
Article Figures & Data
Figures
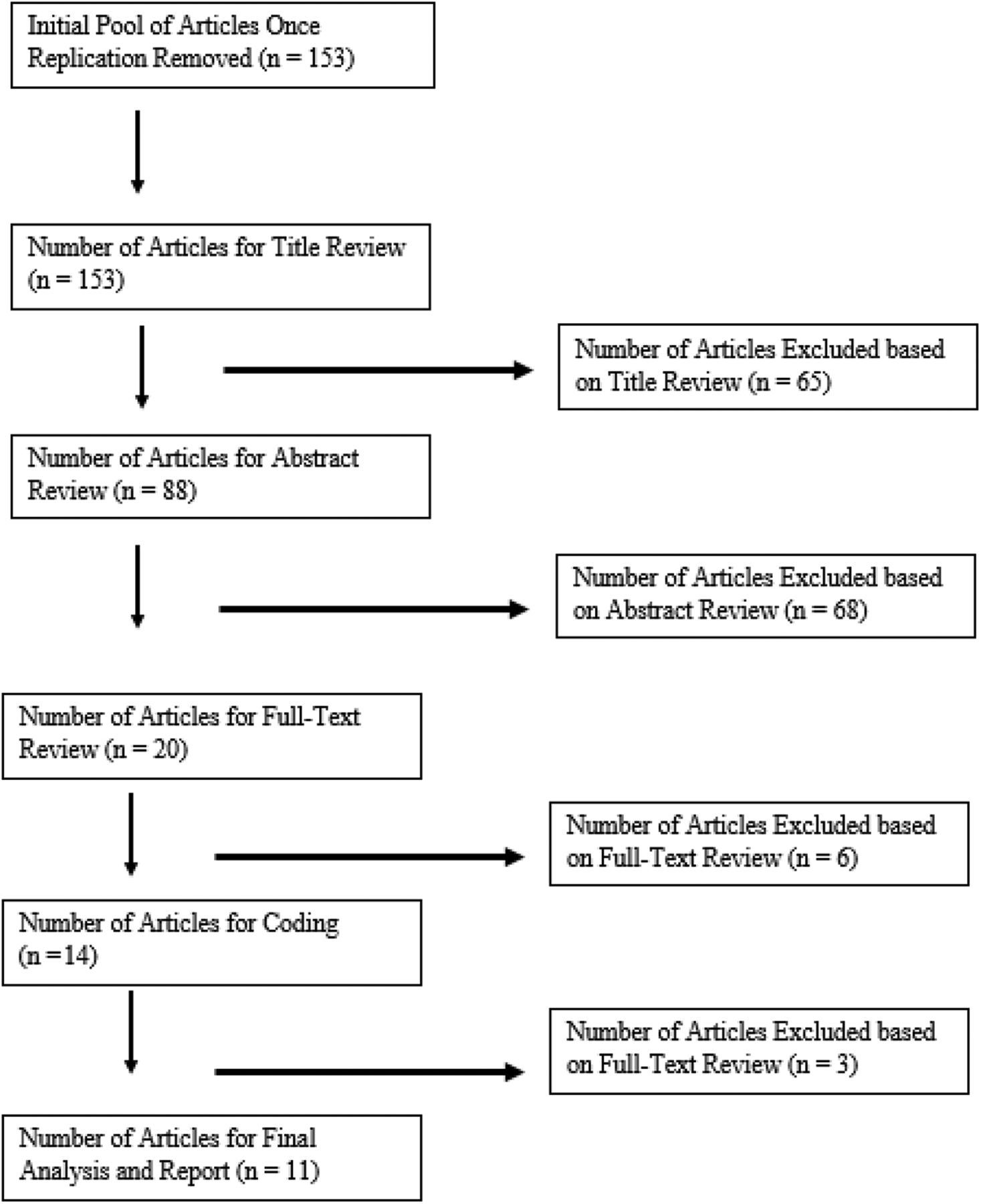
- Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) chart of literature search for Problem-solving therapy (PST) studies for treating primary care patients' depression and/or anxiety.
- Figure 2.
Funnel Plot for Publication Bias in Problem-solving therapy (PST) Studies for Treating Primary Care Patients' Depression an/or Anxiety.
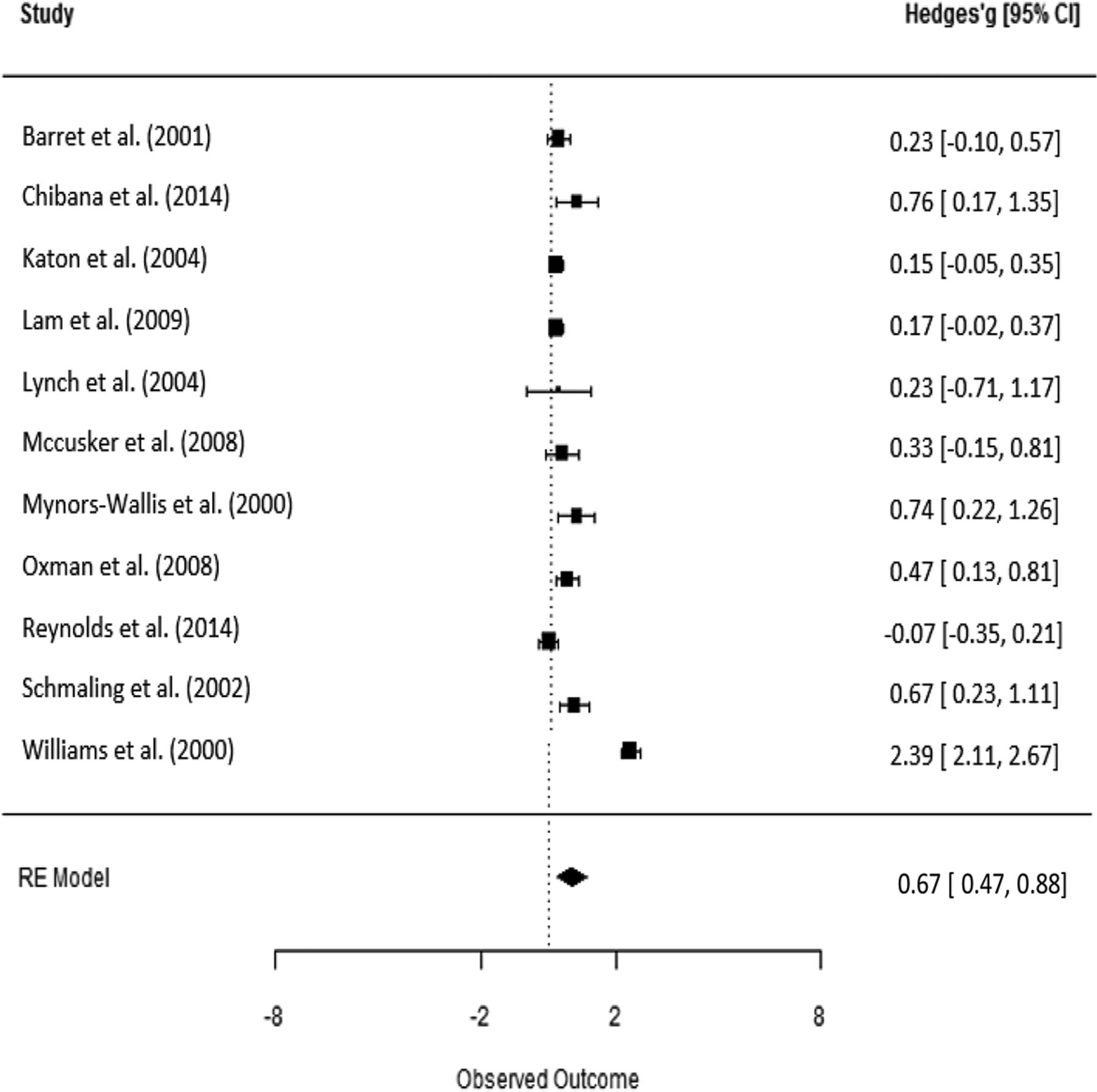
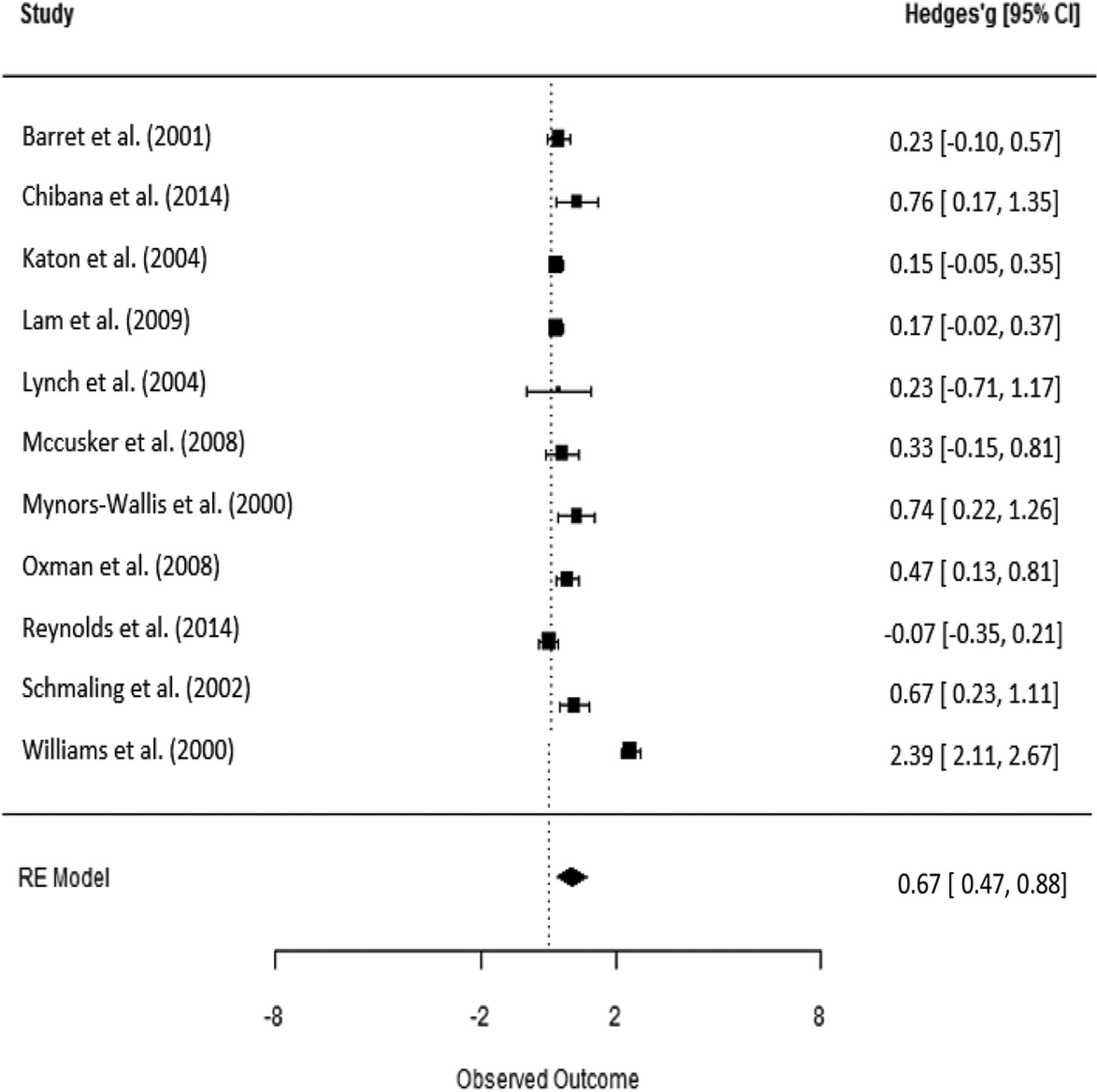
- Figure 3.
Forest Plot of PST Treatment Effect Size Estimates for Treating Primary Care Patients' Depression and/or Anxiety per Study.


Tables
- Table 1.
Study Characteristics for Problem-Solving Therapy as Intervention for Treating Depression and/or Anxiety Among Primary Care Patients (n = 11)
Author Sample* Demographics† Control‡ Provider and PCP's role in PST (if applicable) PST/PST-PC Dosage Diagnostic or Symptom Severity Criteria Depression and/or Outcome Measures Barrett et al. (2001) T = 80
C1 = 80
C2 = 81§44.1 year old (SD NR), MED
PlaceboPh.D-level psychologists. PCP no involvement 6 PST-PC sessions, lasting about 1 hour for the first visit and 30 minutes for subsequent visits. DSM-III-R, HDRS, PRIME-MD HSCL-D-20
HDRS36.1% male, 90% white. Chibanda et al. (2014) T = 30
C = 2824.5 years old (SD = 4.9) MED Trained Peer Counselor. PCP no involvement 12 sessions (60 mins per session) group PST session which were modeled after a 7-step management plan for depression published earlier (Abbas et al., 1994) DSM-IV EPDS % male NR Race NR Katon et al. (2004) T = 164
C = 16558.3 years old (SD = 12), TAU Registered nurses in collaboration with the PCP Medication OR PST-PC, there is a stepped-care algorithm¶ PHQ-9
Did not require diagnostic criteriaSCL-90 depression 35% male, 75.4% white. Lam et al. (2009) T = 149
C = 15071.8 years old (SD = 7.0) AC‖ Primary care physicians 3 sessions of modified PST-PC (Mynors-Wallis et al., 2000), first session 30 to 45 minutes. session 2 & 3 20 to 30 minutes. HADS score HADS (AS), HADS (DS) 43.14% male, SF-36 mental Race NR Lynch et al. (2004) T = 9
C1 = 9
C2 = 1338.5 years old (SD = 13.7), AC**
TAURegistered nurses. PCP referral, no other involvement 6 sessions of telephone-based PST (adopted Nezu, Nezu, & Perri, 1989) PRIME-MD
HRSDPRIME-MD, HRSD
BDI, DHP-D-A17% male Race NR McCusker et al. (2008). T = 36
C = 3273.3 years old (SD = 8.6), TAU Depression care practitioner supervised by (and in collaboration with) PCP 4 sessions PST intervention (60- minute first session, 30 mins for the rest) developed based on IMPACT PHQ-2 SCL-20, SF-12
SCID33.8% male Race NR Mynors-Wallis et al. (2000) T1 = 80
T2 = 35
C = 3635 years old (SD = NR), MED General practitioner 6 sessions PST-PC, with first session 1 hr, others 30 minutes RDC HDRS 23% male, Nurse and General Practitioner (PCP) HDRS score BDI-I 95% white Oxman et al. (2008) T = 72
C = 6955.2 years old (SD = 16), TAU Masters level counselor. PCP referral, no other involvement 6 sessions PST-PC, with first session 1 hr, others 30 minutes DSM-IV, HAM-D, HAM-D, MADRS
HSCL-D-2041.8% male, PRIME-MD 96.5% white Reynolds et al. (2014) T = 125
C = 12236.5 years old (SD = 10.9) TAU Social workers and mental health nurses 6 to 8 sessions PST-PC, with first session 1 hr, the rest 30 minutes CES-D, DSM-IV; SCID/DSM-IV; 28.7% male PCP referral, no other involvement MMSS BDI, SF-12 62.3% white CIRSG, BSI - Anxiety Schmaling et al. (2002) T = 31††
C1 = 31
C2 = 3042.8 years old (SD = 10.7) MED
PlaceboTrained therapists with no further specification 6 sessions PST-PC, with first session 1 hr, others 30 minutes DSM-III-TR
PRIME-MD, HRSCHAM-D (17-item)
HSCL-D (20-item)39.1% male PCP referral, no other involvement 88.0% white Williams et al. (2000) T = 138
C1 = 137
C2 = 14071 years old (SD = 7.0), MED
PlaceboPhD Psychologists, Social workers, and Psychology Counselors 6 sessions PST-PC, with first session 1 hr, others 30 minutes DSM-III-R, HDRS
DSM-IV, PRIME-MDHSCL-D-20
HDRS58.5% male, 78.2% white PCP no involvement ↵* Sample size: T, treatment; T2, treatment 2 if applicable; C, control.
↵† Demographic: NR, not reported.
↵‡ Control: TAU, treatment as usual, W/NT, waitlist or no treatment; MED, medication; Placebo, placebo medication.
↵§ C1, medication paroxetine; C2, Placebo.
↵¶ Participants in the treatment group (68.7% ) received PST. Therefore, the authors believed the effect of intervention can be attributed to PST. Because sensitivity analysis that excluded this study did not alter the overall treatment effect, we included and presented this study in final analysis.
↵‖ AC, active control (health education video).
↵** Active control (stress management).
↵†† Specific breakdown of the numbers was not reported in article, thus assigned arbitrarily.
BSI, Brief Symptoms Inventory; CES-D, Center for Epidemiology Scale–Depression; DCS = depression care specialist; DFD; depression-free days; DHP-D-A, Duke Health Profile-Depression–Anxiety; EPDS, 10-item Edinburgh Postnatal Depression Scale; HAM-D, Hamilton Rating Scale for Depression; HADS, Hospital Anxiety and Depression Scale; HDRS, Hamilton Depression Rating Scale; HRSD, Hamilton Rating Scale for Depression; HSCL-D-20, Hopkins Depression self-report scale; MADRS, Montgomery-Åsberg Depression Rating Scale; MED, Medication Management; PCP, Primary Care Physician; PHQ-2, Patient Health Questionnaire, 2-item; PHQ-9, Patient Health Questionnaire, 9-item; PRIME-MD, Primary Care Evaluation of Mental Disorders; RDC, Research Diagnostic Criteria; SCL-20, Hopkins depression symptom checklist; SCL-90 depression, Hopkins Symptom Checklist—90 depression questions; SCID/DSM-IV, Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II); SF-12, SF-36 Health Survey 12-item version; TAU, Treatment as Usual; CIRSG, Cumulative Illness Rating Scale for Geriatrics.
Abbas M, Broadhead JC, Mbape P, Khumalo-Sakatukwa G. Defeating depression in the developing word: A Zimbabwean model. Br J Psychiatry 164(3):293–296.
Mynors-Wallis LM, Gath DH, Day A, Baker F. Randomised controlled trial of problem solving treatment, antidepressant medication, and combined treatment for major depression in primary care. BMJ 320:26–30.
Nezu A, Nezu C, Perri M. Problem-solving therapy for depression. New York: Wiley; 1989.
- Table 2.
PST for Treating Primary Care Patients' Depression and/or Anxiety; Results of Univariate Meta-regression
Parameter* Estimate 95%CI t (df) P Value Overall Effect (β0) 0.673 0.467 to 0.879 z = 6.41 .000 Depression (β0) 0.601 0.224 to 0.978 t (11) = 3.12 .007 Anxiety (β1) −0.249 −1.015 to 0.516 t (11) = −0.64 .317 Age† (β0) 0.696 0.477 to 0.915 t (10) = 6.23 .000 Age (β1) 0.020 0.007 to 0.033 t (10) = 2.97 .012 % Male (β0) −1.408 −2.161 to −0.655 t (10) = −3.66 .004 % Male (β1) 0.053 0.035 to 0.071 t (10) = 5.63 .000 % White (β0) 0.741 −0.030 to 1.511 t (7) = 1.88 .075 % White (β1) 0.001 −0.009 to 0.011 t (7) = 0.14 .381 % Married (β0) 0.398 0.066 to 0.729 t (5) = 2.35 .041 % Married (β1) 0.007 −0.013 to 0.026 t (5) = 0.66 .296 Individual (β0) 0.668 0.455 to 0.880 t (11) = 6.16 .000 Group (β1) 0.092 −0.769 to 0.954 t (11) = 0.21 .381 Family (β2) — — — In-person (β0) 0.722 0.494 to 0.950 t (10) = 6.22 .000 Tele-health (β1) −0.189 −0.846 to 0.469 t (10) = −0.56 .328 Combined (β2) — — — Session No. (β0) 0.465 −0.213 to 1.142 t (11) = 1.34 .157 Session No. (β1) 0.035 −0.074 to 0.144 t (11) = 0.63 .315 Min per session (β0) −0.005 −1.443 to 1.433 t (10) = −0.01 .389 Min per session (β1) 0.017 −0.018 to 0.052 t (10) = 0.96 .241 Master Level (β0) 1.569 1.181 to 1.957 t (9) = 7.92 .000 Doctoral Level (β1) −1.334 −2.112 to −0.557 t (9) = −3.36 .007 Multi-Discipline (β2) −1.280 −1.757 to −0.802 t (9) = −5.26 .000 No Physician (β0) 1.058 0.755 to 1.362 t (11) = 6.83 .000 Yes Physician (β1) −0.711 −1.124 to −0.298 t (11) = −3.38 .005 ↵* β0 should be interpreted as an intercept in a regression, that is the overall average (effect size) of the reference group. β1 should be interpreted as a regression coefficient in a regression, that is the difference (in effect size) between the reference group and the predicting group, noted as d(diff.) in the text for categorical variable (moderator). For cells with no numeric value, it was either because of missing data or not enough variation for a statistical estimate to be calculated.
↵† Participant age was mean-centered.
PST, problem-solving therapy.
- Table 3.
Results of Subgroup Analysis of Overall Treatment Effect (by Moderator) of PST for Treating Primary Care Patients' Depression and/or Anxiety
Parameter Estimate 95% CI t (df) P Value Depression 0.601 0.224 to 0.978 t (11) = 3.12 .007 Anxiety 0.352 −0.314 to 1.018 t (16) = 1.04 .226 Individual 0.668 0.455 to 0.880 t (11) = 6.16 .000 Group 0.760 −0.075 to 1.595 t (12) = 1.78 .085 Family — — — — In-person 0.722 0.494 to 0.950 t (10) = 6.22 .000 Tele-health 0.533 −0.083 to 1.150 t (11) = 1.70 .097 Combined — — — — Master level 1.569 1.181 to 1.957 t (9) = 7.92 .000 Doctoral level 0.235 −0.439 to 0.909 t (11) = 0.68 .304 Multi-discipline 0.290 −0.012 to 0.567 t (11) = 2.04 .056 Physician not involved 1.058 0.755 to 1.362 t (11) = 6.83 .000 Physician involved 0.347 0.068 to 0.627 t (12) = 2.43 .029 For cells with no numeric value, it was either because of missing data or not enough variation for a statistical estimate to be calculated.
CI, confidential interval; PST, problem-solving therapy.
- Table 4.
PST for Treating Primary Care Patients' Depression and/or Anxiety; Results of the Cochrane Collaboration's Tool for Assessing Risk of Bias*
Study/Year Random Sequence Generation Allocation Concealment Blinding of Participants and Personnel Blinding of Outcome Assessment Incomplete Outcome Data Selective Reporting Other Source of Bias Barrett et al. (2001) + + ? ? ? + + Chibanda et al. (2014) + ? ? ? ? + ? Katon et al. (2004) + + − + ? + − Lam et al. (2009) + + + ? ? + + Lynch et al. (2004) ? ? ? ? ? ? ? McCusker et al. (2008) + + ? ? ? + + Mynors-Wallis et al. (2000) − + + ? ? ? ? Oxman et al. (2008) + ? − ? ? + ? Reynolds et al. (2014) + + + + + + + Schmaling et al. (2002) + ? − − ? ? + Williams et al. (2000) + + ? ? ? ? + Number of “+”s 9 7 3 2 1 7 6 ↵* “+” = criteria were met in primary studies, thus no bias present; “?” = unclear whether or not criteria met from reading of primary studies; and “−” = criteria were not met in primary studies, thus bias present.
- Table 5.
Quality Assessment of Controlled PST Intervention Studies for Primary Care Patients' Depression and/or Anxiety (n=11)
Study/Year Good Fair Poor Barrett et al. (2001)41 ✓ Chibanda et al. (2014)42 ✓ Katon et al. (2004)43 ✓ Lam et al. (2009)44 ✓ Lynch et al. (2004)45 ✓ Mccusker et al. (2008)46 ✓ Mynors-Wallis et al. (2000)47 ✓ Oxman et al. (2008)48 ✓ Reynolds et al. (2014)49 ✓ Schmaling et al. (2002)50 ✓ Williams et al. (2000)51 ✓
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Global health reciprocal innovation to address mental health and well-being: strategies used and lessons learnt
- Psychologic Treatment of Depression Compared With Pharmacotherapy and Combined Treatment in Primary Care: A Network Meta-Analysis
- Brief behaviour change strategies for distressed patients in primary care
- Interventions Must Be Realistic to Be Useful and Completed in Family Medicine