n = 93) P value Discussion Gender* Females (%) 51 (54.8) 51 (54.8) 1.00 Smoker* (%) 63 (67.7) 48 (51.6) 0.04 More smokers in intervention group Use of Benzodiazepine before intervention* (%) 23 (24.7) 38 (40.9) 0.03 More Benzo. use in the control group before intervention Use of Carisoprodol* (%) 3 (3.2) 4 (4.3) 1.00 Positive substance abuse history* (%) 36 (38.7) 9 (9.7) 0.00 More substance abuse dx in the intervention group‡ Age†(%) 0.9 18 to 29 4 (4.3) 4 (4.3) 30 to 39 15 (16.1) 13 (14) 40 to 49 21 (22.6) 28 (30.1) 50 to 59 32 (34.4) 21 (22.6) 60–69 12 (12.9) 18 (19.4) 70–79 9 (9.7) 7 (7.5) 80 to 89 0 2 (2.2) Insurance type§ (%) 0.89 Uninsured 6 (6.5) 4 (4.3) Veterans 1 (1.1) 1 (1.1) Medicare 29 (31.2) 35 (37.6) Medicaid 32 (34.4) 30 (32.3) Private 25 (26.9) 23 (24.7) Psychiatric diagnose§ (%) 0.03 More generalized anxiety in the control group; more PTSD in the experimental group‡ None 27 (29) 23 (24.7) Depression 40 (43) 39 (41.9) Anxiety d/o 11 (11.8) 26 (28) Bipolar 3 (3.2) 2 (2.2) PTSD 11 (11.8) 3 (3.2) Schizophrenia 1 (1.1) 0 Type of pain§ (%) 0.00 More patients with cervical/lumbar radiculopathy in the intervention group‡ Migraine 4 (4.3) 6 (6.5) Osteoarthritis 32 (34.4) 41 (44.1) Rheumatoid Arthritis 1 (1.1) 4 (4.3) Cervical/lumbar Radic. 30 (32.3) 5 (5.4) Diabetic Neuropathy 3 (3.2) 4 (4.3) Fibromyalgia 8 (8.6) 11 (11.8) Somatic dysfunction 8 (8.6) 11 (11.8) GI/pelvic pain 7 (7.5) 11 (11.8) Type of opioid§ 0.24 T #3 5 (5.4) 1 (1.1) Tramadol 7 (7.5) 9 (9.7) Hydrocodone 53 (57) 53 (57) Morphine 8 (8.6) 3 (3.2) Oxycodone 10 (10.8) 15 (16.1) Fentanyl 4 (4.3) 8 (8.6) Methadone¶ 6 (6.5) 4 (4.3) MME strata and number of patients at each strata† (%) 0.94 <20 3 (3.2) 3 (3.2) 20 to 49 43 (46.2) 43 (46.2) 50–99 29 (31.2) 30 (32.3) 100 to 149 4 (4.3) 4 (4.3) 150 – 199 4 (4.3) 4 (4.3) 200 to 249 3 (3.2) 3 (3.2) 250 to 299 1 (1.1) 2 (2.2) 300 to 349 5 (5.4) 1 (1.1) 350 to 399 0 1 (1.1) 400 to 449 1 (1.1) 2 (2.2) - Table 4.
Differences Between Our Rural Chronic Non-Cancer Pain Groups on Secondary Outcomes
Original Control Group N = 93 Original Intervention Group N = 93 Protocol Applied to Control Group (Crossover Phase) n = 93 Is Difference between original Intervention and Crossover Control Significant Total number (%) of patient off COT 2 (2.15) 26 (27.96) 50 (53.76) P < .00 Total number (%) of patients referred to pain specialty/MAT 0 (0) 6 (6.45) 40 (43.01) P < .00 Total number of patients who dropped out of care 3 (3.23) 4 (4.3) 8 (8.6) P = .37 Total number of deaths (any cause) 0 (0) 4 (4.3) 7 (7.5) P = .54 COT, chronic opioid therapy; MAT, medication-assisted treatment.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Most Frequently Read Articles of 2020
- Re: Effects of Implementing a Comprehensive Opioid Reduction Protocol on Overall Opioid Prescribing Among Patients with Chronic, Non-Cancer Pain in a Rural Family Medicine Clinic: A Controlled Crossover Trial
- Medications, Medicating, and Medicated--When, Where, and How--Opioids and Others