
Abstract
Objective: Cardiovascular disease (CVD) is the most common chronic health condition affecting Americans. One important group of Americans that health researchers have noted as key to understanding general population health and wellbeing are veterans of the US military. The healthy soldier effect has been used to explain the health benefits of military service during and for a period of time after service. The purpose of this study was to examine the prevalence of CVD in a national sample with specific attention paid to reported CVD across ages.
Methods: A total of 153,556 veteran and nonveteran respondents from the National Health Interview Survey were examined for the likelihood of reporting the type and number of cardiovascular conditions.
Results: Veterans report higher rates of certain CVD conditions and report a higher number of CVD conditions than nonveterans. Veterans also reported higher numbers of CVD conditions at younger ages (ages 25 to 70 years) than nonveteran counterparts. At older ages (ages 70 to 85+ years), nonveterans reported higher numbers of CVD conditions than veterans.
Discussion: Our findings are consistent with the studies that indicate a waning healthy soldier effect for young veterans potentially due to the unique circumstances of the current conflicts.
Cardiovascular disease (CVD) is the most common chronic health condition in the United States. Almost 30% of Americans suffer from at least 1 cardiovascular condition, and 50% of adults 60 years of age or older have 1 or more cardiovascular conditions.1 CVD is the leading cause of death for American men and women and contributes to 31% of all deaths in the United States each year.1 One important group that health researchers have noted as key to understanding general population health are veterans of the American military.2 There are approximately 21 million veterans,3 representing about 9% of the civilian noninstitutionalized adult population and approximately 7% of the total American population overall.2,4 In this article, “veteran” is defined as those who have ever served in the United States Armed Forces. Although self-reports of having ever served may not meet the strict legal criteria for being eligible for veteran affairs benefits, the definition is consistent with that used by the National Health Interview Survey (NHIS), the source of data for the current analysis.1
Military service has long been associated with both positive and negative health outcomes.6⇓–8 Active-duty service members tend to be more physically fit and less likely to be overweight than same-aged nonmilitary civilians.9 This phenomenon is often referred to as the “healthy soldier effect” (HSE).9 The HSE is an adaptation of the healthy worker effect, the phenomenon whereby employed workers have lower mortality than the general population.10 The HSE likely occurs, in part, because only the healthiest individuals join the military and in part because early-life physical training and health maintenance requirements for active-duty military service members combine to reduce mortality risks throughout middle age and later life.9 The protective effects of military service on disease mortality have been estimated to last from 10 to 30 years after military service has ended11 but most notably in reduced deaths due to CVD.9,12⇓–14
Despite a reduction in mortality related to CVD, research indicates that veterans experience higher rates of CVD, are more likely to suffer from mental health problems and substance use disorders, and are more likely to have musculoskeletal disorders than nonveterans.15⇓⇓–18 Veterans are more likely to engage in risky health behaviors associated with CVD, such as alcohol and tobacco use and abuse. A longitudinal study indicates that veterans across ages are more likely to develop cardiovascular conditions over the course of a 20-year period than nonveterans, even when controlling for sociodemographic and other factors.19
Past research on the cardiovascular health of Veterans has largely taken place among veterans enrolled in the Veterans Administration (VA) health care system.20,21 This can be problematic because VA data tend to capture veterans who are in poorer health22 and who are more likely to report significant service-connected disability than non-VA-enrolled veterans.23,24 Second, VA-enrolled veterans are older than non-VA-enrolled veterans, with veterans over the age of 75 more likely to enroll in, and use, VA services than younger veterans. These older veterans are also more likely to have chronic health conditions in need of ongoing care.25 Third, most veterans are not enrolled in VA health care services.26 Recent estimates suggest that roughly 40% of eligible military veterans accessed and used VA services.25,27 The use of VA-only data might provide an incomplete picture of veteran cardiovascular morbidity, therefore, making it important to look to data sources that can capture a wider veteran population.
The purpose of this study was to examine the prevalence of CVD in a national sample of veterans and nonveterans with specific attention paid to individuals reporting CVD across ages. Specific attention was given to how veterans and nonveterans differ in their reports of specific cardiovascular issues (hypertension, heart problems, heart attack, coronary heart disease, and stroke) and the number of comorbid cardiovascular conditions by age.
Methods
The NHIS is a publicly available, nationally representative health survey of noninstitutionalized individuals living in the United States. The NHIS is conducted by the Centers for Disease Control and Prevention's National Center for Health Statistics (NCHS).28 The total household response rate for the survey was 75.7%.29 The last 4 available years of the NHIS were pooled (2012, 2013, 2014, and 2015) to form 1 dataset. The analytic sample included 153,556 respondents that answered questions about veteran status, NHIS-designated cardiovascular conditions, and sociodemographic characteristics, including age, sex, race/ethnicity, education, marital status, and health status.
Variables
Veteran Status
The NHIS designates respondents who identified themselves as having ever served in the United States Armed Forces as “veterans.” For the purposes of the present study, these respondents are referred to as having veteran status.
Cardiovascular Health Conditions
The NHIS questionnaire asks respondents whether they have “ever been told by their doctor that they had” 5 different cardiovascular conditions: hypertension, coronary heart disease, heart condition, stroke, and heart attack (myocardial infarction). The NHIS-designated categories are used for analyzing the cardiovascular conditions presented in this study. Each condition is examined individually, and to understand whether and how comorbid cardiovascular conditions differ by veteran status, an index, or count, was created. This index adds each of the 5 separate CVD conditions into a new variable that ranged from 0 to 5, with 0 representing those with no cardiovascular conditions and 5 representing those reporting all 5 CVD conditions.
Sociodemographic Characteristics
Race and ethnicity was coded into 4 categories2,30: non-Hispanic white, non-Hispanic black/African American, non-Hispanic Asian and other race, and Hispanic/Latino. Sex was coded as 1 = male and 0 = female. Marital status was coded as 1 = married/unmarried coresidential partners, 2 = divorced/separated, 3 = widowed, and 4 = never married. Educational level was coded so that 1 = less than a high school (HS) diploma, 2 = HS diploma, or general equivalency degree, 3 = some college or 2 year college degree, 4 = 4 year college degree, 5 = graduate work or graduate degree. Age was coded in years with the exception of people over the age of 853 A measure of self-rated health was included in this analysis; respondents rated their health as 5 = excellent, 4 = very good, 3 = good, 2 = fair, or 1 = poor.
Analytic Strategy
To understand how veterans differ from nonveterans across cardiovascular conditions, analyses were conducted in 3 stages. First, bivariate analyses (t test and χ2 tests) explored how veteran status varied by cardiovascular conditions and sociodemographic characteristics. Second, 5 logistic regression analyses examined how veteran status predicts the odds of having each of the reported cardiovascular conditions. Finally, a negative binomial regression analysis examined how veteran status predicts the odds of reporting multiple comorbid cardiovascular conditions. A negative binomial regression analysis was used because the indices of multiple cardiovascular conditions were discrete counts following a Poisson distribution with evidence of overdispersion (conditional variances were larger than the means) in the data. All analyses were weighted to account for the complex survey design of the NHIS survey instrument according to NHIS instructions.
Results
Table 1 displays the results of the bivariate analyses that indicate that veterans differ from nonveterans across heart conditions and other sociodemographic characteristics. Hypertension was the most common cardiovascular condition affecting 33.8% of respondents. Almost 43% of veterans reported hypertension compared with 32.8% of nonveterans. Similar patterns were found in coronary heart disease affecting 9.9% of veterans and 5.5% of nonveterans. Other heart conditions were reported by 11.4% of veterans and 8.3% of nonveterans. Veterans also reported more stroke (5.3% compared with 3.5%) and heart attacks (7.8% compared with 4.1%) than nonveterans. For comorbid heart conditions, nearly 50% of veterans reported at least 1 heart condition compared with 39% of nonveterans.
Bivariate Analyses by Veteran Status
Veterans also differed from nonveterans across all sociodemographic characteristics. Military veterans tended to be non-Hispanic white (76.7% compared with 61.2%) and male (66.4% compared with 42.2%) compared with nonveterans. Fewer veterans had never married (16%) compared with nonveterans (23.3%); said another way, veterans were more likely to have been married. Veterans also had higher levels of education, with 34.9% having a high school diploma or less compared with 41.4% of nonveterans. Veterans in the sample were also significantly older (56.2 years) than nonveterans (48.9 years).
The next step was to understand the difference in odds of having a cardiovascular condition when controlling for the differences highlighted in the section above. This is particularly important because the veterans in this sample tend to be older and male, both of which are unique risk factors for CVD. At the same time, veterans are more educated, more likely to be married, and more likely to be white, all known to be protective against cardiovascular conditions. These factors served as controls when further exploring whether veteran status has an independent effect on the odds of having a particular cardiovascular condition. Table 2 displays the results of 5 different multivariate logistic regression models testing the association between veteran status and reporting CVD conditions. Each odds ratio (OR) and 95% confidence interval (CI) displayed in the table represent a separate regression model fully adjusted for sociodemographic factors.
Odds Ratios for Veterans Compared to Nonveterans Adjusting for Sociodemographic Characteristics*
Table 2 indicates that veterans have an odds of reporting hypertension that are 65% higher than the odds of nonveterans reporting hypertension, controlling for sociodemographic characteristics. Similarly, veterans are 76% (OR, 1.76) more likely to report a diagnosis of coronary heart disease and 125% more likely to report having had a heart attack (OR, 2.25). Veterans and nonveterans had similar rates of reporting “other heart problems” and stroke, controlling for all factors.
Next, a negative binomial regression model was used to understand whether veterans have higher counts of CVD. Table 3 displays the results of this analysis controlling for all sociodemographic characteristics. An interaction term for veteran status by age was included in these models. The purpose of the interaction term was to understand whether the relationship between the count of cardiovascular veteran status and age has a different trajectory based on veteran status, controlling for other sociodemographic factors.
Negative Binomial Regression for Cardiovascular Conditions by Veteran Status and Sociodemographic Characteristics
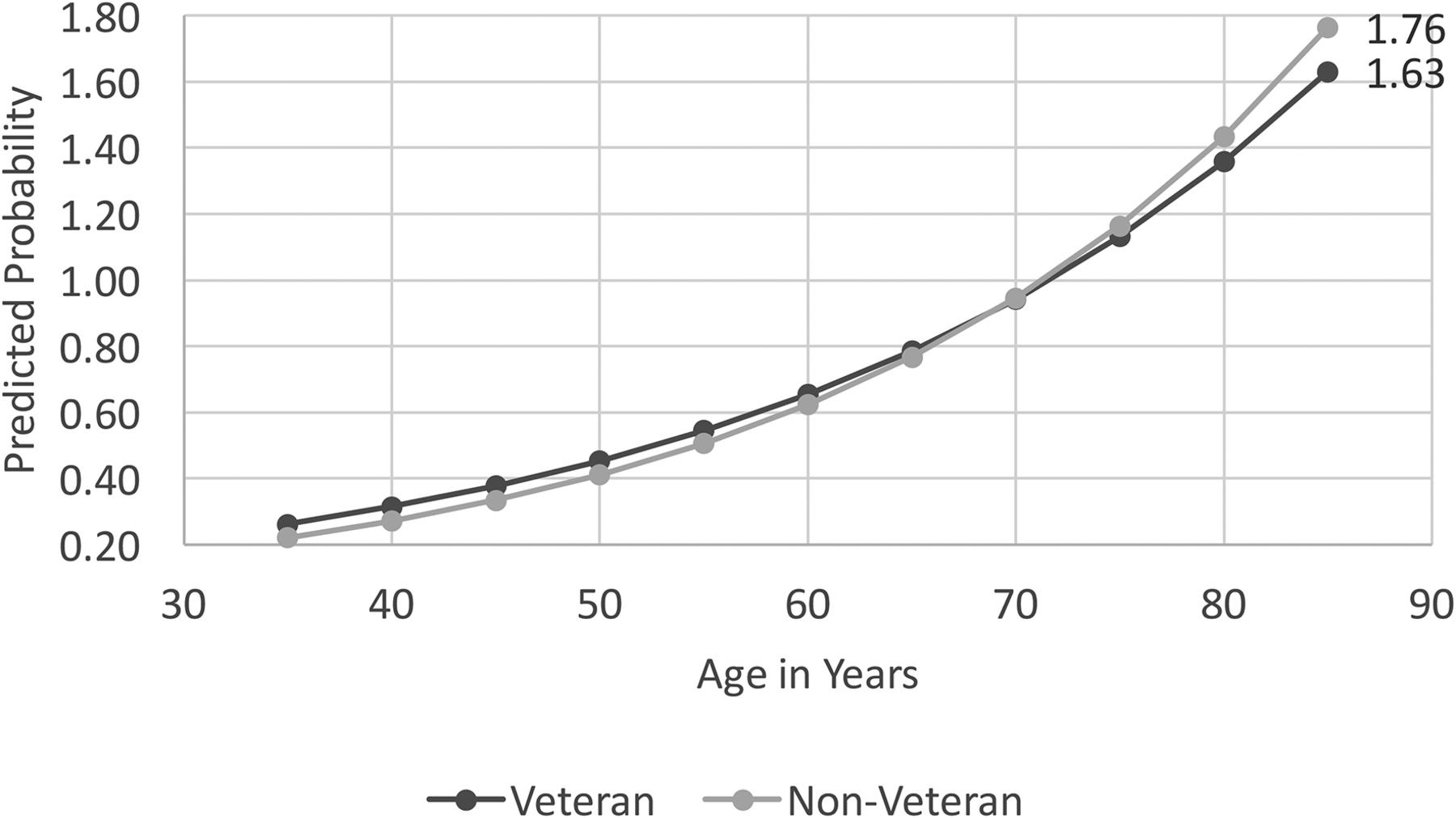
In the negative binomial regression analysis, an incidence rate ratio (IRR) was calculated. An IRR is interpreted to be the odds of having a higher incidence (number) of cardiovascular conditions. Table 3 shows that veteran status is associated with a 42% higher odds of having a higher number of cardiovascular conditions than nonveterans, controlling for sociodemographic characteristics. The interaction term “veteran status*age” in the model was a significant predictor of the count of cardiovascular conditions. This means that veteran status moderates the relationship between age and cardiovascular conditions (IRR, 0.99; 95% CI, 0.99–0.99). The CI seems to be the same because of rounding to 2 decimal places in the tables. Next, the predicted count of cardiovascular conditions (using the STATA margins command) for veterans and nonveterans by age was calculated controlling for all the other factors in the model. Figure 1 displays this relationship.
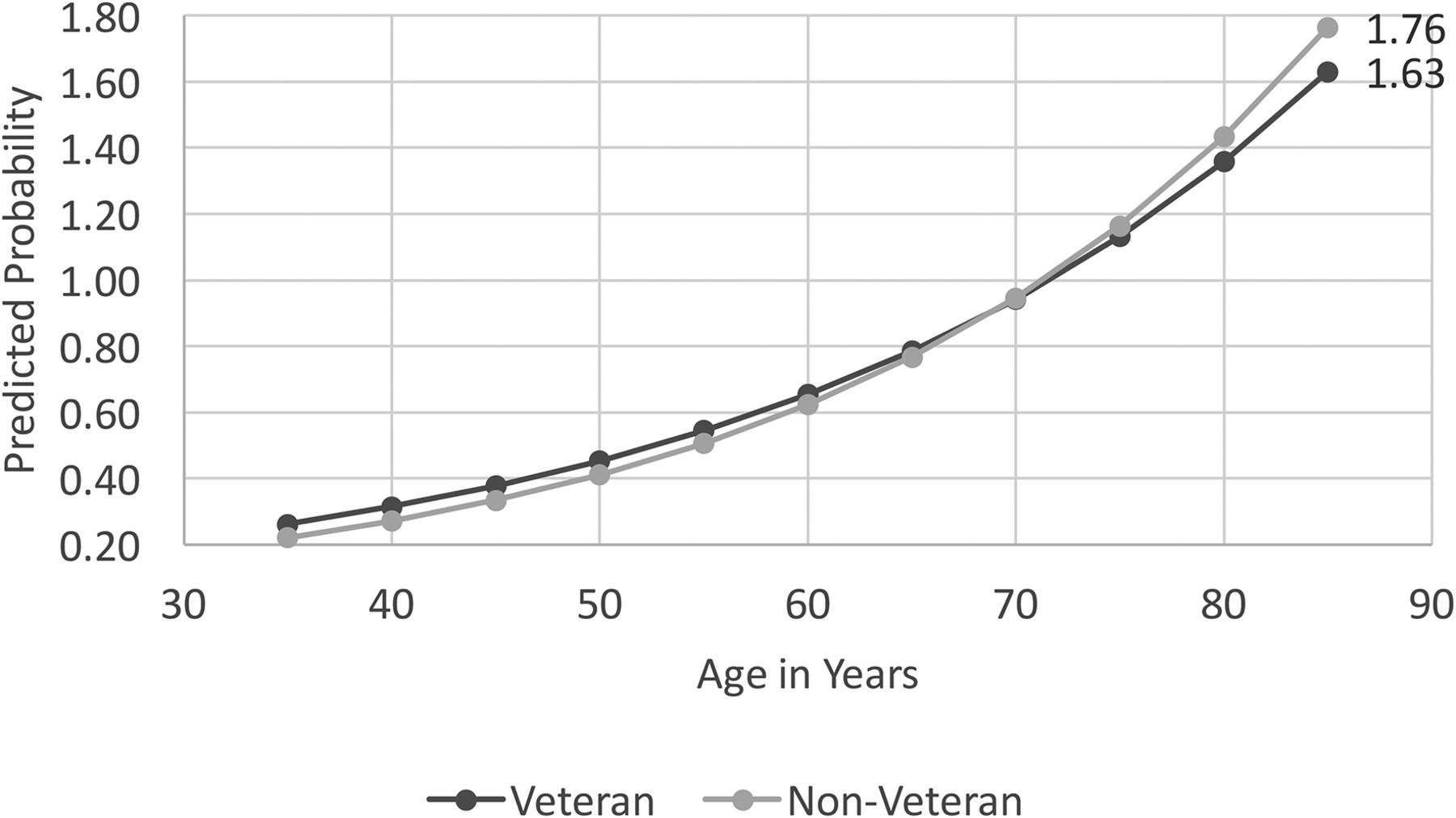
Predicted Count of Heart Conditions by Veteran Status and Age.
Each dot (dark gray for veterans and light gray for nonveterans) represents the predicted count of cardiovascular conditions. Recall that an index variable for “cardiovascular conditions” was created to be the sum of all 5 cardiovascular conditions identified in the study. The index ranges from 0 (no conditions) to 5 (all cardiovascular conditions), and the predicted probability (obtained from the margins command in Stata) represents the predicted count of cardiovascular conditions. Predicted counts of cardiovascular conditions were calculated for veterans and nonveterans ages 35 through 85+ and are presented in Figure 1. For a veteran at age 35, the predicted count of cardiovascular conditions is 0.26 and the predicted count for nonveterans is slightly lower at 0.22. Although these differences are small, they are statistically significant (P < .01). Veterans continue to have higher predicted counts of cardiovascular conditions until about age 70 where the counts are the same, 0.94 for Veterans and 0.95 for nonveterans. After age 70, nonveterans have higher counts of cardiovascular conditions and at ages 85 and older; the predicted count for veterans is 1.63 conditions and 1.76 for nonveterans. In other words, after age 70, nonveterans are more likely to report higher CVD counts.
Discussion
Data from the NHIS were used to examine how a national sample of veterans and nonveterans differed by CVD condition, the number of comorbid CVD conditions, and whether, and how, veterans and nonveterans differed in their CVD count by age. Findings indicate an emerging health crisis for younger veterans, as their rate of CVD morbidity and comorbidity is higher than in same-aged nonveteran civilians. Starting at age 35, Veterans have a greater likelihood of reporting a greater number of cardiovascular conditions. Around age 70, there is a change in reporting, whereby nonveterans are more likely to report a greater number of cardiovascular conditions. Higher rates of CVD with a greater likelihood of CVD comorbidity at younger ages is a recipe for early on-set CVD mortality later in life,31 which may help explain this switch-over effect. Said another way, there may be fewer older Veterans reporting CVD conditions because they have not survived into older ages.
These findings support an emerging literature that questions whether the HSE is as relevant for the newest generation of veterans as it once was.2,32,33 Researchers from the VA note that “the healthy solider/worker effect gradually subdued over time.”33 VA data estimate that male and female veterans have fewer expected life years (0.8 and 1.2 years, respectively) than nonveterans.4,33 This is concerning, because, as a group, veterans have greater access to health care, are more educated, and they tend to earn higher wages than the nonveteran civilian population.34,35 Despite greater access to these health protective resources, those holding veteran status seem to have overall poorer cardiovascular health, and at younger ages, than their nonveteran counterparts.
Previous studies have explored combat exposure and long-term cardiovascular health but often neglect other explanatory factors for differences in CVD outcomes, such as preservice pre-existing mental health conditions or low socioeconomic status.36 Another potential explanation is found in how military service varies by era and conflict.37 Veteran cohorts experience different social and economic conditions that play a role in their long-term health.8 Recent, younger veterans are more likely than older veterans to have had lower grades in high school at the time of enlistment, come from single-parent households, and have parents with lower educational achievement,38 which are all predictors of persistent poverty over the life course, and all related to overall poorer cardiovascular health.
The NHIS does not ask about combat exposures, but the available evidence suggests that the recent wars in Iraq and Afghanistan have been more psychologically stressful than wars of other eras. This is due to a lack of clearly designated front lines and clear demarcation between enemy combatants and the civilians populations in which the enemy tended to embed; the higher number of war-zone tours; and longer deployments than earlier wars.39 In addition, the wars in Iraq and Afghanistan relied more heavily on service members from National Guard and Reserve units that, in general, have a lower state of military preparedness32 and less access to military institutional support mechanisms such as Family Readiness Groups that provide crucial social, economic, and emotional support before, during, and after deployment.40 Emerging evidence suggests increased risks to health for Iraq and Afghanistan veterans who seem to have higher rates of tobacco and alcohol use,32,41,42 known risk factors for CVD, and to early onset mortality. Interestingly, the effects of tobacco and alcohol use seem to marginally affect the likelihood of veterans reporting higher rates of CVD conditions than nonveterans when controlling for age; this has been documented elsewhere.43
Limitations
There are several limitations to this study. Self-reports of the presence of a diagnosis of CVD conditions was explored. Individuals may not report specific conditions accurately or may under or over report certain diagnoses. That said, the NHIS is among the best available data for monitoring chronic disease among veterans living in the general American population. Another limitation is that data are cross-sectional and that only allows for an examination of veterans and nonveterans at a single time point. It is impossible to examine individuals across time. Therefore, understanding the development of CVD or the propensity of death from CVD and the difference between veterans and nonveterans remains out of reach when using NHIS data. Therefore, it is only possible to speculate on how higher CVD morbidity and comorbidity in younger veterans may indicate risks for later-life early CVD mortality.
Another distinct limitation is the possibility for “lead time” bias to skew results. Because veterans tend to have greater access to health care, there is also an increased chance that interaction with health care providers will result in receiving a CVD diagnosis and at earlier ages. The current analysis did not control for time-since-diagnosis, as this data are not available.
Despite these limitations, the findings of this study are consistent with research that demonstrates a link between military service and cardiovascular health.44 This study provides support for emerging research documenting the erosion of the HSE.32,43 When the data are taken together, this study provides more evidence of a looming cardiovascular health crisis for American veterans, who seem to have CVD at younger ages and at higher rates than nonveterans.
Future research should continue to explore the potential erosion of the HSE32 by examining other cardiovascular health correlates, such as risk-taking behavior, substance use and abuse, alcohol use, smoking, obesity, and exercise regimes. Spiro et al. 2016 (p. 7)8 argue that “Rather than asking whether military service has long-term health effects, the more appropriate questions are, for whom does military service have long- term positive and/or negative effects, in which domains, and why?” The research presented here moves us closer to answering these important questions.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
↵1 Veteran status is defined according to American legal code (38 U.S. Code § 101) as military personnel that have “served in the active military, naval, or air service” and were “discharged or released therefrom under conditions other than dishonorable”. 38 U.S. Code § 101establishes the legal definition for Veteran as a means to determine eligibility for Veterans' Benefits 5. Veterans' Benefits., Public Law 85–857, §1, September 2, 1958, 72 Stat. 1105, 38 USC §101 (1958).
↵2 Race and ethnicity (Hispanic origin of respondents) was collected by the NHIS following the guidelines set forth by the Office of Management and Budget Directive 15 30. OMB, Budget OoMa. Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity. In: Register F, editor. 1997. p. 58782–90, 31. NCHS National Center for Health Statistics. Public Use Data File and Documentation. 2013.
↵3 In the NHIS data, age is top coded so that the public release data does not identify individuals above the age of 85 years.
↵4 The authors of the NSVAS report on Veteran life expectancy and mortality note that the higher mortality rate estimates for Veterans is incomplete because it is missing older and healthier Veterans. Data quality issues are noted above, but it is worth remembering that only about 40 percent of eligible Veterans are enrolled in VA healthcare.
To see this article online, please go to: http://jabfm.org/content/32/1/50.full.
- Received for publication May 15, 2018.
- Revision received August 30, 2018.
- Accepted for publication September 7, 2018.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Blood Pressure Control and Maintenance in a Prospective Cohort of Younger Veterans: Roles of Sex, Race, Ethnicity, and Social Determinants of Health
- Opportunities to Address Specialty Care Deserts and the Digital Divide: VAs Virtual Hub-and-Spoke Cardiology Clinic
- Conversations, Communication and Counseling Are Key Family Medicine Tactics to Improve Patient Health