
Article Figures & Data
Figures
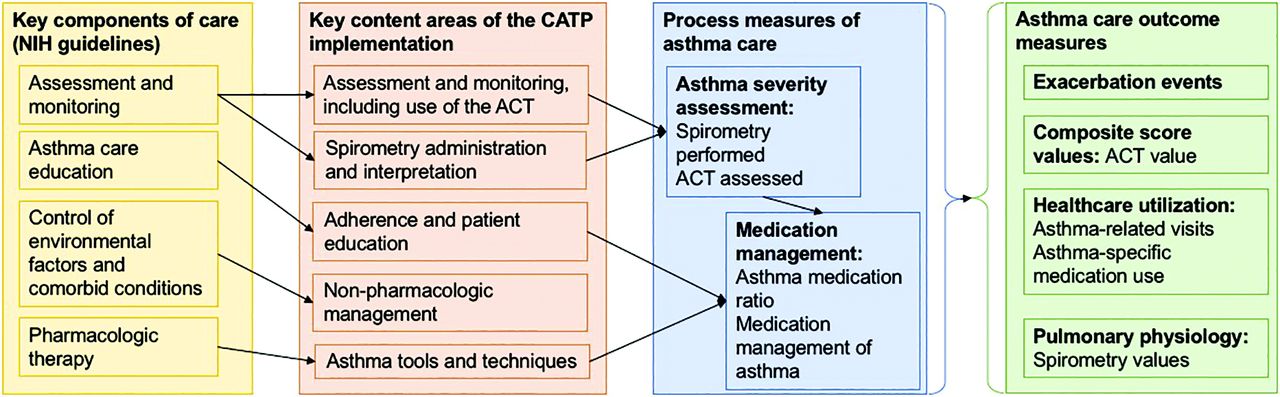
- Figure 1.
Colorado Asthma Toolkit Program (CATP) Conceptual Model. Key content areas were introduced in 3 education and feedback/audit sessions, which were then reinforced via 3 other approaches: 1) organizational change to optimize efficieny integrating CATP processes into practice workflow; 2) decision support tools for asthma management; and 3) online resources to help reinforce and sustain practice changes.
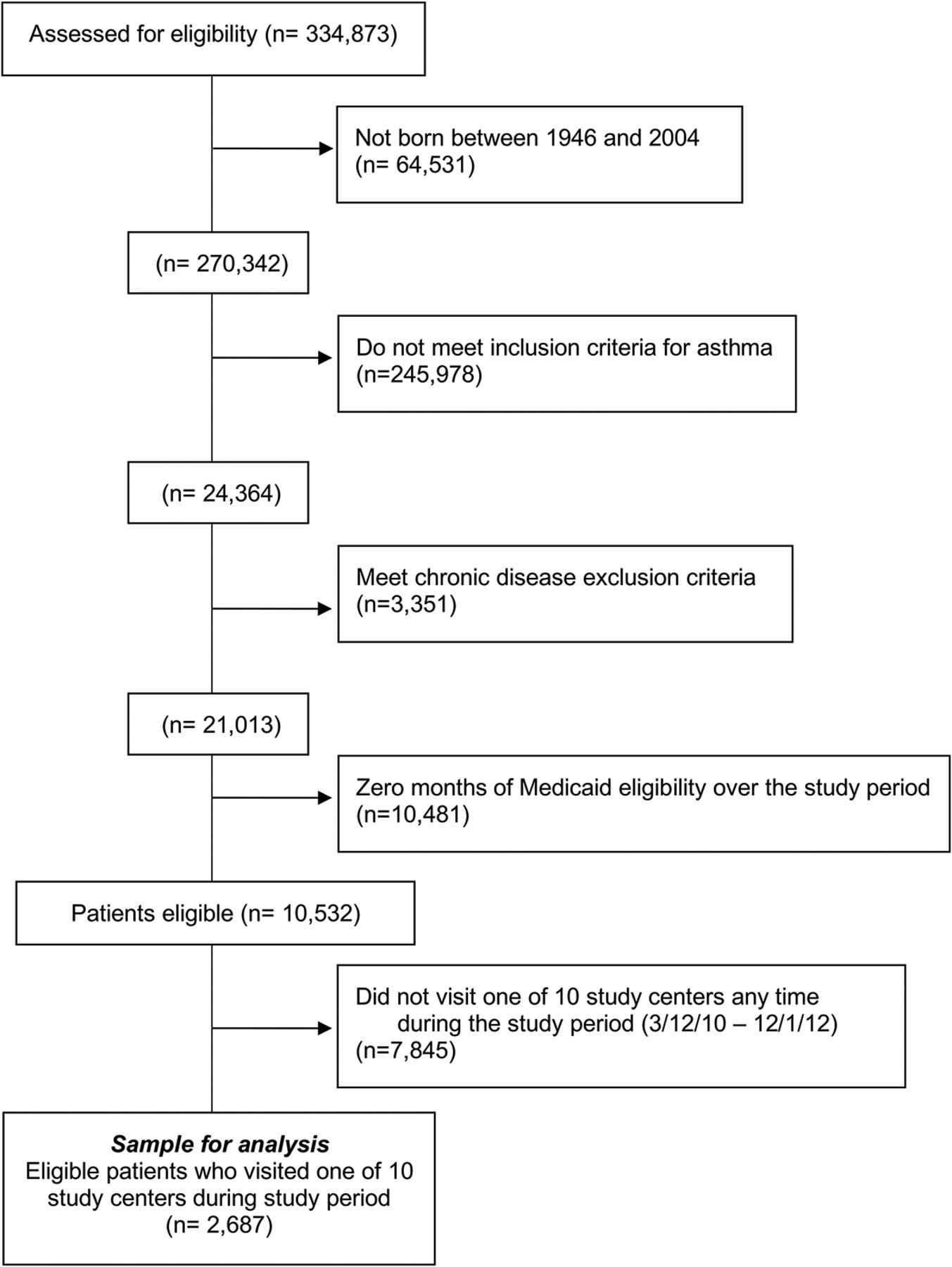
- Figure 2.
The study cohort flow diagram.
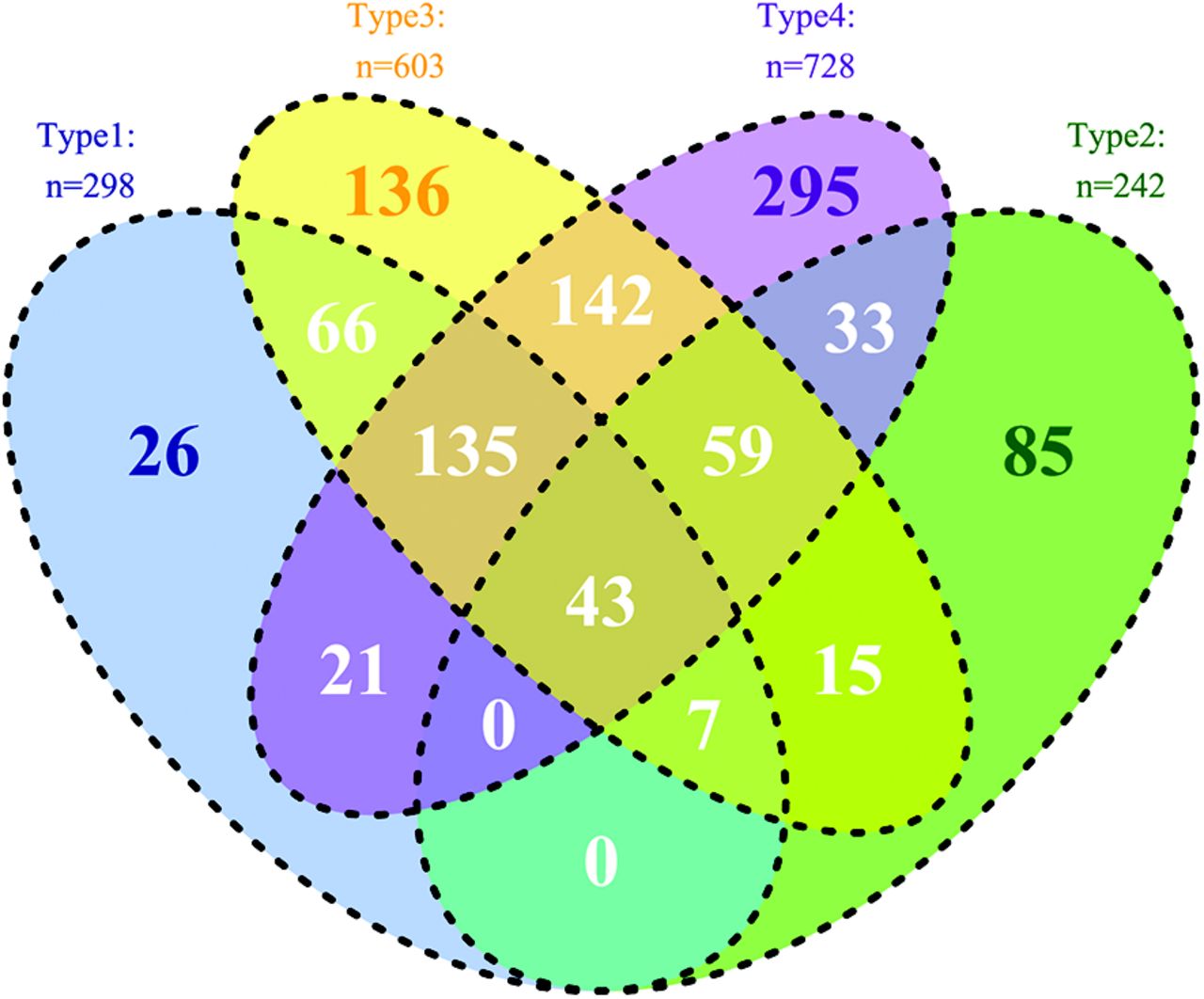
- Figure 3.
Distribution of exacerbations by qualifying event. Type 1: single Emergency Department (ED) or inpatient (IP) visit with primary diagnosis of asthma. Type 2: cluster of 2 visits with asthma diagnosis <14 days apart. Type 3: ICD code or string indicating exacerbation. Type 4: systemic corticosteroid within 0 to 3 days after any type of asthma visit. Note: exacerbations occurring within 14 days of each other were grouped into a single exacerbation.



Tables
Variable Asthma Cohort (n = 2678) Age group, n (%) 5 to 11 years 747 (27.8) 12 to 17 years 374 (13.9) 18 to 64 years 1566 (58.3) Sex Male 899 (33.5) Female 1788 (66.5) Race, n (%) White 874 (32.5) Black/African American 294 (10.9) Other 128 (4.8) Unknown 1391 (51.8) Ethnicity Hispanic/Latino 854 (31.8) Not Hispanic/Latino 1254 (46.7) Unknown 579 (21.6) Comorbidity count, n (%)* 0 340 (12.7) 1 522 (19.4) 2 425 (15.8) >2 1400 (52.1) Medicaid eligibility [months of 33 study months], (median, IQR) 33 (31 to 33) ↵* Number of Healthcare Cost and Utilization Project (HCUP) Chronic Condition Indicator (CCI) “body systems” wherein the patient has one or more comorbidities, excluding respiratory.
IQR, interquartile range.
Pre-Intervention Post-Intervention P Value Asthma severity assessed Spirometry performed, N, (% of patients) 32 (1.2%) 272 (10.1%) .0031,2 ACT assessed, N, (% of patients) 0 (0.0%) 310 (11.5%) N/A HEDIS measures Patients meeting inclusion criteria for HEDIS definition of persistent asthma (% of study sample) 129 (4.8%) 228 (8.5%) <.00011 Asthma medication ratio: percentage identified as having persistent asthma who had a ratio of controller medications to total asthma medications of 0.50 or greater 52.3% 58.5% .3 Medication management for people with asthma: percentage identified as having persistent asthma who were dispensed an asthma controller medication that they remained on for at least: 75% of their treatment period 27.6% 34.2% .2 50% of their treatment period 56.9% 63.2% .3 All P values in this table obtained using generalized linear mixed models with random effects to control for variability between clinics. Random effects for subject were included when 1) applicable, and 2) random treatment effects by clinic were included when significant.
ACT, Asthma Control Test; HEDIS, Health care Effectiveness Data and Information Set.
Exacerbation Events Pre-Intervention Period Post-Intervention Period P Value Total exacerbations 386 414 Patients with no exacerbations, N (%) 2410 (89.7) 2389 (88.9) .3‡ Exacerbations per person among those with 1 or more exacerbations, Median (IQR) (min, max) 1 (1–1) (1,9) 1 (1–1) (1,8) 1.0‡ Percent of exacerbations with a qualifying event of type:* Type 1: single ED or IP visit with primary diagnosis of asthma 112/386 (29.0) 109/414 (26.3) .3‡ Type 2: cluster of 2 visits with 1 to 14 days between, both with an asthma diagnosis 85/386 (22.0) 89/414 (21.5) .5‡ Type 3: ICD code (5th digit) or string indicating exacerbation 220/386 (57.0) 245/414 (59.2) .3‡ Type 4: systemic corticosteroid within 0 to 3 days after any type of visits for asthma 265/386 (68.7) 275/414 (66.4) .4‡ Healthcare utilization 1. IP visits with primary asthma diagnosis (number of visits) 5 1 — 2. ED visits with primary asthma diagnosis (number of visits) 131 121 — 3. Outpatient visits with an asthma diagnosis (number of visits) 1888 1910 — 4. Asthma-specific medication use (n prescriptions)† 5,221 7,116 — 4a. Controller use 2,224 2,987 4b. Reliever use 2,997 4,129 Healthcare utilization—number of patients with at least 1 of the following: 1. IP visit with primary asthma diagnosis 5/2687 (0.2) 1/2687 (0.0) .1 2. ED visit with primary asthma diagnosis 83/2687 (3.1) 92/2687 (3.4) .4 3. Outpatient visits with an asthma diagnosis 609/2687 (22.7) 649/2687 (24.2) .1 4. Asthma-specific medication use† 1094/2687 (40.7) 1334/2687 (49.6) <.0001 4a. Controller use 468/2687 (17.4) 585/2687 (21.8) <.0001 4b. Reliever use 1005/2687 (37.4) 1240/2687 (46.2) <.0001 Composite scores: ACT Observations, N 0 543 — ACT score = “in control,” n (% of all ACTs) n/a 325 (60.2) — ACT score = “poorly controlled,” n (%) n/a 132 (24.4) — ACT score = “very poorly controlled,” n (%) n/a 83 (15.4) — Pulmonary physiology: FEV1/FVC percent predicted Observations, N 13 456 — Mean value, % predicted, (standard deviation) 82.5 (11.1) 77.9 (13.1) .1‡ ACT, asthma control test; ED, emergency department; IP, inpatient; OP, outpatient; IQR, interquartile range.
↵* Percentages add up to greater than 100% as an exacerbation may have more than one qualifying event.
↵† This includes controllers and relievers but not steroids.
↵‡ Random effects for subject were included when applicable.
- Appendix Table 1.
Number of Patients Defined as Having Persistent Asthma by Measurement Period
Pre-Intervention Measurement Period Post-Intervention Measurement Period Before Pre Pre Before Post Post (12 March 2009 to 11 March 2010) (12 March 2010 to 11 March 2011) (2 December 2010 to 1 December 2011) (2 December 2011 to 1 December 2012) ≥1 asthma ED visit 64 83 90 92 ≥1 asthma IP visit 0 5 3 1 ≥4 asthma OP visits & ≥2 asthma medications 39 36 61 46 ≥4 asthma medications (not all leukotriene modifiers) 186 258 319 374 ≥4 leukotriene dispensing events & ≥1 asthma diagnosis 1 0 0 2 Any type(s) 221 313 379 438 ED, emergency department; IP, inpatient; OP, outpatient.
N % Infectious and parasitic disease 92 3.42 Neoplasms 67 2.49 Endocrine, nutritional, and metabolic diseases and immunity disorders 1246 46.37 Diseases of blood and blood-forming organs 254 9.45 Mental disorders 1557 57.95 Diseases of the nervous system and sense organs 1084 40.34 Diseases of the circulatory system 783 29.14 Diseases of the respiratory system* 1987 73.95 Diseases of the digestive system 717 26.68 Diseases of the genitourinary system 670 24.93 Complications of pregnancy, childbirth, and the puerperium 169 6.29 Diseases of the skin and subcutaneous tissue 213 7.93 Diseases of the musculoskeletal system 592 22.03 Congenital anomalies 243 9.04 Certain conditions originating in the perinatal period 1 0.04 Symptoms, signs, and ill-defined conditions 249 9.27 Injury and poisoning 20 0.74 Factors influencing health status and contact with health services 386 14.37 All records include only conditions marked as “chronic” in HCUP.
↵* Respiratory conditions excluded from comorbidity count calculation.




{kind=link}
{kind=link}
{kind=link}